Explain each and everything about the anterior abdominal wall with help of diagrams. I want each minor detail about that topic. Provide me so much detail so I don't have to read the book. Also explain the clinical correlates along the content
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the diagrams and comprehensive content. Let me compile the complete, detailed response.
The Anterior Abdominal Wall - Complete Guide
Source: Gray's Anatomy for Students, 4th ed.
1. Boundaries
The abdominal wall covers a large area bounded by:
- Superiorly: xiphoid process and costal margins
- Posteriorly: vertebral column
- Inferiorly: upper parts of the pelvic bones (pubic symphysis, pubic crests, iliac crests)
2. Layers of the Anterior Abdominal Wall
From superficial to deep, the wall has 7 layers:
- Skin
- Superficial fascia (Camper's + Scarpa's)
- Muscles and their aponeuroses (3 flat muscles + 2 vertical muscles)
- Deep (investing) fascia - transversalis fascia
- Extraperitoneal fascia
- Parietal peritoneum
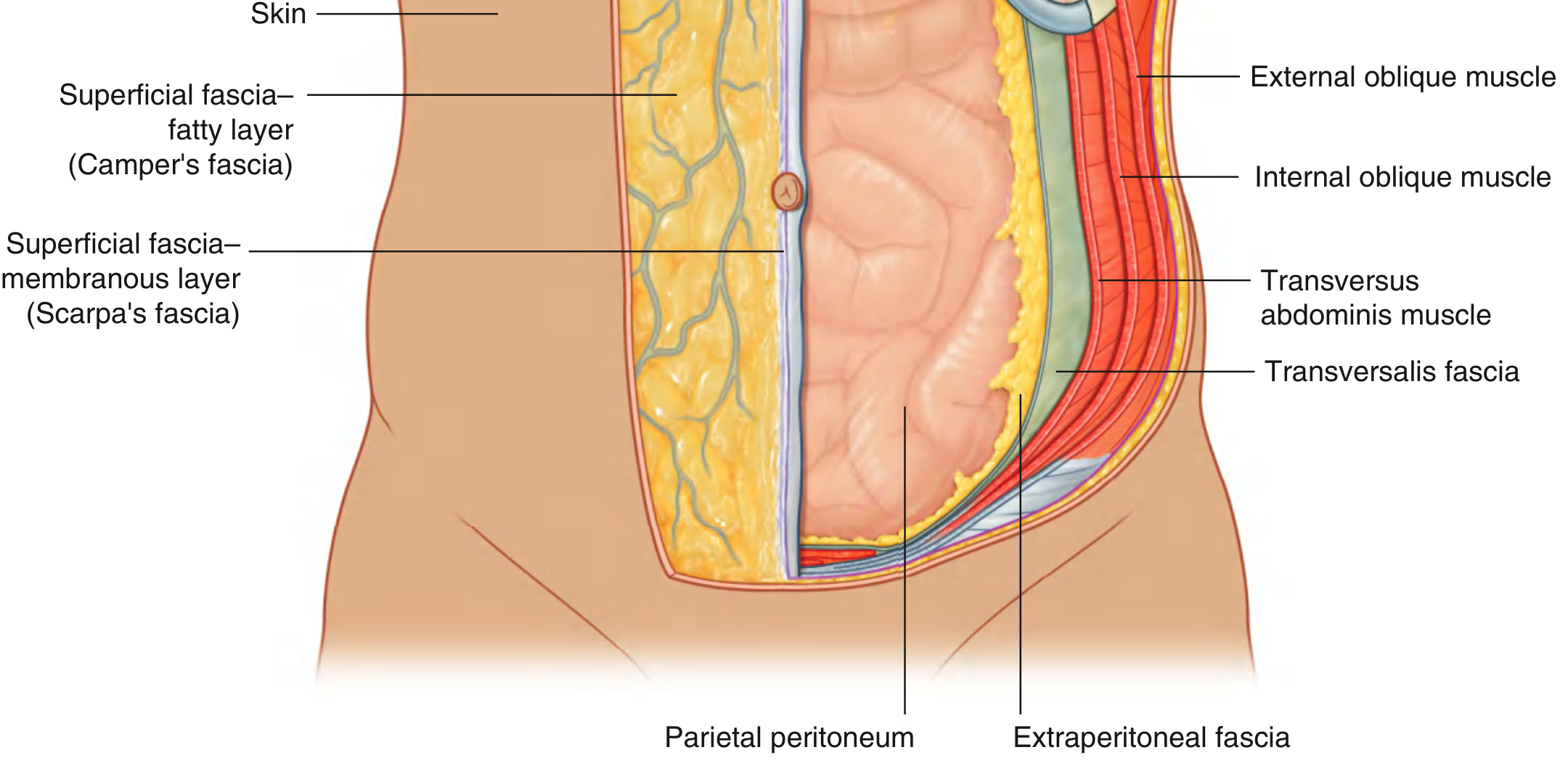
Fig. 1 - Layers of the Abdominal Wall (from Gray's Anatomy for Students)
3. Superficial Fascia (Subcutaneous Tissue)
Above the umbilicus the superficial fascia is a single fatty layer, continuous with fascia elsewhere. Below the umbilicus it splits into two distinct layers:
Camper's Fascia (Superficial Fatty Layer)
- Contains fat, variable in thickness
- Continuous over the inguinal ligament with superficial fascia of the thigh and perineum
- In men: continues over the penis, loses fat, fuses with Scarpa's fascia, then continues into the scrotum as the dartos fascia (contains smooth muscle - responsible for scrotal wrinkling)
- In women: retains fat, forms part of the labia majora
Scarpa's Fascia (Deeper Membranous Layer)
- Thin, membranous, contains little to no fat
- Important attachments:
- Midline: firmly attached to the linea alba and pubic symphysis
- Inferiorly: fuses with the deep fascia of the thigh (fascia lata) just below the inguinal ligament - this is a key surgical landmark
- In the perineum: becomes Colles' fascia (superficial perineal fascia), firmly attached to the ischiopubic rami and posterior margin of the perineal membrane
📌 Clinical Correlation - Pelvic Fracture/Urethral Rupture: When the urethra ruptures below the perineal membrane, urine tracks into the scrotum, penis, and up the anterior abdominal wall deep to Scarpa's fascia - but not into the thighs (because Scarpa's fuses with fascia lata below the inguinal ligament) and not into the perineum posteriorly (because Colles' fascia is attached to ischiopubic rami). This explains the classic "butterfly bruising" pattern seen in urethral injuries.
4. Muscles of the Anterior Abdominal Wall
There are 5 muscles in total - three flat lateral muscles and two vertical midline muscles.
