CLINICAL PRESENTATIONS of ncc in cns, muscle, eye and subcutaneous tissue
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
neurocysticercosis MRI brain cyst scolex
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full clinical presentation answer.
Clinical Presentations of Neurocysticercosis (NCC)
NCC is caused by CNS penetration of the larval stage (cysticercus) of the pork tapeworm Taenia solium, acquired by ingesting its eggs. Cysticerci can lodge in CNS parenchyma, ventricles, subarachnoid/cisternal spaces, spinal cord, eye, skeletal muscle, and subcutaneous tissue. Clinical manifestations depend entirely on location and the host inflammatory response to viable vs. degenerating vs. calcified cysts.
Gross Pathology — Brain Cysticercosis
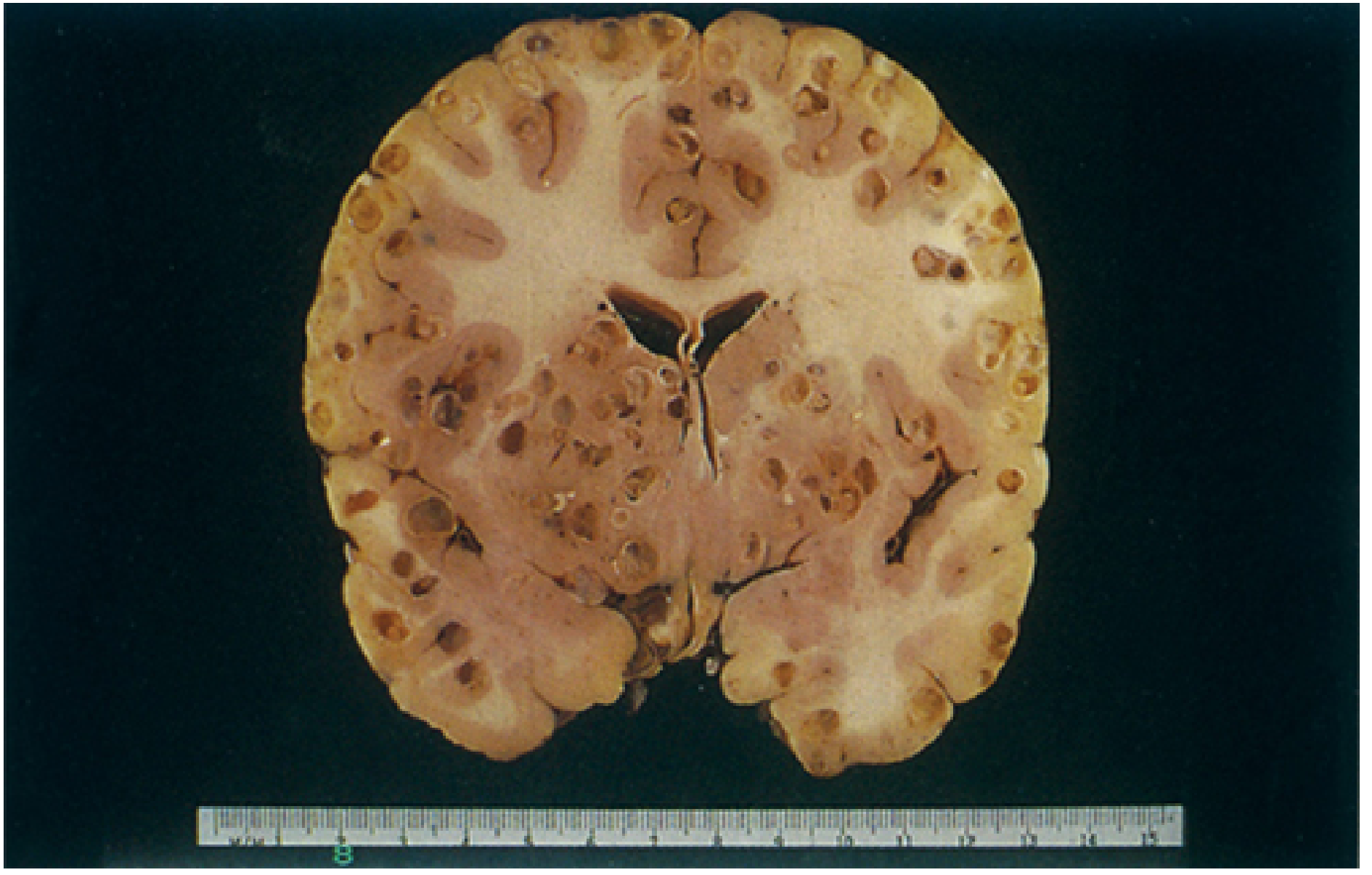
I. CNS Involvement
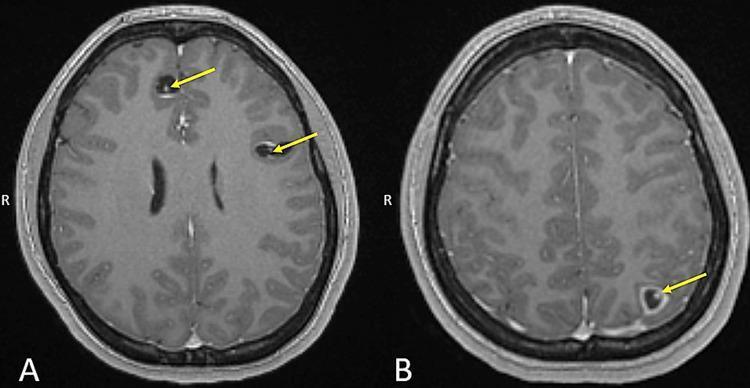
A. Parenchymal Neurocysticercosis
This is the most common form. Cysticerci lodge preferentially at the gray-white matter junction.
1. Single Enhancing Lesion (SEL)
- Most common manifestation in India and the United States
- Patient presents with headache or seizures (focal or focal with secondary generalization)
- Many have a single seizure or a few seizures during the period when the cysticercus is degenerating; seizures are eventually self-limited in most
- Some cases progress to calcified lesions, which are a risk factor for recurrent seizures
2. Multiple Parenchymal Cysticerci
- Main presentation is seizures associated with parenchymal inflammation
- Seizures are more likely to recur than with single lesions
3. Calcified Lesions
- Patients may develop recurrent seizures over years
- Some develop mesiotemporal sclerosis leading to refractory epilepsy
- Calcified lesions can intermittently become inflamed (edema/contrast enhancement on MRI) and trigger additional seizure episodes
4. Cysticercal Encephalitis
- Occurs with massive larval invasion, producing diffuse cerebral edema
- Presents as encephalopathy, raised ICP, seizures
- More common in children and young women
- Antiparasitic drugs are contraindicated in this form; treat with steroids only
Acute invasive stage features (Sherris): fever, headache, eosinophilia; heavy infection can cause meningoencephalitic syndrome with CSF eosinophilic pleocytosis.
