Pleura
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive content from Gray's Anatomy for Students, Color Atlas of Human Anatomy, Ganong's Review of Medical Physiology, Robbins Pathologic Basis of Disease, and Medical Physiology. Let me compile the complete answer.
The Pleura
1. Overview
The pleura is the serous membrane that encloses each lung. It consists of a single layer of flat cells - the mesothelium - and an underlying layer of supporting connective tissue. Each pleural cavity is the potential space enclosed between the two layers of pleura, normally containing only 15-20 mL of serous fluid that lubricates the lung surfaces and reduces friction during breathing.
- Gray's Anatomy for Students, p. 201
- Color Atlas of Human Anatomy Vol. 2
2. Anatomy
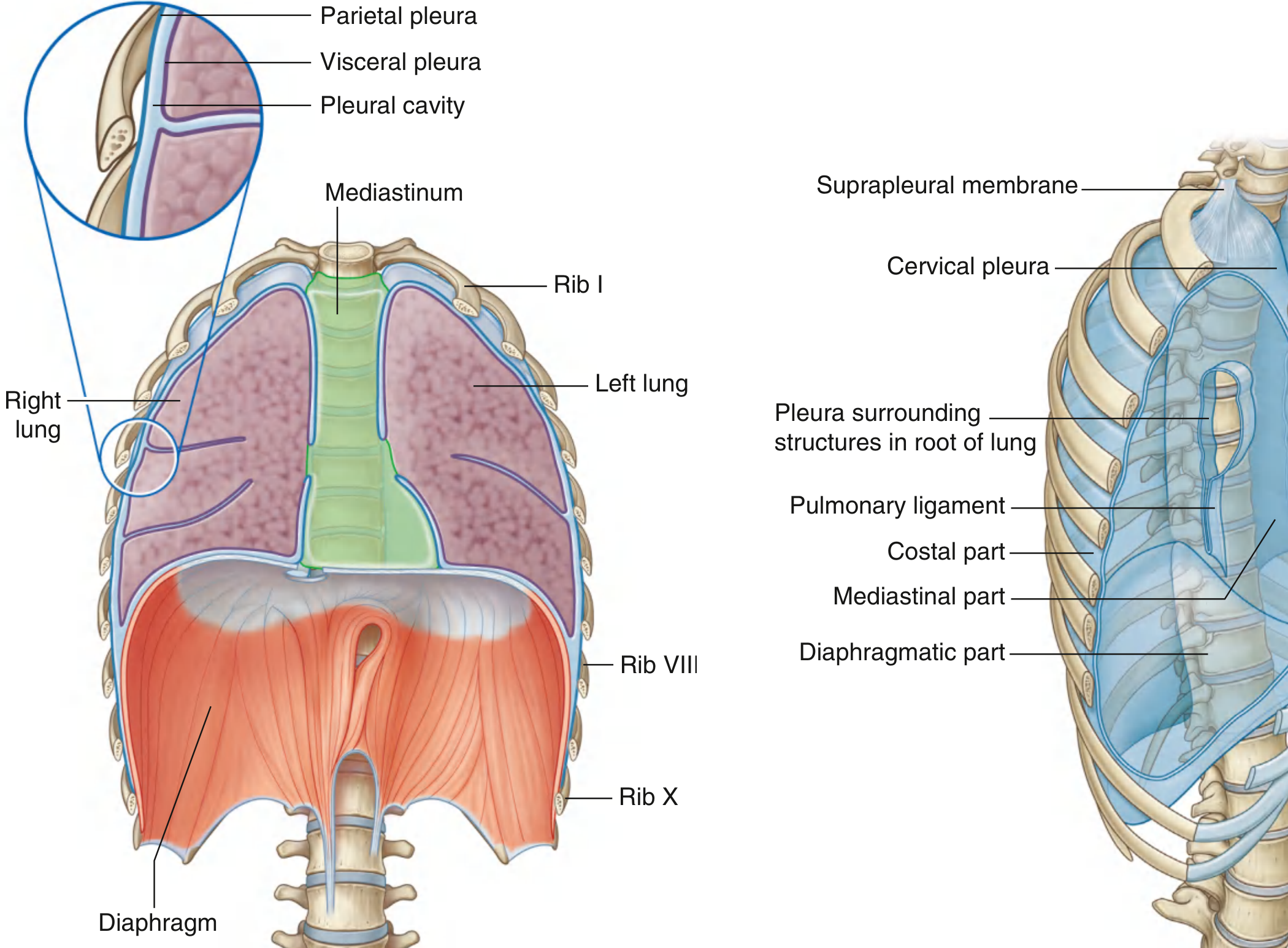
Fig. 3.38 & 3.39 - Pleural Cavities and Parietal Pleura. (Gray's Anatomy for Students)
Visceral Pleura
- Covers the lung surface almost entirely and cannot be stripped from it
- Dips into the interlobular fissures
- Continuous with the parietal pleura at the hilum of the lung
- Contains three connective tissue layers that support lung shape:
- Elastic fibers wrapping the lung lobes (following the mesothelium)
- Fine fibers outlining individual alveoli
- An intermediate layer of connective tissue interspersed with cells
- Its neurovascular supply and lymphatic drainage mirror those of the lung
- Ganong's Review of Medical Physiology; Color Atlas of Human Anatomy
Parietal Pleura
Named according to the wall region it covers:
| Part | Location |
|---|---|
| Costal part | Lines the ribs and intercostal spaces |
| Diaphragmatic part | Covers the diaphragm |
| Mediastinal part | Covers the mediastinum |
| Cervical pleura (pleural cupula) | Dome-shaped, extends above the superior thoracic aperture into the root of the neck |
The suprapleural membrane is a connective tissue sheet covering the superior surface of the cervical pleura. It attaches laterally to the medial margin of the first rib and posteriorly to the transverse process of CVII. Scalene muscle fibers attach to it superiorly to keep it taut, providing apical support for the pleural cavity.