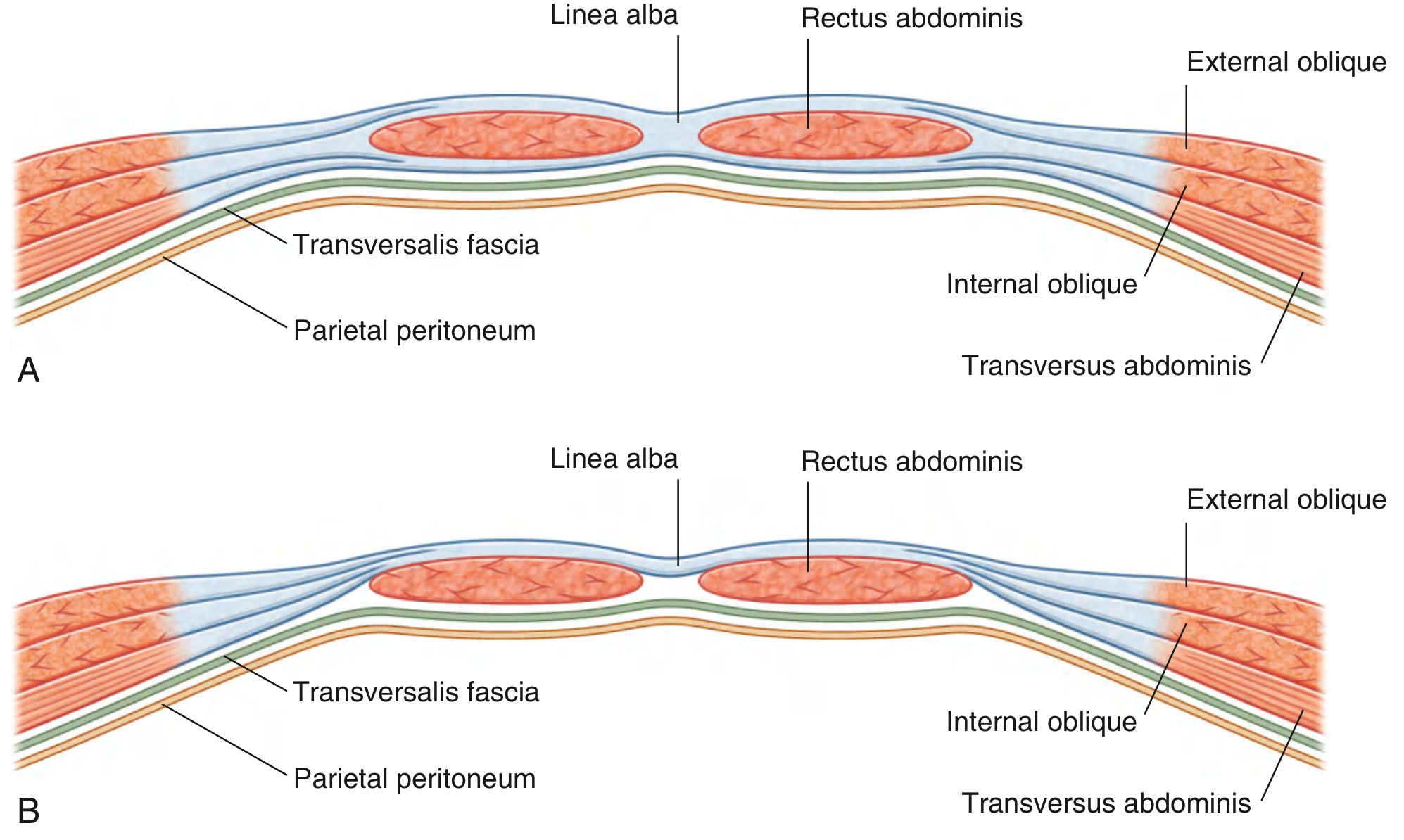
Fig. 2 - Organization of the Rectus Sheath. (A) Above arcuate line. (B) Below arcuate line.
4a. External Oblique
| Feature | Detail |
|---|---|
| Origin | Outer surfaces of the lower 8 ribs (ribs V-XII) as muscular slips |
| Insertion | Lateral lip of iliac crest; aponeurosis → linea alba |
| Innervation | Anterior rami T7-T12 (also T5 and T6 for upper portion) |
| Action | Compresses abdominal contents; both muscles flex trunk; each bends trunk ipsilaterally, rotates contralaterally |
Key features of the external oblique aponeurosis:
- Fibers run in a "hands-in-pockets" direction (inferiorly and medially)
- The lower free edge of the aponeurosis folds under on itself to form the inguinal ligament (from ASIS to pubic tubercle)
- The inguinal ligament forms the floor of the inguinal canal
- At its medial end, the inguinal ligament fans out as the lacunar ligament (attaches to the pectin pubis) - the medial most sharp edge of the lacunar ligament is the site where a femoral hernia becomes strangulated
- The superficial inguinal ring is a triangular defect in the aponeurosis, just above and lateral to the pubic tubercle
4b. Internal Oblique
| Feature | Detail |
|---|---|
| Origin | Thoracolumbar fascia; iliac crest (between external oblique and transversus origins); lateral 2/3 of inguinal ligament |
| Insertion | Inferior border of lower 3-4 ribs; aponeurosis → linea alba; pubic crest and pectineal line |
| Innervation | T7-T12 and L1 |
| Action | Compresses abdominal contents; flexes trunk; bends and rotates trunk to the same side |
Key features:
- Fibers run perpendicular to external oblique (superiorly and medially - "fan-shaped")
- Its aponeurosis splits at the lateral border of rectus abdominis to contribute to both anterior and posterior walls of the rectus sheath above the arcuate line
- Lowest fibers arch medially with transversus abdominis to form the conjoint tendon (falx inguinalis) which inserts into the pubic crest and pectineal line
- The cremaster muscle and fascia are derived from the internal oblique - they form the middle covering of the spermatic cord
4c. Transversus Abdominis
| Feature | Detail |
|---|---|
| Origin | Thoracolumbar fascia; medial lip of iliac crest; lateral 1/3 of inguinal ligament; costal cartilages of ribs VII-XII |
| Insertion | Aponeurosis → linea alba; pubic crest and pectineal line |
| Innervation | T7-T12 and L1 |
| Action | Compresses and supports abdominal contents |
Key features:
- The deepest of the flat muscles; fibers run transversely
- Its aponeurosis passes entirely posterior to the rectus abdominis above the arcuate line, then anterior below it
- The processus vaginalis passes under the arching fibers of transversus (unlike internal oblique), so the transversus does NOT contribute a covering to the spermatic cord
- The transversalis fascia (the deep fascia of transversus) forms the deepest covering of the spermatic cord - the internal spermatic fascia
4d. Rectus Abdominis
| Feature | Detail |
|---|---|
| Origin | Pubic crest, pubic tubercle, and pubic symphysis |
| Insertion | Costal cartilages of ribs V-VII; xiphoid process |
| Innervation | Anterior rami mainly T7-T12 |
| Action | Compresses abdominal contents; flexes vertebral column; tenses abdominal wall |
Key features:
- Long vertical strap muscle running parallel to the midline on either side of linea alba
- The muscle widens and thins as it ascends from pubis to costal margin
- Crossed by 3-4 tendinous intersections (fibrous bands) - these are fused to the anterior wall of the rectus sheath and are the basis of the "6-pack" in lean individuals
- The intersections do NOT go through the full thickness of the muscle - the posterior part has no attachment to the sheath
- Enclosed within the rectus sheath throughout its length
4e. Pyramidalis
| Feature | Detail |
|---|---|
| Origin | Front of pubis and pubic symphysis |
| Insertion | Into the linea alba |
| Innervation | Anterior ramus of T12 |
| Action | Tenses the linea alba |
- Small triangular muscle, anterior to the lower rectus abdominis
- May be absent in a significant percentage of people (absent in ~20%)
- Has no functional importance; used as a surgical landmark
5. The Rectus Sheath
The rectus sheath is an aponeurotic envelope formed by the interlacing aponeuroses of the three flat muscles. Its composition changes at the arcuate line.