B. Ventricular Cysticercosis
- Cysticerci most commonly lodge in the 4th ventricle, followed by 3rd and lateral ventricles
- Causes obstructive hydrocephalus — a medical emergency
- Symptoms: headache, nausea, vomiting, dizziness, altered mental status, papilledema with altered visual acuity
- A cysticercus in the 4th ventricle acting as a ball valve causes Bruns syndrome: intermittent acute hydrocephalus triggered by changes in head position — sudden severe headache, vomiting, loss of consciousness, and sometimes sudden death
C. Subarachnoid/Cisternal (Racemose) Cysticercosis
- Cysticerci in the basilar cisterns are often multilobulated ("racemose" = cluster-of-grapes form), can grow to several centimeters
- Typically accompanied by cysticerci at other locations (parenchymal, ventricular, spinal, or ocular)
- The cysts induce chronic arachnoiditis, with:
- Communicating hydrocephalus (headache, nausea, vomiting, dizziness, altered mental status)
- Chronic meningitis / meningeal signs
- Vascular involvement: large- or small-vessel strokes (arteritis)
- Mass effect
- Hemorrhage
- This is the most severe form of NCC with the highest fatality rate
D. Spinal Cysticercosis
- Less common
- Produces cord compression or meningeal inflammation (radiculitis)
- Symptoms: back/radicular pain, limb weakness, sensory deficits, myelopathy
- May present as chronic progressive paraparesis
Neuroimaging Overview
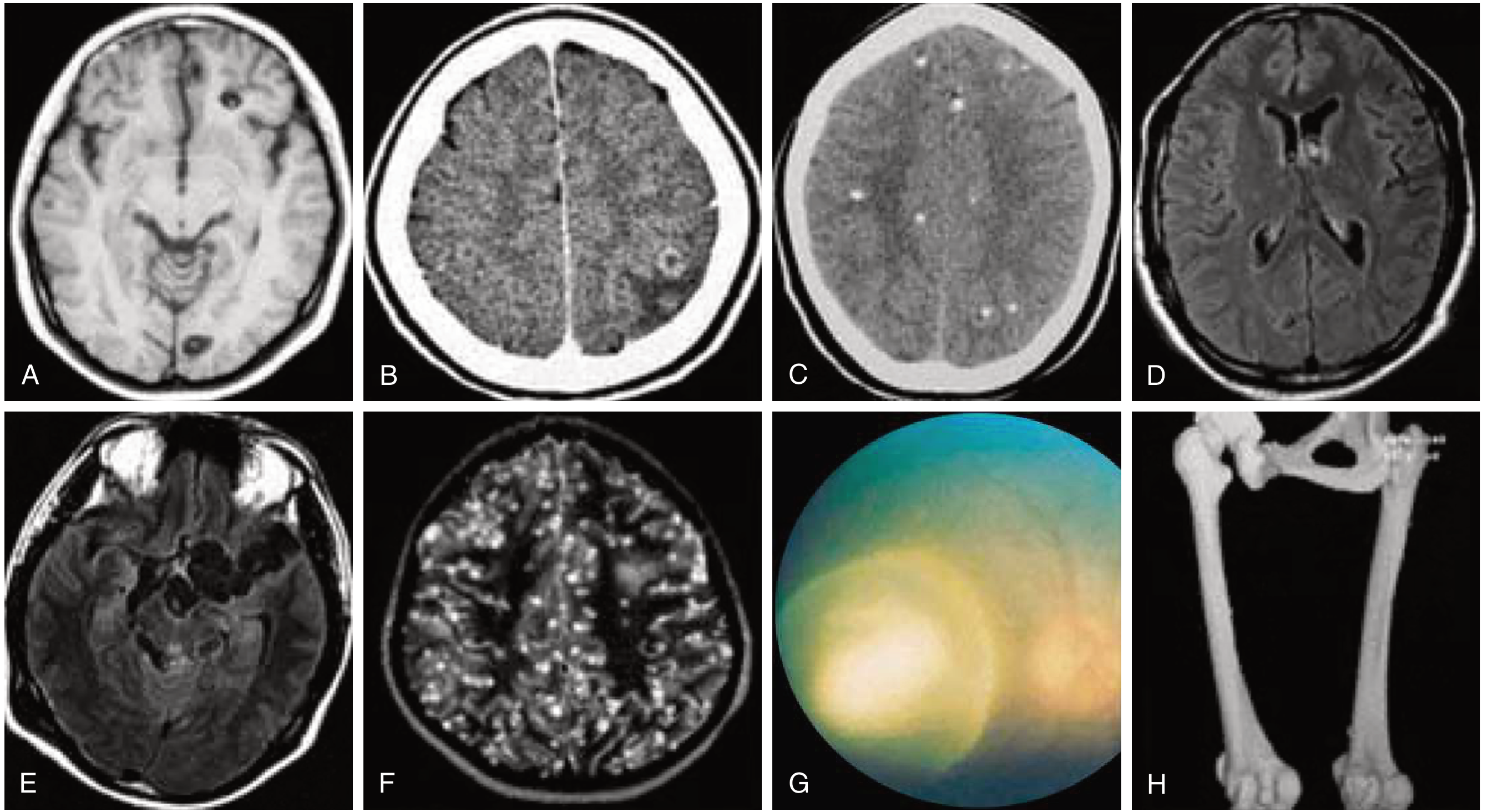
II. Ocular Cysticercosis
- Occurs in ~1–3% of all NCC cases; the eye may be the only site of involvement
- Cysts may lodge in:
- Vitreous humor (most common intraocular location)
- Subretinal space
- Anterior chamber
- Extraocular muscles (less common)
- Symptoms:
- Ocular pain and visual disturbances (floaters, blurring, decreased acuity)
- If subretinal: retinal detachment risk
- The degenerating cyst provokes severe inflammatory reaction with endophthalmitis → blindness
- Absolute diagnostic criterion: direct visualization of subretinal parasites by fundoscopic examination (shows the scolex)
- Note: Antiparasitic drugs are contraindicated in ocular cysticercosis — destruction of the cyst in the eye causes severe intraocular inflammation; surgical removal is the treatment of choice
III. Muscular Cysticercosis
- Generally asymptomatic as long as cysts remain viable (the live cyst suppresses host inflammatory response)
- Death of larvae → marked inflammatory reaction: fever, muscle pain, swelling, tenderness, and eosinophilia
- Heavy infection: pseudohypertrophy of muscles (especially tongue — classical)