- Gray's Anatomy for Students; Color Atlas of Human Anatomy
Pleural Recesses
Complementary spaces formed at junctions between pleural parts that expand during deep inspiration:
- Costodiaphragmatic recess - between the costal and diaphragmatic pleura; the most clinically significant recess (most dependent - fluid collects here first)
- Costomediastinal recess - between the costal and mediastinal pleura; wider on the left at the level of the cardiac notch
Root of the Lung
At vertebrae TV-TVII, the mediastinal pleura forms a sleeve-like covering around structures (airway, vessels, nerves, lymphatics) passing between the mediastinum and lung. This forms the root of the lung, which joins the medial lung surface at the hilum, where mediastinal pleura becomes continuous with visceral pleura.
3. Nerve Supply
| Pleura | Innervation | Pain referral |
|---|---|---|
| Costal parietal | Intercostal nerves (somatic afferents) | Thoracic wall |
| Diaphragmatic parietal (central) | Phrenic nerve (C3-C5) | Shoulder tip (referred) |
| Diaphragmatic parietal (peripheral) | Intercostal nerves | Thoracic/abdominal wall |
| Mediastinal parietal | Phrenic nerve | Shoulder tip (referred) |
| Visceral pleura | Autonomic (visceral) - insensitive to pain | - |
This difference in innervation explains why central diaphragmatic pleuritis causes shoulder pain, while costal pleuritis causes localised chest wall pain.
4. Blood Supply & Lymphatics
- Visceral pleura: branches of the pulmonary vasculature
- Parietal pleura: posterior intercostal arteries, internal thoracic artery, musculophrenic artery; venous drainage via thoracic wall veins
- Lymphatic drainage of the parietal pleura follows the thoracic wall; visceral pleura drains into bronchopulmonary nodes
5. Pleural Surface Borders
The pleural borders (unlike the lung borders) do not change during respiration. During quiet breathing, the inferior lung margins extend 1-2 intercostal spaces above the inferior pleural border:
| Surface line | Lung inferior border | Pleural inferior border |
|---|---|---|
| Midclavicular | Rib 6 | Rib 8 |
| Midaxillary | Rib 8 | Rib 10 |
| Paravertebral | Rib 10 | Rib 12 |
The costodiaphragmatic recess is never completely filled by the lung, providing a useful landmark for clinical procedures.
6. Physiology
The pleural fluid (~15-20 mL) forms a thin layer between the pleural membranes, preventing friction during the respiratory cycle. The cavity and its infoldings allow lung movement within the thoracic cage.
Critically, the intrapleural pressure is normally negative relative to atmospheric pressure, which keeps the lung expanded against the chest wall. Accumulation of air (pneumothorax) or fluid (pleural effusion) in the intrapleural space restricts alveolar expansion and impairs ventilation.
- Medical Physiology (Boron & Boulpaep); Ganong's Review of Medical Physiology
7. Pathology (Robbins Pathologic Basis of Disease)
Most pleural disorders arise as complications of disease elsewhere. Primary pleural disease is less common.
Pleural Effusion
Fluid accumulation (>15 mL) occurs via:
- Increased hydrostatic pressure - congestive heart failure (most common)
- Increased vascular permeability - pneumonia
- Decreased osmotic pressure - nephrotic syndrome, cirrhosis
- Increased intrapleural negative pressure - atelectasis
- Decreased lymphatic drainage - mediastinal carcinomatosis
Inflammatory effusions (Exudates)
- Serous/serofibrinous pleuritis - TB, pneumonia, lung infarction, abscess, bronchiectasis; also rheumatoid arthritis, SLE, uremia, radiotherapy
- Empyema - purulent exudate from bacterial/fungal seeding; characterized by loculated yellow-green pus (masses of neutrophils). If unresolved, organizes into dense fibrous adhesions restricting pulmonary expansion
- Hemorrhagic pleuritis - hemorrhagic diatheses, rickettsial infections, neoplasms
Noninflammatory effusions (Transudates)
- Hydrothorax - clear straw-coloured fluid; most commonly heart failure, also renal failure, cirrhosis
- Hemothorax - blood in the pleural cavity; usually traumatic; aortic aneurysm rupture is almost invariably fatal
- Chylothorax - milky fluid from lymphatic disruption (thoracic duct trauma or malignant obstruction)
Pneumothorax
Air in the pleural cavity. Types:
| Type | Cause |
|---|---|
| Spontaneous idiopathic | Rupture of apical subpleural blebs; young, tall individuals; tends to recur |
| Secondary spontaneous | Complication of emphysema, asthma, TB, abscess |
| Traumatic | Chest wall or lung penetration |
| Tension pneumothorax | Flap-valve effect - air enters on inspiration but cannot escape; progressively increasing intrapleural pressure compresses mediastinum and contralateral lung - medical emergency |

Fig. 15.39 - Tension pneumothorax (right-sided) showing mediastinal shift. (Robbins Pathologic Basis of Disease)
Pleural Tumors
Solitary Fibrous Tumor
- Soft tissue tumor, propensity for the pleura; highly associated with NAB2::STAT6 fusion gene (cryptic inversion of chromosome 12)
- Grossly: dense fibrous tissue, often pedunculated; microscopically: whorls of reticulin/collagen with fibroblast-like spindle cells
- Immunostaining: CD34+, STAT6+, keratin- (distinguishes from mesothelioma)
- No association with asbestos exposure
Malignant Mesothelioma
- Arises from visceral or parietal pleura
- Strongly associated with asbestos exposure (up to 90% in high-exposure regions); 25-45 year latent period
- Lifetime risk in heavily exposed individuals: 7-10%
- Smoking does NOT increase mesothelioma risk (contrast with lung carcinoma)
- Most common cytogenetic abnormality: homozygous deletion of the CDKN2A locus (encoding p16/INK4a and p14/ARF)
- Immunostaining: keratin+ (opposite to solitary fibrous tumor)
- Tends to encase the lung as a thick rind; spreads locally to mediastinum and diaphragm
Metastatic tumors are far more common than primary pleural tumors. Most frequent primaries: lung and breast. Ovarian carcinomas classically produce widespread pleural implants with serous/serosanguineous effusions - cytological examination of effusion sediment has significant diagnostic value.