Above the Arcuate Line (Upper 3/4)
- Anterior wall: aponeurosis of external oblique + anterior half of internal oblique aponeurosis
- Posterior wall: posterior half of internal oblique aponeurosis + aponeurosis of transversus abdominis
Below the Arcuate Line (Lower 1/4)
- Anterior wall: all three aponeuroses (external oblique + internal oblique + transversus abdominis) - all pass anterior to the rectus
- Posterior wall: absent - the rectus abdominis is in direct contact with the transversalis fascia
The arcuate line (semicircular line of Douglas) marks the transition point - located approximately midway between the umbilicus and pubic symphysis.
📌 Clinical Correlation - Rectus Sheath Hematoma: Tears of the inferior epigastric vessels or the rectus muscle itself (from trauma, straining, anticoagulation) cause bleeding within the confined rectus sheath. The hematoma tracks along the sheath but stops at the arcuate line because below it, the peritoneum is adherent. Presents as a painful abdominal mass that does NOT cross the midline, is tender on palpation, and tenses with muscle contraction (Carnett's test positive - the mass remains or increases when the patient raises their head, distinguishing it from intraabdominal causes).
6. Linea Alba and Linea Semilunaris
Linea Alba
- A fibrous band formed by the interlacing and fusion of the aponeuroses of all three flat muscles in the midline
- Runs from xiphoid process to pubic symphysis
- Wide above the umbilicus (about 2 cm) and narrows below it
- Contains the umbilicus (a scar from the obliterated umbilical cord)
- A relative weak point - site of epigastric hernias (protrusion of preperitoneal fat or peritoneal sac through defects in the linea alba)
Linea Semilunaris
- The curved line marking the lateral border of the rectus abdominis
- Visible on lean individuals as a curved groove lateral to the muscle
📌 Clinical Correlation - Epigastric Hernia: Small defects in the linea alba between the xiphoid and umbilicus allow preperitoneal fat to protrude. Common in middle-aged men. Usually presents as a small, tender midline nodule. Most contain only extraperitoneal fat without true peritoneal sac, unlike most hernias.
📌 Clinical Correlation - Diastasis Recti: Separation of the two rectus abdominis muscles with widening of the linea alba (>2 cm above umbilicus). Common post-pregnancy and in obesity. On straining, a midline bulge appears but it is NOT a true hernia (peritoneum is intact). The "bulge" is the abdominal contents pushing through the wide linea alba.
7. Deep Fascia - Transversalis Fascia
- The deep fascia investing the internal surface of the transversus abdominis muscle
- Lines the inside of the abdominal wall continuously
- At the deep inguinal ring, it forms a tubular evagination that becomes the internal spermatic fascia (deepest covering of spermatic cord)
- Important surgical layer in laparoscopic hernia repair (TAPP and TEP procedures work in the preperitoneal space between transversalis fascia and peritoneum)
8. Extraperitoneal (Preperitoneal) Fascia
- Connective tissue layer between transversalis fascia and parietal peritoneum
- Contains variable amounts of fat
- Subdivisions:
- Preperitoneal fascia (anterior) - contains the preperitoneal fat of the inguinal region, continuous with fat in the inguinal canal
- Retroperitoneal fascia (posterior) - around the kidneys and great vessels
- Site of the laparoscopic working space in TAPP/TEP hernia repair
9. Parietal Peritoneum
- Innermost layer of the abdominal wall
- Lines the entire abdominal cavity
- Closed sac in men; has two small openings in women (uterine tube ostia - clinically relevant as a route for ascending pelvic infections)
- Innervated by somatic nerves - pain from parietal peritoneum is well-localized, sharp, and worsens with movement (unlike visceral pain which is dull and poorly localized)
- On its internal surface over the lower anterior abdominal wall are several important peritoneal folds/fossae:
- Median umbilical fold: covers the median umbilical ligament (remnant of the urachus)
- Medial umbilical folds (paired): cover the medial umbilical ligaments (remnants of the umbilical arteries)
- Lateral umbilical folds (paired): cover the inferior epigastric vessels
📌 Clinical Correlation - Referred Appendicitis Pain: The parietal peritoneum is somatic; the visceral peritoneum covering the appendix is autonomic (T10). Initially, appendicitis causes poorly localized periumbilical pain (T10 dermatome). As inflammation extends to the parietal peritoneum, pain becomes localized to the RIF (McBurney's point). This classic migration of pain from periumbilical to RIF is a hallmark of acute appendicitis.
