Routes of spread of cholesteatoma and theories of etiopathogenesis 10 marks answer for ms ent exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I have everything needed. Now I'll write the comprehensive MS ENT exam answer.
Cholesteatoma: Theories of Etiopathogenesis and Routes of Spread
(10-mark answer)
DEFINITION
A cholesteatoma is a collection of keratinizing stratified squamous epithelium within the middle ear cleft that is associated with progressive resorption/erosion of adjacent bony structures. It may be congenital or acquired (acquired accounts for ~98% of cases). - Cummings Otolaryngology, p. 2684
CLASSIFICATION
| Type | Origin |
|---|---|
| Congenital | Epidermoid cell rests within temporal bone, present at birth |
| Primary acquired | Invagination/retraction of TM (no prior perforation) |
| Secondary acquired | Ingrowth via existing TM perforation or iatrogenic implantation |
PART A: THEORIES OF ETIOPATHOGENESIS
1. Invagination / Retraction Pocket Theory (Most Accepted)
Proposed by: Wittmaack (1933); supported by Sade and numerous experimental studies.
Mechanism:
- Eustachian tube (ET) dysfunction leads to hypoventilation of the middle ear cleft
- Persistent negative middle ear pressure ("ex vacuo") causes the pars flaccida (which is less fibrous and less rigid) to retract inward
- The retraction pocket deepens progressively; at a critical depth, desquamated keratin can no longer self-migrate out of the pocket
- Keratin accumulates, bacteria colonize the keratin matrix forming biofilms, and a cholesteatoma results
- An atrophic or thinned TM (from previous AOM/OME) is especially susceptible
Evidence supporting:
- Eustachian tube obstruction in animal models produces drum retraction and cholesteatoma
- Higher incidence in cleft palate patients (poor ET function)
- Retraction pockets are recognized clinically as precursor lesions
- Selective epitympanic dysventilation syndrome (Palva) and the Sudhoff-Tos combined retraction + basal hyperplasia model are variants of this theory
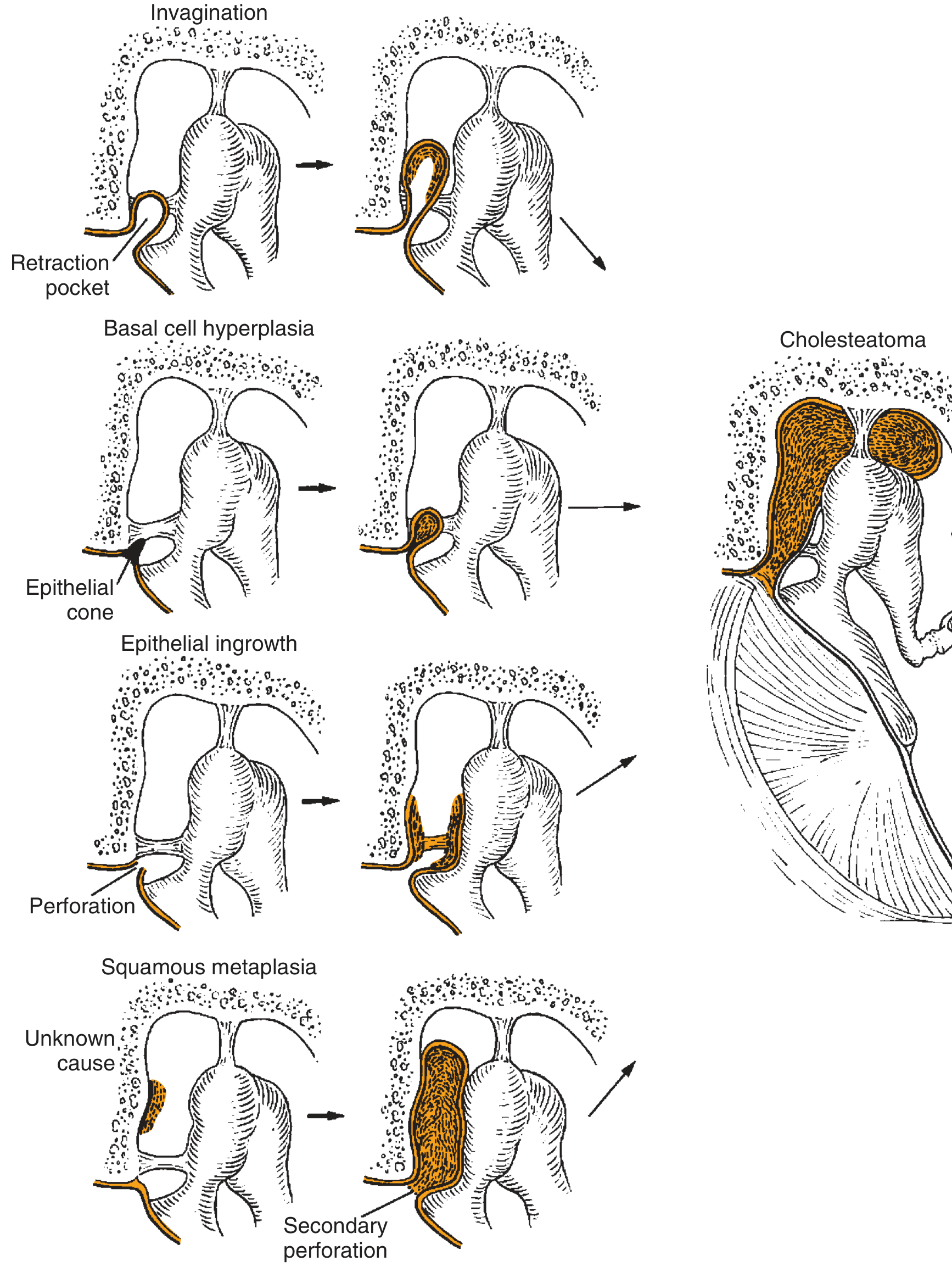
Fig. 140.11 - Cummings Otolaryngology: Four theories of cholesteatoma pathogenesis
2. Epithelial Invasion / Immigration Theory (Migration Theory)
Proposed by: Habermann (1888) and Bezold; supported by Van Blitterswijk, Palva, and Jackson.