- Cysts calcify over time → appear as characteristic cigar-shaped (rice-grain) calcifications on plain X-ray, most prominent in the limbs and trunk
- These calcifications are a minor criterion in NCC diagnostic scoring (evidence of cysticercosis outside the CNS)
- Headache can accompany all forms of disease
IV. Subcutaneous Cysticercosis
- Presents as firm, mobile, non-tender subcutaneous papulonodules, usually multiple
- More often palpable than visible
- Typically asymptomatic
- When the cyst dies: local inflammation, tenderness, eventually calcification
- Prevalence varies by region: recognized in <1%–20% of patients; more common in Asia and Africa than Latin America
- In some series (Brazil): 90% of patients had cysts in subcutaneous tissue, skeletal muscle, or mucous membranes, while CNS was affected in <10%
- On plain radiograph: calcified cysts visible in soft tissues
- Clinical importance: the presence of subcutaneous cysticercosis should always prompt evaluation for NCC — surgical biopsy of a subcutaneous nodule can confirm the diagnosis (demonstrating the larva), and the finding counts as a major clinical/exposure criterion for NCC diagnosis
Summary Table
| Location | Key Clinical Features |
|---|---|
| Parenchymal brain | Seizures (most common NCC presentation globally); headache; focal neurological deficits; personality/cognitive changes |
| Calcified lesions | Recurrent seizures; risk of mesiotemporal sclerosis → refractory epilepsy |
| Ventricular | Obstructive hydrocephalus; Bruns syndrome (positional acute hydrocephalus); medical emergency |
| Subarachnoid/cisternal | Chronic arachnoiditis; communicating hydrocephalus; strokes; meningeal signs; highest fatality |
| Spinal | Radiculitis; myelopathy; paraparesis |
| Eye | Pain; visual disturbance; floaters; retinal detachment; endophthalmitis/blindness if cyst ruptures |
| Muscle | Usually asymptomatic; with larval death: fever, muscle pain, eosinophilia; pseudohypertrophy; rice-grain calcifications |
| Subcutaneous | Firm, mobile, asymptomatic nodules; calcify with time; important as diagnostic clue to systemic cysticercosis |
Headache is common to all CNS forms. Seizures predominate with parenchymal inflammation; hydrocephalus predominates with ventricular/subarachnoid disease.
Sources: Goldman-Cecil Medicine, 26e · Harrison's Principles of Internal Medicine, 22e · Bradley & Daroff's Neurology in Clinical Practice · Sherris & Ryan's Medical Microbiology, 8e · Dermatology 5e (Elsevier)
This is a shared conversation. Sign in to Orris to start your own chat.