10. Innervation of the Anterior Abdominal Wall
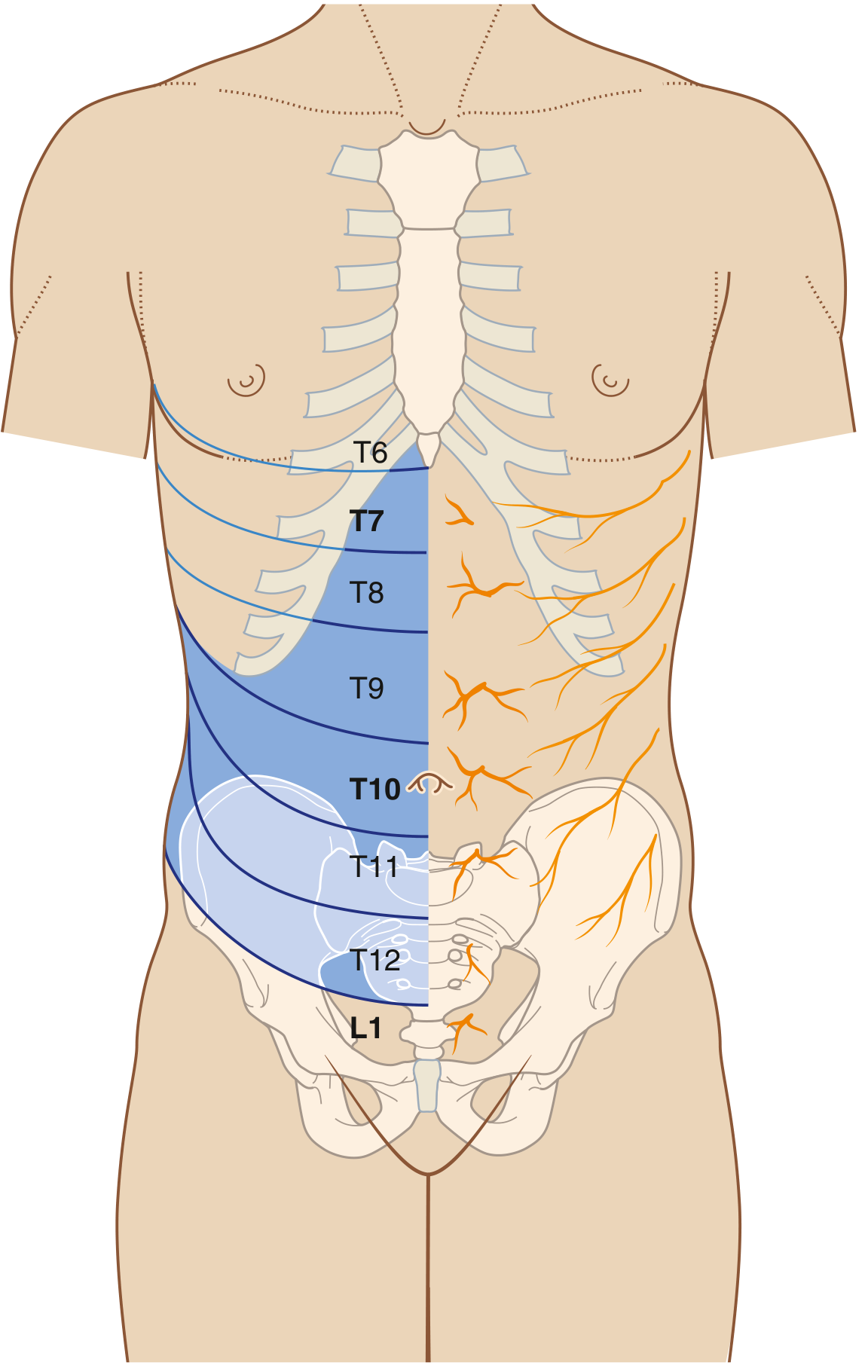
Fig. 3 - Innervation and Dermatomes of the Anterior Abdominal Wall
The skin, muscles, and parietal peritoneum of the anterolateral abdominal wall are supplied by T7-T12 and L1 spinal nerves.
Thoracic Nerves (T7-T12)
- The anterior rami pass around the body from posterior to anterior in an inferomedial direction
- Each gives off:
- A lateral cutaneous branch (divides into anterior and posterior branches)
- Ends as an anterior cutaneous branch
- T7-T11: intercostal nerves - leave their intercostal spaces and enter the abdominal wall
- T12: subcostal nerve
Key Dermatome Landmarks (MUST KNOW):
| Level | Landmark |
|---|---|
| T6 | Xiphoid process/infrasternal angle |
| T7 | Epigastric region |
| T8-T9 | Upper and mid abdomen |
| T10 | Umbilicus |
| T11 | Between umbilicus and inguinal ligament |
| T12 | Just above inguinal ligament |
| L1 | Inguinal and suprapubic regions (via iliohypogastric and ilio-inguinal nerves) |
L1 Nerves (from Lumbar Plexus):
Iliohypogastric nerve (L1):
- Enters abdominal wall through internal surface of transversus abdominis
- Passes between internal oblique and transversus abdominis
- Gives a lateral cutaneous branch to the buttock
- Ends as an anterior cutaneous branch to the suprapubic region
Ilio-inguinal nerve (L1):
- Enters abdominal wall through transversus abdominis
- Pierces the internal oblique
- Enters and traverses the inguinal canal
- Exits through the superficial inguinal ring
- Supplies skin of the medial thigh, anterior scrotum/labia majora, root of penis/mons pubis
📌 Clinical Correlation - Nerve Injury in Surgery: Appendectomy through a gridiron/McBurney's incision, inguinal hernia repair, and lower segment cesarean section can injure the iliohypogastric or ilio-inguinal nerves. This results in numbness/paresthesia in the inguinal and suprapubic regions, and in men, numbness of the ipsilateral scrotal skin.
📌 Clinical Correlation - Referred Pain to Testis: The testis descends from a position at L1, carrying its nerve supply (T10) with it. Ureteric colic from a stone at the ureteropelvic junction (L1 level) classically causes pain radiating to the ipsilateral testis or labium majus - because the testicular/ovarian nerve supply is T10 and L1.