Mechanism:
- Keratinizing squamous epithelium from the external auditory canal or outer surface of the TM migrates inward through the margins of a pre-existing tympanic membrane perforation (usually posterosuperior marginal)
- The inner mucosal lining of the TM is damaged by inflammation, losing its barrier function
- The outer keratin epithelium then migrates in by "contact guidance" along exposed connective tissue surfaces
- This produces a secondary acquired cholesteatoma, located medial to the ossicular chain
Evidence supporting:
- CK-10 (cytokeratin 10, a marker of meatal epidermis) is preferentially expressed in cholesteatoma matrix
- Animal studies (Jackson and Lim) showed keratinizing epithelium can migrate into cat bulla by contact guidance
- Temporal bone fractures allowing ingrowth of EAC epithelium - Cummings, p. 2686
3. Basal Cell Hyperplasia / Papillary Ingrowth Theory
Proposed by: Lange (1925); supported by Ruedi (1958).
Mechanism:
- Epithelial "prickle cells" (basal keratinocytes) of the pars flaccida invade the subepithelial connective tissue via proliferating columns/cones of epithelium ("epithelial cones")
- For this invasion, the basement membrane (basal lamina) must be disrupted - such disruptions have been documented in human and animal cholesteatomas
- Microcholesteatomas form behind an intact TM and then secondarily perforate
- Propylene glycol instillation into chinchilla middle ear induces this process experimentally
Molecular evidence supporting:
- Overexpression of CK-13 and CK-16 (hyperproliferation markers)
- Increased EGF receptor expression
- Elevated fibronectin and tenascin (extracellular matrix disruption)
- Increased ICAM-1/ICAM-2 (cell migration facilitators)
- Presence of heat shock proteins 60 and 70
- Langerhans cells promoting keratinocyte proliferation via IL-1α and TGF-β
- Caspase-8/caspase-3 activation leading to accelerated apoptosis - Cummings, p. 2687
4. Squamous Metaplasia Theory
Proposed by: Wendt (1873).
Mechanism:
- Simple squamous or cuboidal epithelium of the middle ear mucosal lining undergoes metaplastic transformation into keratinizing stratified squamous epithelium in response to chronic inflammation/infection
- The resulting keratinizing area enlarges due to debris accumulation, forming a pearl-like cyst
- With intercurrent infection, the cholesteatoma leads to secondary TM perforation, producing the classic appearance
Evidence for/against:
- Islands of keratinizing epithelium found in biopsies from children with OME (supports)
- No convincing human or animal model support; considered the least accepted theory - Cummings, p. 2687
5. Mucosal Traction Theory (Newest)
Proposed by: Jackler and colleagues (2015).
Mechanism:
- Opposing mucosal surfaces on the medial TM and lateral ossicles become adherent
- Mucociliary clearance propels these adherent surfaces upward into the attic, pushing the pars flaccida inward
- Net epithelial cell migration and adhesive forces from trapped mucus further deepen the retraction pocket
- This theory proposes a more active mechanical role for the mucosa in cholesteatoma genesis
Challenged by: Pauna et al., who found ciliated cells are actually rarer in ears with cholesteatoma than in controls, arguing against the ciliary mechanism - Cummings, p. 2687-2688
Congenital Cholesteatoma - Etiopathogenesis
- Michaels (1986) described an "epidermoid formation" - a small area of keratinizing epithelium in the anterior tympanum of fetuses at 10-33 weeks' gestation (found in 37/68 temporal bones)
- These embryonic epithelial cell rests normally regress; if they persist and expand, keratinous material accumulates forming a congenital cholesteatoma, typically in the anterior middle ear
- Diagnosed by the presence of: white mass behind intact TM, no prior history of otorrhea/perforation/surgery - Scott-Brown's Vol 2, p. 200
PART B: ROUTES OF SPREAD
The routes of spread are determined by the mucosal folds, ossicular ligaments, and bony architecture of the middle ear. They follow predictable anatomical pathways - understanding these is essential for surgical clearance.