Sources:
- Gray's Anatomy for Students (Gray's)
- Color Atlas of Human Anatomy Vol. 2
- Ganong's Review of Medical Physiology, 26th Edition
- Medical Physiology (Boron & Boulpaep)
- Robbins, Cotran & Kumar - Pathologic Basis of Disease
Difference between right and lwft lung
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed. Let me compile the comprehensive comparison.
Right Lung vs Left Lung - Key Differences
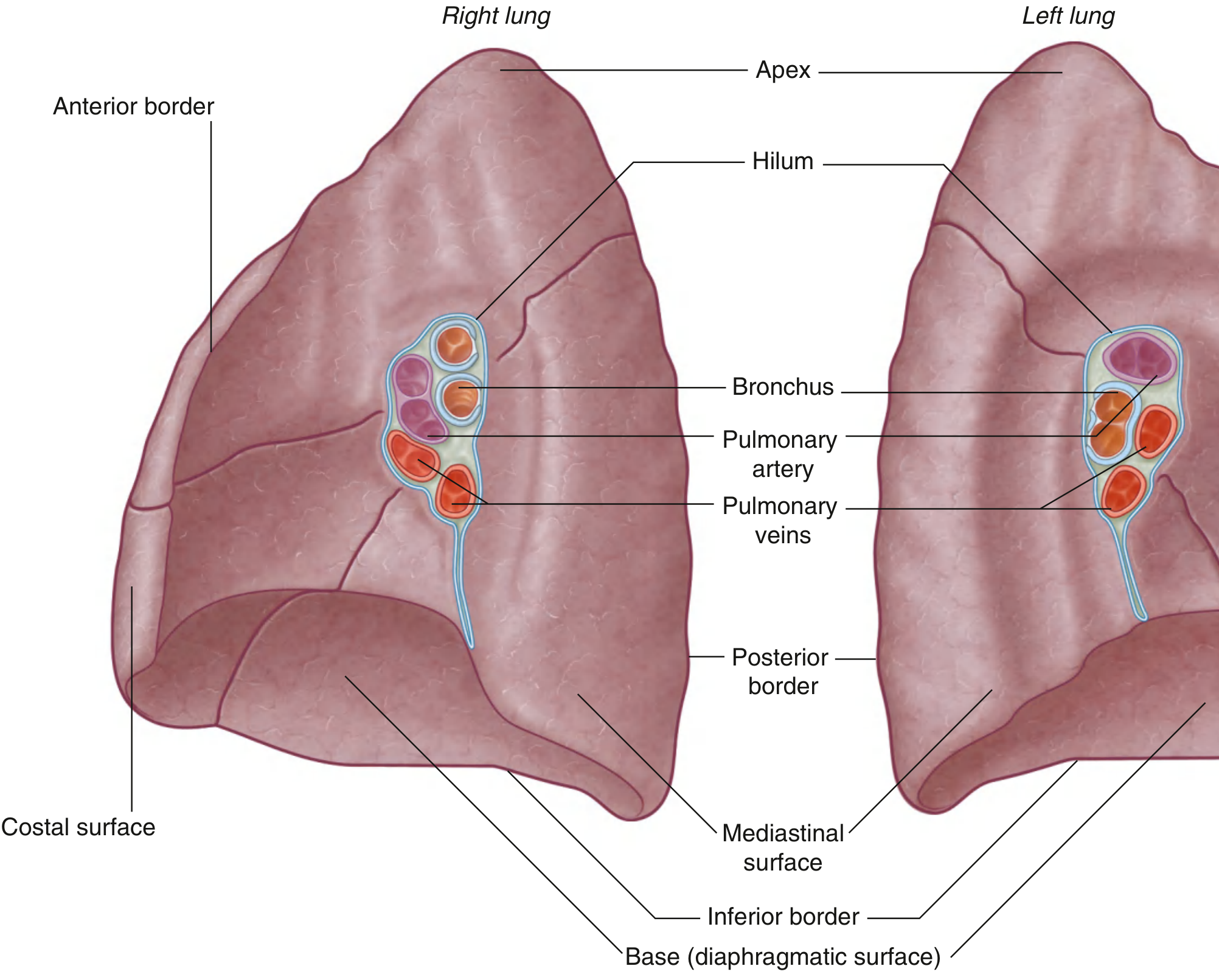
1. Size & Shape
| Feature | Right Lung | Left Lung |
|---|---|---|
| Relative size | Larger (slightly) | Smaller |
| Shape | Shorter and wider | Longer and narrower |
| Reason | Liver pushes diaphragm up on right | Heart bulges more to the left |
| Cardiac notch | Absent | Present - notch on inferior medial surface where heart projects in |
| Lingula | Absent | Present - tongue-like projection from anterior border of upper lobe, overlying the cardiac notch |
2. Lobes & Fissures
| Feature | Right Lung | Left Lung |
|---|---|---|
| Number of lobes | 3 (upper, middle, lower) | 2 (upper, lower) |
| Fissures | 2 - oblique + horizontal | 1 - oblique only |
| Oblique fissure | Starts at ~TIV, crosses 5th interspace, follows rib VI | Starts between TIII-TIV, same lateral course - slightly more oblique |
| Horizontal fissure | Follows 4th intercostal space anteriorly, meets oblique at rib V | Absent |
| Middle lobe equivalent | Middle lobe (distinct lobe) | Lingula (part of upper lobe, not a separate lobe) |