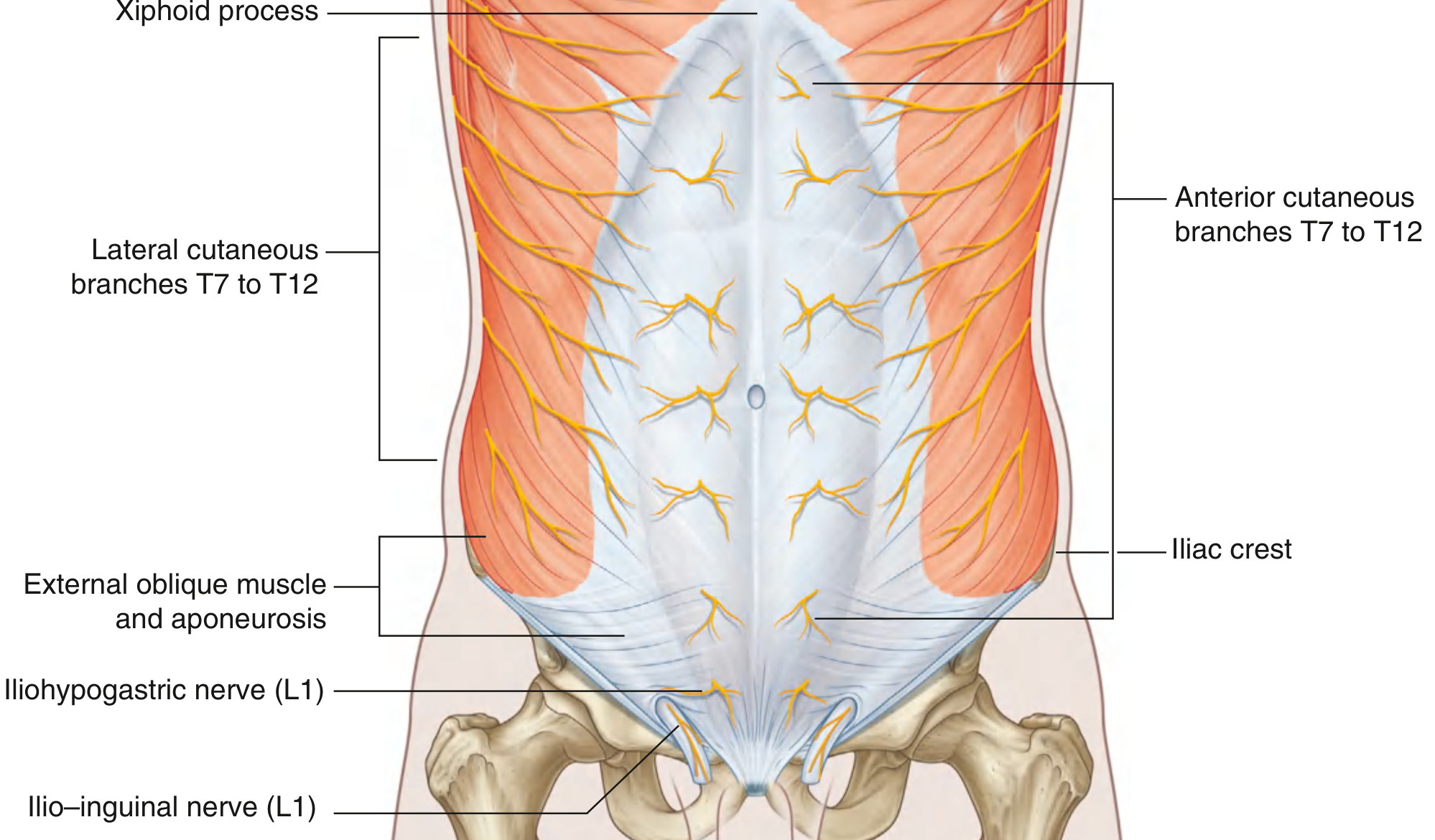
Fig. 4 - Innervation of the Anterolateral Abdominal Wall
11. Blood Supply
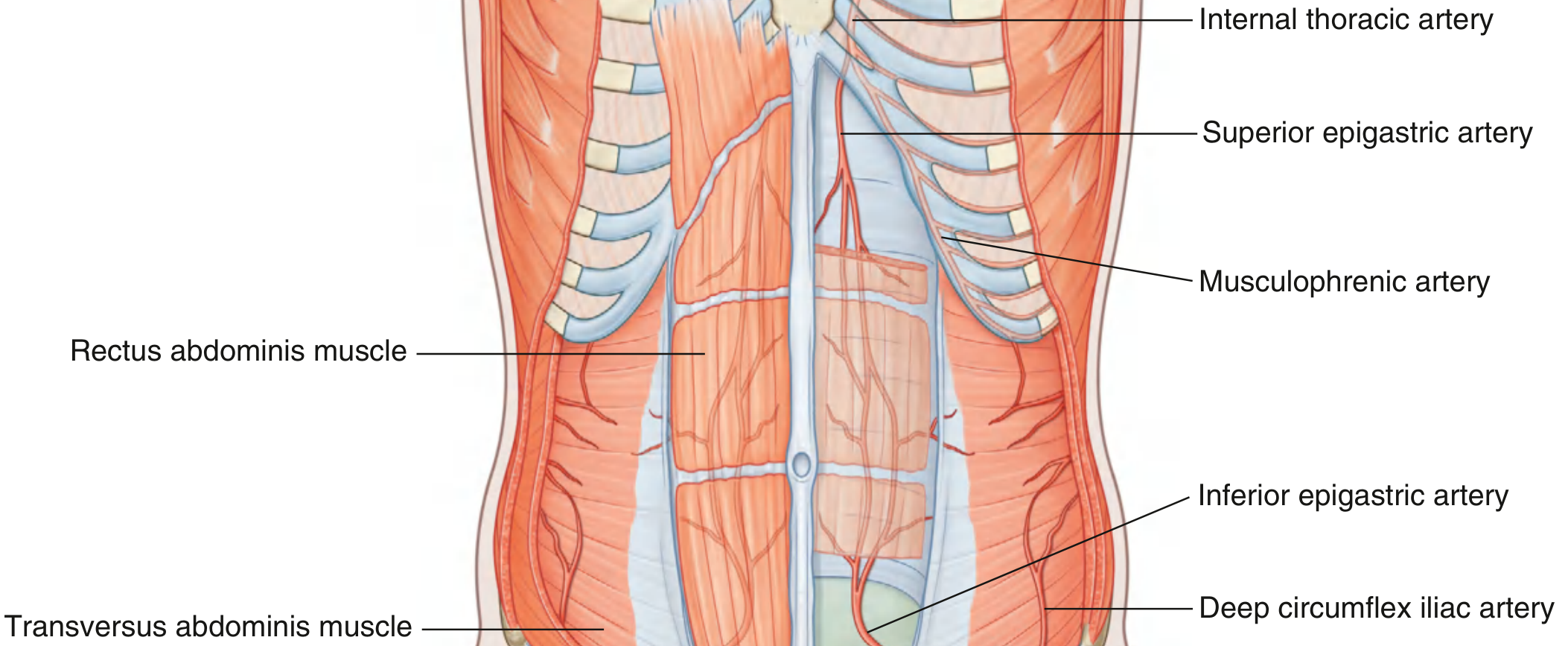
Fig. 5 - Arterial Supply to the Anterolateral Abdominal Wall
Superior Epigastric Artery
- Terminal branch of the internal thoracic artery (itself from the subclavian artery)
- Enters the rectus sheath from above
- Runs posterior to the rectus abdominis muscle
- Anastomoses with the inferior epigastric artery within the rectus sheath
Inferior Epigastric Artery
- Branch of the external iliac artery (just before it becomes the femoral artery)
- Ascends medially in the extraperitoneal fascia
- Passes medial to the deep inguinal ring
- Enters the rectus sheath from below, running posterior to rectus abdominis
- Anastomoses with the superior epigastric artery
- Lateral to deep inguinal ring (key landmark for distinguishing direct vs indirect hernia)
Musculophrenic Artery
- The other terminal branch of internal thoracic artery
- Supplies the lower intercostal spaces and parts of the diaphragm
Deep Circumflex Iliac Artery
- Branch of the external iliac artery
- Runs along the inguinal ligament to supply the lateral wall
Superficial Arteries
- Superficial epigastric artery: branch of femoral, runs upward toward the umbilicus
- Superficial circumflex iliac artery: branch of femoral
- Superficial external pudendal arteries: branches of femoral
Venous Drainage
- Veins follow the arteries
- Clinically important: the paraumbilical veins connect the portal system (via the round ligament of the liver) with the superficial veins of the abdominal wall (via the superficial epigastric and lateral thoracic veins) - this is the basis of caput medusae
📌 Clinical Correlation - Caput Medusae: In portal hypertension, blood shunts from the portal vein → paraumbilical veins → superficial abdominal veins. This causes dilated, visible veins radiating from the umbilicus ("caput medusae" - head of Medusa). The flow in these veins is away from the umbilicus in all directions (distinguishing it from IVC obstruction where flow above the umbilicus goes upward and below the umbilicus also goes upward).