Starting Point: Prussak's Space
Most primary acquired cholesteatomas begin in Prussak's space (lateral epitympanic space), the space between:
- Laterally: pars flaccida of TM
- Medially: neck and head of malleus
- Superiorly: lateral malleolar fold
From Prussak's space, spread occurs in four main directions:
Route 1: Posterosuperior (Most Common)
Prussak's space → Posterior epitympanum → Aditus ad antrum → Mastoid antrum → Mastoid air cells
- The cholesteatoma spreads posteriorly through a posterior opening in the epitympanum
- Enters the posterior epitympanum lateral to the body of the incus
- Travels through the aditus ad antrum
- Reaches the mastoid antrum and progressively erodes mastoid air cell walls, forming a single large cavity
Route 2: Inferior - Into Mesotympanum
Prussak's space → Pouch of von Tröltsch → Mesotympanum → Hypotympanum
- Spreads inferiorly through the lateral pouch of von Tröltsch (anterior and posterior)
- Enters the mesotympanum proper
- Can extend to the hypotympanum (inferior to the annulus)
- Here, it may threaten the jugular bulb
Route 3: Anterior - Supratubal Route
Prussak's space → Anterior epitympanum → Supratubal recess (supraTubal recess) → Eustachian tube region
- Extends anteriorly into the anterior epitympanic space (anterior to the malleus head/neck)
- Enters the supratubal recess (STR) - a bony cul-de-sac above the ET opening
- Here it threatens the geniculate ganglion and first genu of the facial nerve, which lie just medial to the STR
- The "cog" (bony septum based on the tegmen) must be removed surgically to visualize the STR - Cummings, p. 2613
Route 4: Medial Extension (Advanced Disease)
- Advanced disease extends medial to the ossicles (lateral chain displaced medially by pars flaccida cholesteatoma)
- Reaches the medial wall of the tympanic cavity: threatens the oval window, round window niche, and otic capsule
- Most common site of labyrinthine fistula: horizontal (lateral) semicircular canal (ampullated limb)
- Rarely: cochlear fistula
Bony Erosions and Structures Threatened
| Structure Eroded | Consequence |
|---|---|
| Scutum (lateral attic wall) | Pathognomonic finding on CT |
| Long process of incus | Most commonly eroded ossicle - conductive hearing loss |
| Stapes superstructure | Conductive hearing loss |
| Tegmen tympani / mastoideum | Brain herniation, CSF leak, extradural abscess |
| Fallopian canal (tympanic segment) | Facial nerve paralysis (acute or insidious) |
| Lateral semicircular canal | Labyrinthine fistula - vertigo, SNHL |
| Sinus plate (sigmoid sinus) | Lateral sinus thrombophlebitis |
| Posterior canal wall | Leads to formation of "natural" cavity |
Summary: BOX - Complications Arising from Routes of Spread
(From Cummings Otolaryngology, Box 140.1)
- Conductive, sensorineural, or mixed hearing loss
- Labyrinthine fistula (mainly horizontal SCC, rarely cochlea)
- Facial nerve paralysis (acute or chronic)
- Intracranial infections (meningitis, brain abscess, extradural abscess)
- Brain herniation or CSF leakage (tegmen erosion)
- Lateral sinus thrombophlebitis
SUMMARY TABLE
| Theory | Mechanism | Type of Cholesteatoma |
|---|---|---|
| Invagination (Wittmaack) | ET dysfunction → retraction pocket | Primary acquired |
| Migration (Habermann) | Epithelial ingrowth via perforation | Secondary acquired |
| Basal cell hyperplasia (Lange/Ruedi) | Epithelial cones invade through disrupted BM | Primary acquired |
| Squamous metaplasia (Wendt) | ME mucosa → keratinizing epithelium | Primary acquired |
| Mucosal traction (Jackler) | Mucociliary force propels TM into attic | Primary acquired |
| Epidermoid cell rests (Michaels) | Persistence of fetal epithelial rests | Congenital |
Sources: Cummings Otolaryngology Head & Neck Surgery (Ch. 140, pp. 2684-2688); Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2 (Ch. 82, pp. 199-200); Shambaugh Surgery of the Ear (pp. 292-293)
This is a shared conversation. Sign in to Orris to start your own chat.