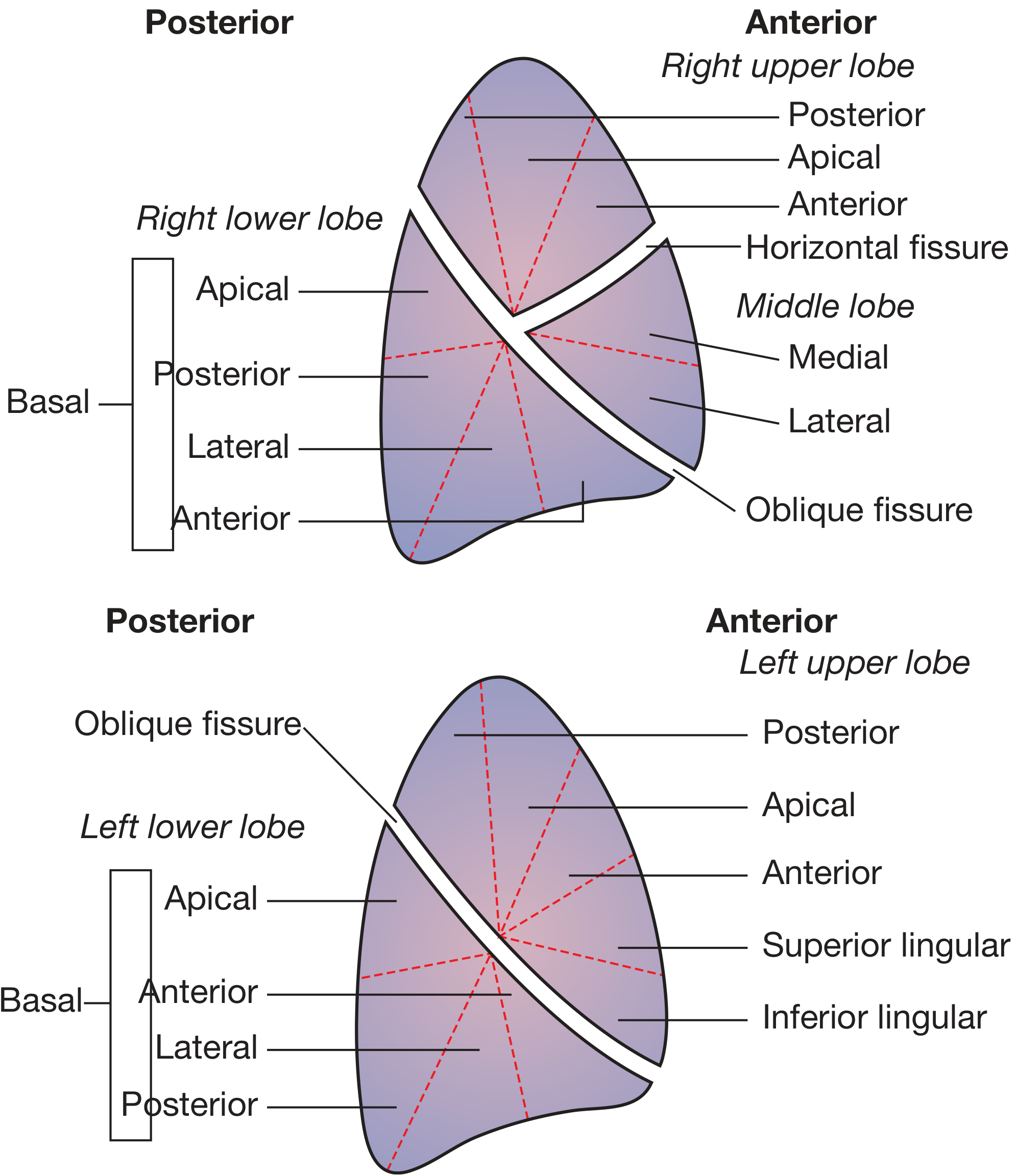
3. Bronchopulmonary Segments
| Right Lung (10 segments) | Left Lung (8-10 segments) |
|---|---|
| Upper lobe: apical, posterior, anterior (3) | Upper lobe: apical-posterior, anterior, superior lingular, inferior lingular (4) |
| Middle lobe: lateral, medial (2) | (No middle lobe) |
| Lower lobe: superior, medial basal, anterior basal, lateral basal, posterior basal (5) | Lower lobe: superior, anterior-medial basal, lateral basal, posterior basal (4) |
Note: In the left lung, the apical and posterior segments of the upper lobe are fused into a single apico-posterior segment, and the medial and anterior basal segments of the lower lobe are fused - giving 8 segments (some texts count 10 by splitting these).
4. Main Bronchus
| Feature | Right Main Bronchus | Left Main Bronchus |
|---|---|---|
| Length | Shorter (~2.5 cm) | Longer (~5 cm) |
| Width | Wider | Narrower |
| Angle | More vertical (in line with trachea) | More horizontal |
| Superior lobe bronchus | Branches within the root (before entering lung) | Branches within the lung |
| Clinical consequence | Inhaled foreign bodies preferentially lodge here | Less commonly affected |
The right main bronchus is more vertical because it is more directly in line with the trachea - this is also why aspirated vomit, blood, and foreign bodies tend to enter the right lung more often.