📌 Clinical Correlation - TRAM Flap (Transverse Rectus Abdominis Myocutaneous): Breast reconstruction surgeons base this flap on either the superior epigastric artery (pedicled) or inferior epigastric artery (free flap). Understanding the anastomosis between superior and inferior epigastric arteries within the rectus sheath is essential for flap planning.
12. Lymphatic Drainage
- Superficial lymphatics ABOVE the umbilicus → drain superiorly to axillary nodes
- Superficial lymphatics BELOW the umbilicus → drain inferiorly to superficial inguinal nodes
- Deep lymphatics follow the deep arteries back to:
- Parasternal nodes (along internal thoracic artery)
- Lumbar nodes (along the abdominal aorta)
- External iliac nodes (along the external iliac artery)
📌 Clinical Correlation - Umbilical Metastases (Sister Mary Joseph Nodule): Malignancies from the stomach, pancreas, colon, or ovary can metastasize to the umbilical lymph nodes via deep lymphatics, producing a hard umbilical nodule (Sister Mary Joseph nodule). The umbilicus communicates with intraabdominal structures through the round ligament of the liver and paraumbilical vessels.
13. The Groin (Inguinal Region)
The groin is the junction between the anterior abdominal wall and the thigh. It is inherently weak due to developmental changes.
Developmental Basis of Weakness
- During development, the gonads descend from the posterior abdominal wall
- Before descent, a peritoneal outpouching (processus vaginalis) projects through the layers of the anterior abdominal wall
- The processus vaginalis acquires coverings from each layer it passes through:
- Transversalis fascia → internal spermatic fascia
- Internal oblique muscle → cremasteric fascia and muscle
- Aponeurosis of external oblique → external spermatic fascia
- Note: NO covering from transversus abdominis (it passes under the arching fibers)
- This track through the wall is the inguinal canal
14. The Inguinal Canal
A slit-like passage about 4 cm long running downward and medially, just above and parallel to the lower half of the inguinal ligament.
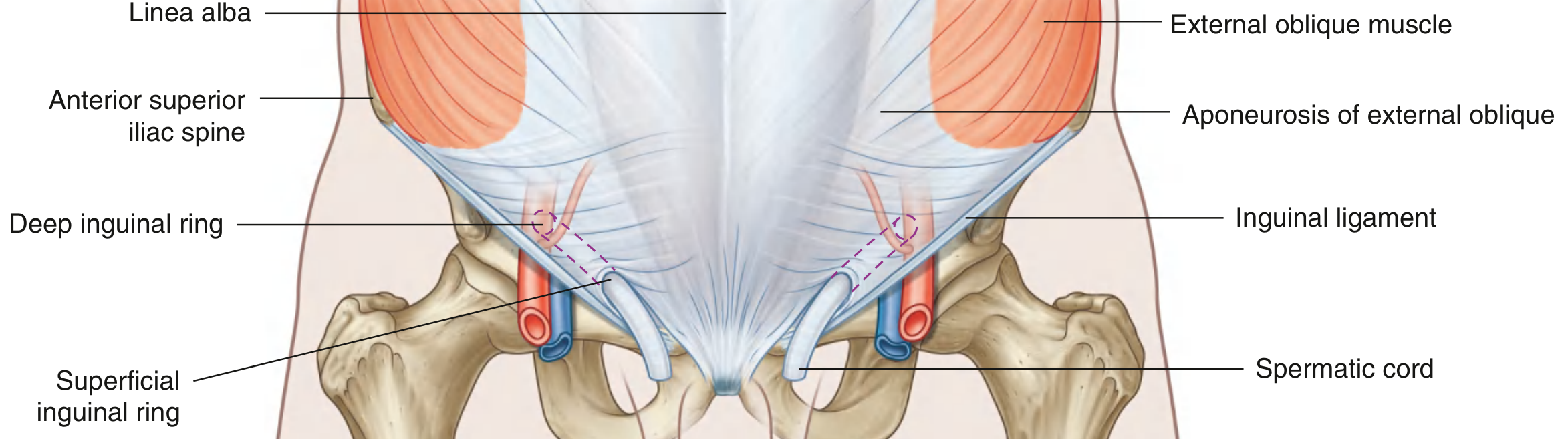
Fig. 6 - Inguinal Canal: Deep and Superficial Rings
Openings:
Deep (Internal) Inguinal Ring:
- Beginning of the canal
- Located at a point midway between ASIS and pubic symphysis (i.e., at the mid-inguinal point)
- Just above the inguinal ligament and immediately lateral to the inferior epigastric vessels
- Formed by the evagination of the transversalis fascia
- Has a "sling" formed by the transversalis fascia which tightens around the ring when intraabdominal pressure rises (valve mechanism)
Superficial (External) Inguinal Ring:
- End of the canal, triangular opening in the aponeurosis of external oblique
- Located above and lateral to the pubic tubercle
- Apex points superolaterally; base formed by pubic crest
- Medial crus: attached to pubic symphysis
- Lateral crus: attached to pubic tubercle
- Apex held together by intercrural fibers (prevent further widening)
Walls of the Inguinal Canal:
| Wall | Formation |
|---|---|
| Anterior wall | Aponeurosis of external oblique (along entire length); reinforced laterally by internal oblique (which arises from the inguinal ligament) |
| Posterior wall | Transversalis fascia (along entire length); reinforced medially by the conjoint tendon |
| Roof (superior wall) | Arching fibers of internal oblique and transversus abdominis |
| Floor (inferior wall) | Medial half of inguinal ligament; reinforced medially by lacunar ligament |
Contents of the Inguinal Canal:
In Men:
- Spermatic cord
- Ductus deferens (vas deferens)
- Testicular artery (from aorta, at L2)
- Pampiniform plexus of veins
- Cremasteric artery and vein
- Artery to vas deferens (from inferior vesical artery)
- Genital branch of genitofemoral nerve (motor to cremaster; sensory to scrotal skin)
- Autonomic nerves
- Lymphatics
- Ilio-inguinal nerve (L1) - passes through the canal but is NOT technically in the spermatic cord; exits through the superficial ring alongside it
In Women:
- Round ligament of the uterus (remnant of the gubernaculum)
- Genital branch of the genitofemoral nerve
- Ilio-inguinal nerve
Coverings of the Spermatic Cord (3 layers, acquired during passage through the canal):
| Covering | Derived From |
|---|---|
| 1. External spermatic fascia (outermost) | Aponeurosis of external oblique (at superficial ring) |
| 2. Cremasteric fascia and cremaster muscle | Internal oblique muscle |
| 3. Internal spermatic fascia (deepest) | Transversalis fascia (at deep ring) |
📌 Clinical Correlation - Cremasteric Reflex: Stroking the inner thigh (L1 afferent via ilio-inguinal nerve) → reflex contraction of cremaster muscle (L1 efferent via genital branch of genitofemoral nerve) → testicular elevation. Active in children, diminishes with age. Loss of reflex: cord lesion at L1, or testicular torsion (though not reliable enough alone for diagnosis of torsion).
📌 Clinical Correlation - Varicocele: Dilation of the pampiniform plexus. 90% are left-sided because the left testicular vein drains at 90° into the left renal vein (higher pressure, longer course), while the right drains obliquely into the IVC. A sudden-onset right-sided varicocele in an older man should raise suspicion for RCC invading the right renal vein or a retroperitoneal mass compressing the IVC.
15. Inguinal Hernias
An inguinal hernia is the protrusion of a peritoneal sac (with or without abdominal contents) through a weakened part of the abdominal wall in the groin.
Indirect Inguinal Hernia
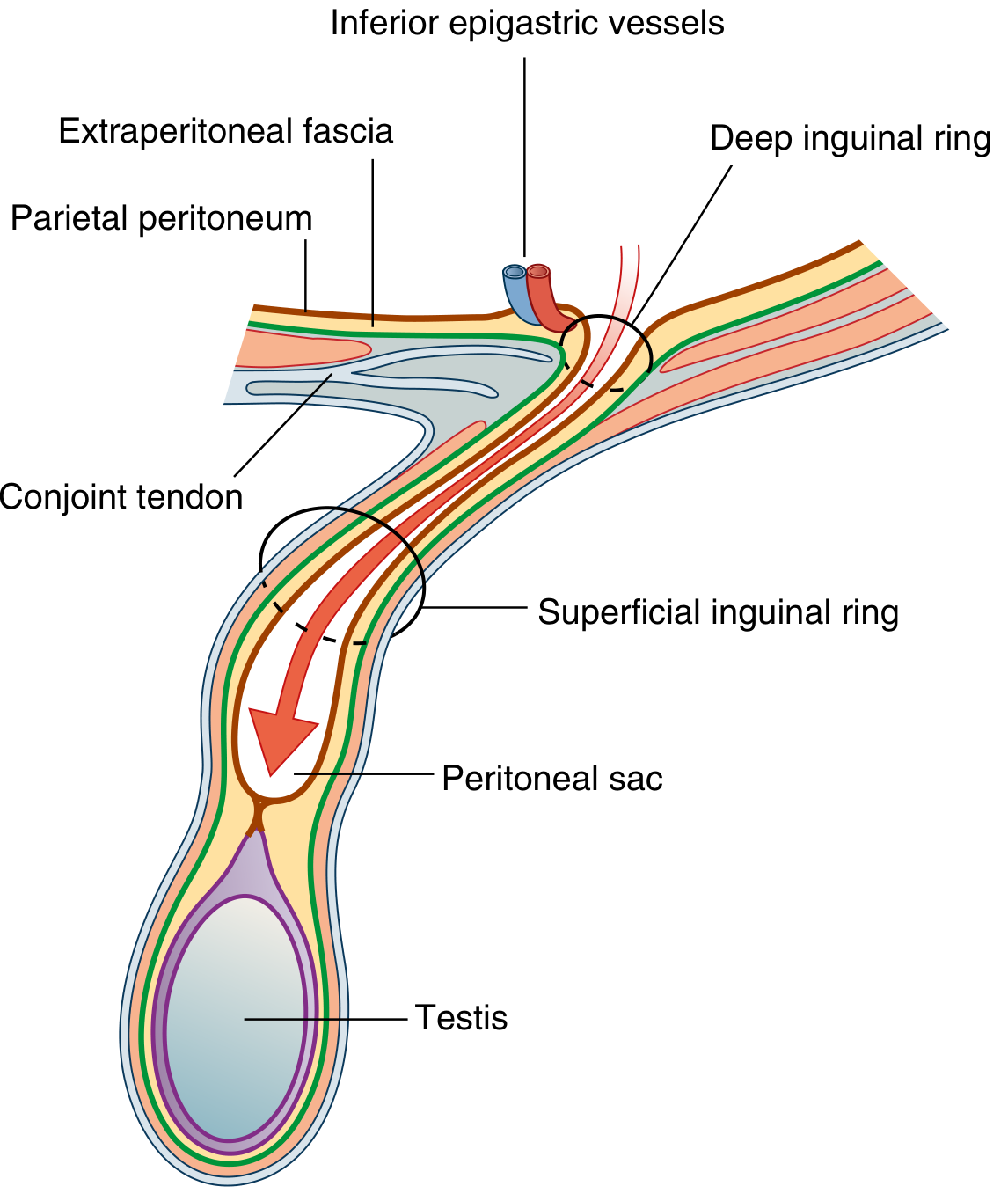
Fig. 7 - Indirect Inguinal Hernia
- Most common type of inguinal hernia
- Much more common in men than women
- Congenital in origin - due to persistence/patency of the processus vaginalis
- The peritoneal sac enters through the deep inguinal ring (lateral to inferior epigastric vessels) → traverses the inguinal canal → exits through the superficial ring
- In men, may extend into the scrotum
- The sac is covered by all three spermatic cord coverings
- Because it enters through the deep inguinal ring, it is lateral to the inferior epigastric vessels
- To confirm: apply pressure at the deep inguinal ring and ask patient to cough - hernia is controlled
Direct Inguinal Hernia
- Less common; acquired (not congenital)
- Caused by weakening of the posterior wall of the inguinal canal (transversalis fascia)
- The peritoneal sac protrudes directly through the posterior wall of the inguinal canal (through Hesselbach's triangle) - medial to the inferior epigastric vessels
- Does NOT enter through the deep ring
- Rarely extends into the scrotum
- More common in elderly men with weak abdominal muscles
Hesselbach's Triangle (Inguinal Triangle):
Bounded by:
- Medially: lateral border of the rectus abdominis
- Laterally: inferior epigastric vessels
- Inferiorly: inguinal ligament
Direct hernias protrude through this triangle. Indirect hernias arise lateral to this triangle.