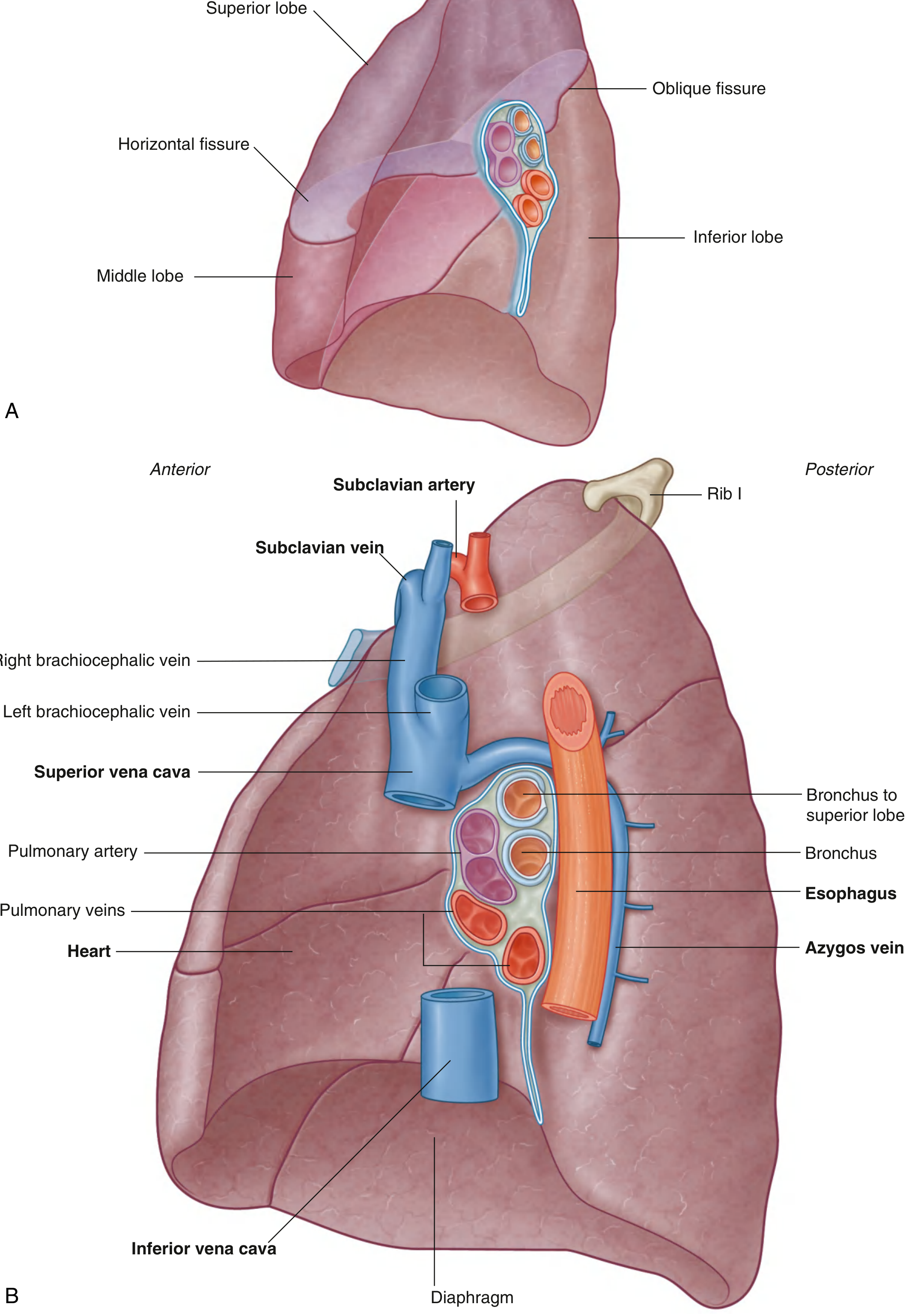
5. Mediastinal Relations (Impressions on Medial Surface)
| Right Lung | Left Lung |
|---|---|
| Heart (right side) | Heart (most of cardiac impression) |
| Inferior vena cava | Aortic arch |
| Superior vena cava | Thoracic (descending) aorta |
| Azygos vein | Esophagus |
| Esophagus | Left subclavian artery |
| Right subclavian artery/vein | Left subclavian vein |
The left lung has grooves for the aortic arch and descending aorta along its medial/posterior surface - features entirely absent from the right lung.
Summary Table
| Feature | Right Lung | Left Lung |
|---|---|---|
| Lobes | 3 | 2 |
| Fissures | 2 (oblique + horizontal) | 1 (oblique) |
| Bronchopulmonary segments | 10 | 8-10 |
| Main bronchus | Shorter, wider, more vertical | Longer, narrower, more horizontal |
| Foreign body aspiration | More common | Less common |
| Cardiac notch | Absent | Present |
| Lingula | Absent | Present |
| Size | Larger, shorter, wider | Smaller, longer, narrower |
| Reason for size difference | Liver below (raises diaphragm) | Heart displaces to left |
| Key mediastinal relations | SVC, IVC, azygos, esophagus | Aortic arch, thoracic aorta, esophagus |
Sources: Gray's Anatomy for Students; Bailey and Love's Short Practice of Surgery, 28th Ed.
Bronchial tree
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I have comprehensive content from multiple authoritative textbooks. Let me now compile the full answer.
The Bronchial Tree
Overview: Conducting vs. Respiratory Portions
The respiratory system is divided into two functional parts:
-
Conducting portion: nasal cavities → pharynx → larynx → trachea → bronchi → bronchioles → terminal bronchioles. Conditions and conducts air; no gas exchange.
-
Respiratory portion: respiratory bronchioles → alveolar ducts → alveolar sacs → alveoli. Gas exchange occurs here.
-
Junqueira's Basic Histology, 17th Ed.