Key Clinical Distinction (Indirect vs Direct):
| Feature | Indirect | Direct |
|---|---|---|
| Entry point | Deep inguinal ring (lateral to inf. epigastric a.) | Posterior wall of canal (medial to inf. epigastric a.) |
| Hesselbach's triangle | Outside (lateral) | Inside |
| Age | Any age, congenital | Older adults |
| Scrotal extension | Common | Rare |
| Control at deep ring | Yes | No (hernia pops back without control at ring) |
| Associated | Patent processus vaginalis | Weakness of posterior wall |
📌 Clinical Correlation - Strangulated Hernia: When the neck of the hernia sac is tight, the blood supply to the bowel within the sac is cut off. This constitutes a surgical emergency. The patient has a tense, tender, irreducible groin swelling with signs of intestinal obstruction. Delay leads to bowel ischemia, perforation, and peritonitis. Indirect hernias strangulate more often than direct ones (due to tight deep ring).
📌 Clinical Correlation - Inguinal vs Femoral Hernia: Inguinal hernias appear above and medial to the pubic tubercle; femoral hernias appear below and lateral to the pubic tubercle (through the femoral canal). Femoral hernias are more common in women, smaller, and strangulate more readily due to rigid femoral ring margins.
16. The Femoral Canal (Brief)
Though technically at the junction with the thigh, the femoral canal is intimately related to the lower anterior abdominal wall:
- The femoral canal is the medial compartment of the femoral sheath
- Located below the inguinal ligament, medial to the femoral vein
- Bounded medially by the lacunar ligament (whose sharp edge can strangulate a femoral hernia)
- Normally contains lymph nodes (Cloquet's node) and loose areolar tissue
- Represents a potential space through which a femoral hernia protrudes
17. Surface Anatomy and Abdominal Quadrants/Regions
4-Quadrant Division:
- Right Upper Quadrant (RUQ): liver, gallbladder, right kidney, ascending colon, hepatic flexure
- Left Upper Quadrant (LUQ): stomach, spleen, left kidney, descending colon, splenic flexure, pancreas tail
- Right Lower Quadrant (RLQ): appendix, cecum, right ureter
- Left Lower Quadrant (LLQ): sigmoid colon, left ureter, left ovary (women)
9-Region Division (for more precise localization):
- Epigastric (midline, upper): stomach, liver, duodenum, pancreas
- Umbilical (central): transverse colon, small bowel loops
- Hypogastric/pubic (midline, lower): bladder, uterus, sigmoid colon
- Right/Left hypochondriac regions (lateral, upper): liver, kidney, splenic flexure
- Right/Left lumbar/flank regions (lateral, middle): ascending/descending colon
- Right/Left iliac (inguinal) regions (lateral, lower): cecum/appendix (right), sigmoid/ovary (left)
18. Summary Table: All 5 Muscles
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| External oblique | Lower 8 ribs (V-XII) outer surfaces | Iliac crest; linea alba (via aponeurosis) | T7-T12 | Compress abdomen; trunk flexion; ipsilateral lateral flexion; contralateral rotation |
| Internal oblique | Thoracolumbar fascia; iliac crest; lat. 2/3 inguinal lig. | Lower 3-4 ribs; linea alba; pubic crest | T7-T12 + L1 | Compress abdomen; trunk flexion; ipsilateral rotation |
| Transversus abdominis | Thoracolumbar fascia; iliac crest; lat. 1/3 inguinal lig.; ribs VII-XII costal cartilages | Linea alba; pubic crest | T7-T12 + L1 | Compress abdomen |
| Rectus abdominis | Pubic crest, tubercle, symphysis | Costal cartilages V-VII; xiphoid | T7-T12 | Compress abdomen; flex vertebral column |
| Pyramidalis | Front of pubis, pubic symphysis | Linea alba | T12 | Tense linea alba |
19. Key Clinical Correlates - Summary
| Condition | Anatomical Basis |
|---|---|
| Rectus sheath hematoma | Injury to inferior epigastric vessels within rectus sheath; limited by sheath; Carnett's test positive |
| Indirect inguinal hernia | Patent processus vaginalis; enters deep inguinal ring lateral to inferior epigastric vessels |
| Direct inguinal hernia | Weakness of posterior wall; protrudes through Hesselbach's triangle medial to inferior epigastric vessels |
| Femoral hernia | Through femoral canal below inguinal ligament; strangulates at rigid lacunar ligament edge |
| Urethral rupture urine tracking | Urine tracks in Scarpa's fascia space (fuses with fascia lata = no thigh spread; attached posteriorly = no posterior perineum spread) |
| Epigastric hernia | Defect in linea alba between xiphoid and umbilicus; contains preperitoneal fat |
| Caput medusae | Portal hypertension → flow through paraumbilical veins to superficial abdominal veins |
| Cremasteric reflex loss | Spinal cord injury at L1, or testicular torsion (though non-specific) |
| Varicocele (left > right) | Left testicular vein drains at 90° into left renal vein; suspect malignancy with sudden right varicocele |
| Sister Mary Joseph nodule | Umbilical metastasis from GI/ovarian malignancy via deep lymphatics/peritoneal seeding |
| Nerve injury in hernia repair | Ilio-inguinal + iliohypogastric nerves at risk; causes scrotal/labial and suprapubic numbness |
| Diastasis recti | Widening of linea alba >2 cm; not a true hernia; common post-partum |
All content sourced from Gray's Anatomy for Students, 4th Edition - the comprehensive gold standard for clinical anatomy.
This is a shared conversation. Sign in to Orris to start your own chat.