1. Trachea
- Extends from vertebral level CVI (lower neck) to TIV/V (mediastinum), where it bifurcates
- Held open by C-shaped hyaline cartilage rings (16-20); open part faces posteriorly, closed by the trachealis smooth muscle
- Lined by pseudostratified ciliated columnar (respiratory) epithelium with goblet cells, on a thick basement membrane
- The lowest tracheal ring has the carina - a hook-shaped ridge projecting between the origins of the two main bronchi; highly sensitive area (cough reflex)
2. Primary (Main) Bronchi
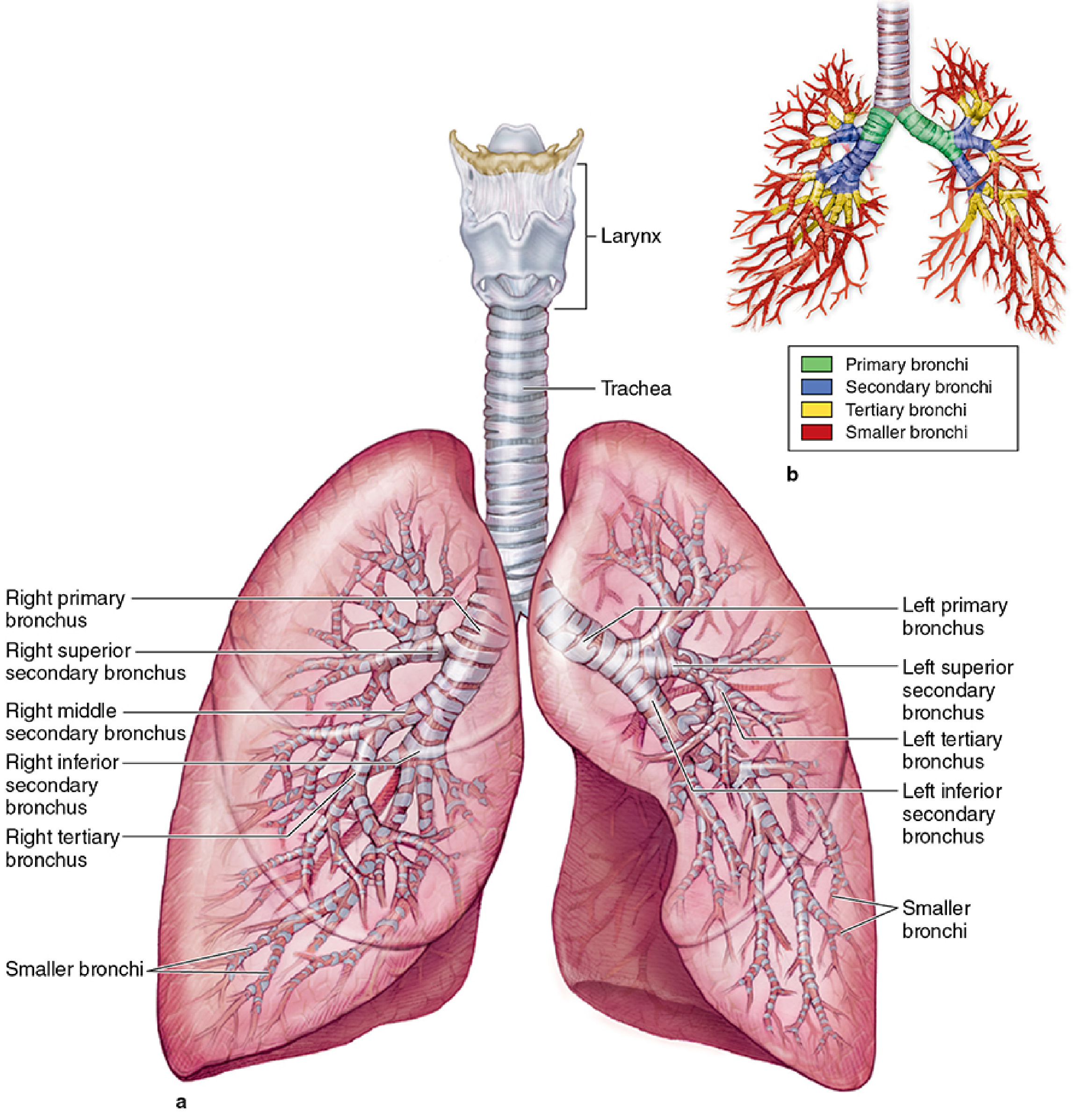
The trachea bifurcates into right and left primary (main) bronchi:
| Feature | Right Main Bronchus | Left Main Bronchus |
|---|---|---|
| Length | ~2.5 cm (shorter) | ~5 cm (longer) |
| Width | Wider | Narrower |
| Angle | More vertical (~25° from midline) | More horizontal (~45° from midline) |
| Clinical note | Foreign bodies preferentially lodge here | Less commonly affected |
Each main bronchus enters the lung at the hilum. On the right side, the superior lobar bronchus branches off within the root (before fully entering the lung); on the left, it branches within the lung.
Histology of bronchi:
- Respiratory (pseudostratified ciliated columnar) epithelium
- Prominent spiral bands of smooth muscle
- Irregular plates of hyaline cartilage (not rings - become discontinuous as bronchi narrow)
- Submucosal mucous and serous glands
- Elastic fibers
3. Lobar (Secondary) Bronchi
- Right lung: 3 lobar bronchi (superior, middle, inferior)
- Left lung: 2 lobar bronchi (superior, inferior)
- Diameter: 8-12 mm
- Each supplies one lobe
- Right superior lobar bronchus arises ~1-2.5 cm from the tracheal bifurcation; the right middle and inferior, and all left lobar bronchi arise ~5 cm from the bifurcation
4. Segmental (Tertiary) Bronchi
- Each lobar bronchus divides into segmental bronchi
- Right lung: 10 segmental bronchi; Left lung: 9 segmental bronchi (some fused)
- Each segmental bronchus, with its accompanying branch of the pulmonary artery, defines a bronchopulmonary segment
Bronchopulmonary Segments
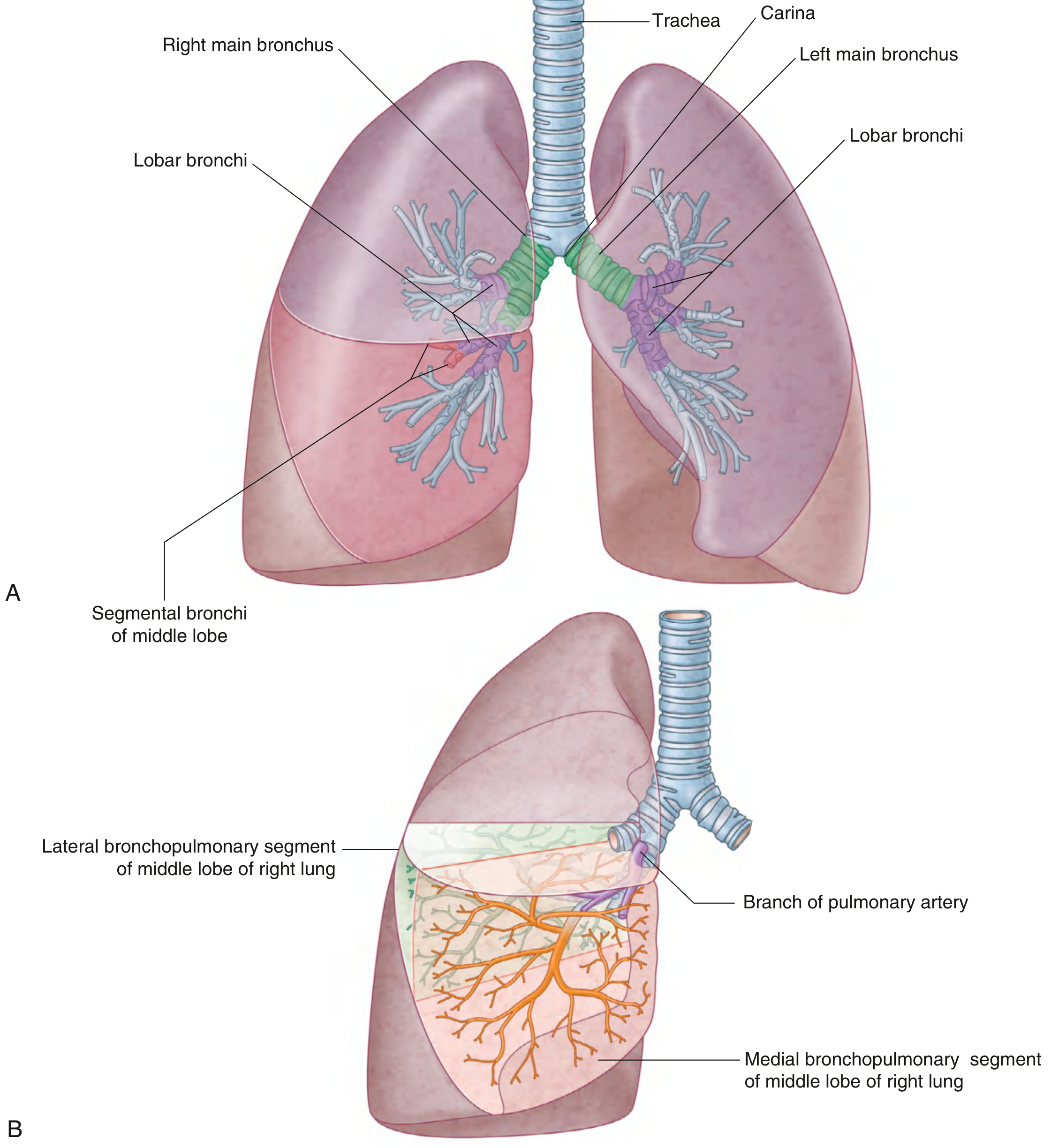
A bronchopulmonary segment is:
- An irregular cone with its apex toward the hilum and base on the lung surface
- The smallest functionally independent region of lung
- The smallest area that can be surgically resected without affecting adjacent lung
- Contains a central segmental bronchus + pulmonary artery branch (bronchoarterial unit)
- Pulmonary vein tributaries travel intersegmentally (between segments), demarcating boundaries
Right lung segments (10):
- Upper lobe: apical (1), posterior (2), anterior (3)
- Middle lobe: lateral (4), medial (5)
- Lower lobe: superior (6), medial basal (7), anterior basal (8), lateral basal (9), posterior basal (10)
Left lung segments (8-9):
- Upper lobe: apico-posterior (1+2 fused), anterior (3), superior lingular (4), inferior lingular (5)
- Lower lobe: superior (6), anteromedial basal (7+8 fused), lateral basal (9), posterior basal (10)
5. Smaller Bronchi → Bronchioles
The segmental bronchi divide through multiple generations into medium and small bronchi, then into bronchioles (diameter ≤1 mm). Each bronchiole enters a pulmonary lobule.
Bronchioles
- No cartilage (key distinction from bronchi)
- No submucosal glands
- Epithelium: simple ciliated columnar to cuboidal with club cells (formerly Clara cells)
- Prominent circular layer of smooth muscle (proportionately thicker than bronchi)
- Elastic fibers in lamina propria
Each bronchiole divides into 5-7 terminal bronchioles within each lobule.
Terminal Bronchioles
- Last part of the conducting portion (no alveoli, no gas exchange)
- Epithelium: simple cuboidal, ciliated cells + club cells predominate
- Club cells secrete: surfactant components, protease inhibitors, cytokines for local immune regulation; also serve as stem cells for bronchiolar epithelium
- Thin, incomplete smooth muscle layer; no cartilage
Clinical note - Asthma: Chronic inflammation causes mast cell degranulation → sudden smooth muscle constriction (bronchospasm) in bronchioles. Epinephrine/sympathomimetics relax the muscle and relieve obstruction. - Junqueira's Basic Histology
6. Respiratory Bronchioles
Each terminal bronchiole subdivides into 2-3 respiratory bronchioles - the first part of the respiratory portion.
- Similar to terminal bronchioles but interrupted by scattered alveolar outpouchings (gas exchange begins here)
- Epithelium: simple cuboidal (club cells) with simple squamous cells at alveolar openings
- Smooth muscle and elastic connective tissue in lamina propria
- Alveoli become progressively more numerous moving distally
7. Alveolar Ducts → Alveolar Sacs → Alveoli
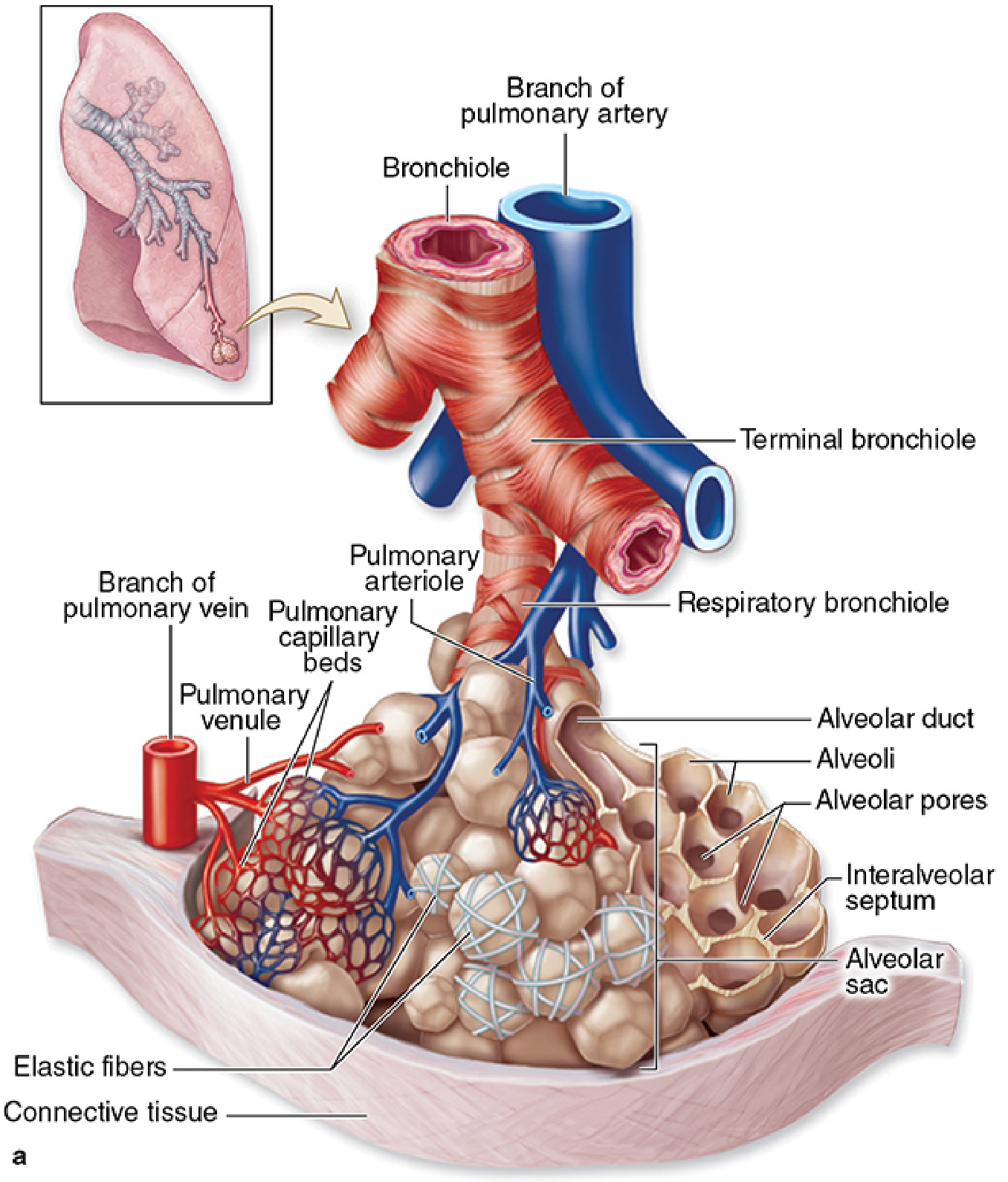
- Alveolar duct: a respiratory bronchiole leads to an alveolar duct, which is lined by a continuous series of alveoli in its walls
- Alveolar sac: cluster of alveoli at the blind end of an alveolar duct
- Alveoli: small, air-filled, saclike structures; sites of actual O₂/CO₂ exchange; separated by interalveolar septa containing elastic/reticular fibers and dense capillary networks
- Alveolar pores of Kohn: allow air pressure to equilibrate between adjacent alveoli; provide collateral ventilation if a local airway is blocked
Alveolar Cell Types
| Cell | Type | Features | Function |
|---|---|---|---|
| Type I pneumocytes | Extremely thin, squamous | Cover ~95% of alveolar surface | Gas exchange (diffusion) |
| Type II pneumocytes | Cuboidal, bulge into lumen; contain lamellar bodies | ~5% of surface but more numerous cells | Surfactant synthesis & secretion; stem cells (regenerate Type I) |
| Alveolar macrophages (dust cells) | Large, phagocytic | Free within alveoli or in septa | Clear particulate matter, pathogens |
Blood-Air Barrier
The diffusion path for gas exchange consists of only 3 layers:
- Type I alveolar cell (extremely thin cytoplasm)
- Fused basal laminae of alveolar epithelium and capillary endothelium
- Capillary endothelial cell (thin)
Total thickness: ~0.5 µm - optimized for rapid gas diffusion.
Summary: Divisions of the Bronchial Tree
| Division | Cartilage | Smooth Muscle | Epithelium | Gas Exchange |
|---|---|---|---|---|
| Trachea | C-rings (hyaline) | Trachealis (posterior) | Pseudostratified ciliated columnar | No |
| Primary bronchi | Rings → plates | Spiral bands | Pseudostratified ciliated columnar | No |
| Lobar bronchi (2°) | Irregular plates | Spiral bands | Pseudostratified ciliated columnar | No |
| Segmental bronchi (3°) | Irregular plates (smaller) | Spiral bands | Pseudostratified ciliated columnar | No |
| Bronchioles | None | Circular (prominent) | Simple ciliated columnar + club cells | No |
| Terminal bronchioles | None | Thin, incomplete | Simple cuboidal (club cells dominant) | No |
| Respiratory bronchioles | None | Elastic + smooth muscle | Simple cuboidal + scattered squamous | Begins here |
| Alveolar ducts | None | Elastic fibers | Lined by alveoli | Yes |
| Alveolar sacs / Alveoli | None | None | Type I + Type II pneumocytes | Yes |
Sources: Gray's Anatomy for Students; Junqueira's Basic Histology, 17th Ed.; Color Atlas of Human Anatomy Vol. 2; Bailey and Love's Short Practice of Surgery, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.