Mechanisms of clasp knife spasticity through 1a and 2 afferent fibre
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
clasp knife spasticity mechanism afferent
I now have all the material needed for a comprehensive answer. Here is the full synthesis:
Clasp-Knife Spasticity: Mechanisms Through Ia and Group II Afferent Fibres
Overview
Clasp-knife spasticity is the velocity-dependent increase in muscle tone followed by a sudden release of resistance during passive stretch of a spastic limb — named for its resemblance to closing a pocket knife. Two distinct reflex mechanisms, mediated by Group Ia and Group II (type II) afferent fibres, underlie its characteristic biphasic quality.
1. The Muscle Spindle and Its Afferents
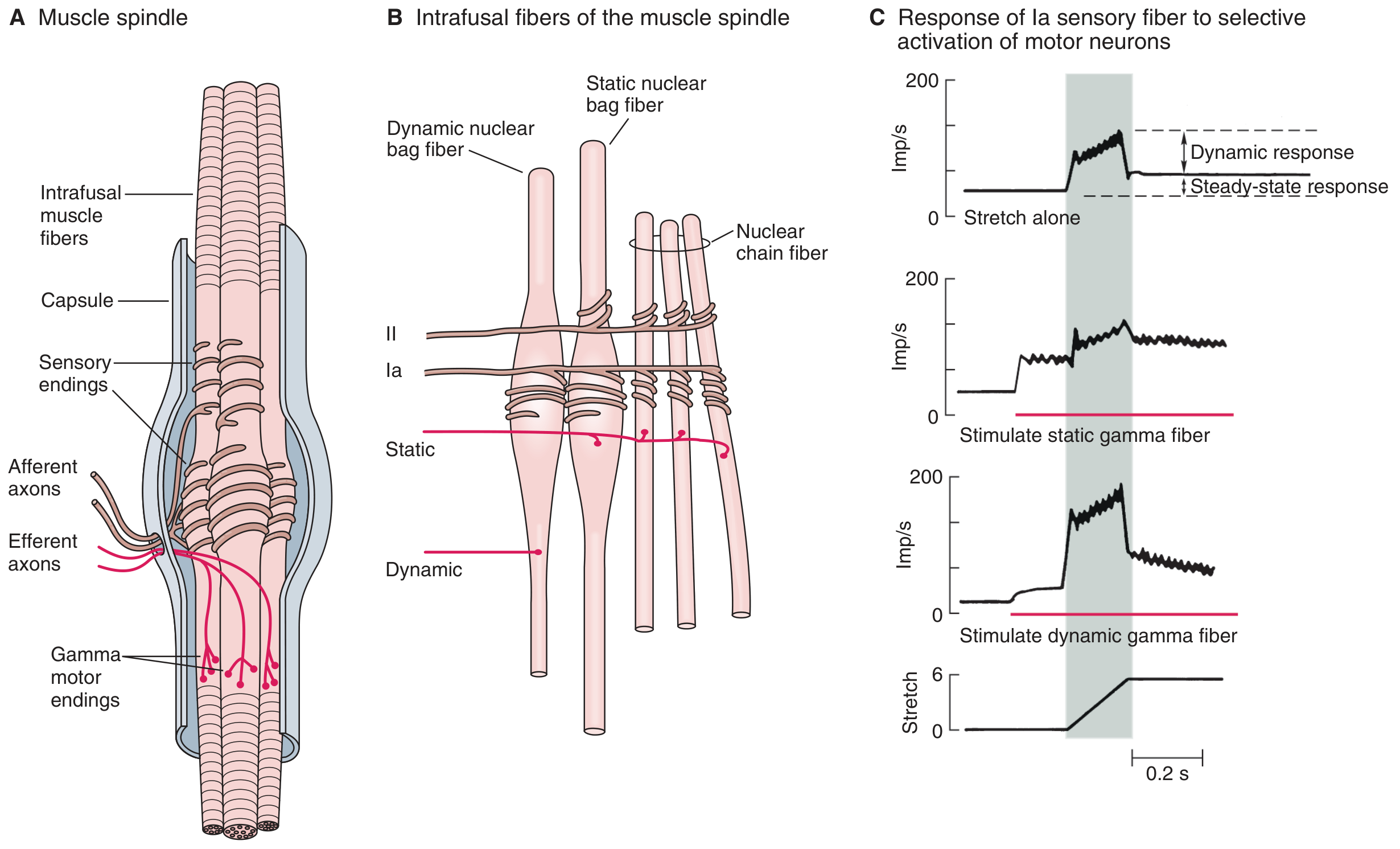
Ganong's Review of Medical Physiology — Mammalian muscle spindle. Panel B shows the single Group Ia (primary) ending innervating all three intrafusal fibre types, and Group II (secondary) endings on nuclear chain and static bag fibres.
| Feature | Group Ia (Primary) | Group II (Secondary) |
|---|---|---|
| Fibre diameter | ~17 µm (large myelinated) | ~8 µm |
| Conduction velocity | 70–120 m/s | Slower |
| Location | Nuclear bag + chain fibres | Nuclear chain + static bag |
| Detects | Velocity of length change (dynamic) + static length | Static length only |
| Response | Strong dynamic burst + steady tonic firing | Tonic/static firing proportional to length |
| Spinal target | Monosynaptic → α-motor neurons | Polysynaptic → interneurons → α-motor neurons |
- Group Ia (annulospiral/primary ending): wraps around the equatorial region of both dynamic nuclear bag fibres and nuclear chain fibres. It fires powerfully during the rate of change of stretch (dynamic response) and maintains tonic discharge proportional to length (static response).
- Group II (flower-spray/secondary ending): located adjacent to the Ia ending on nuclear chain and static nuclear bag fibres. It does not innervate dynamic bag fibres, and it has no dynamic response — it signals only sustained muscle length.
— Guyton and Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology, 26th ed.; Costanzo Physiology, 7th ed.
2. The Spastic State: Prerequisite for Clasp-Knife
In an upper motor neuron (UMN) lesion, descending inhibitory control is disrupted:
- The dorsal reticulospinal tract (normally inhibitory to stretch reflexes) is damaged, disinhibiting spinal interneurons.
- The medial reticulospinal and vestibulospinal tracts remain relatively intact, facilitating extensor tone.
- The result is excess tonic γ-motor neuron drive, particularly via elevated spinal serotonin, norepinephrine, and glutamate, with reduced glycinergic/GABAergic inhibition.
- α-motor neuron excitability is increased, and Group II afferent activity is amplified — Bradley and Daroff explicitly states that spasticity "reflects altered firing of alpha motoneurons and interneurons, together with increased activity of Group II nerve fibres derived from muscle spindles."
— Adams and Victor's Principles of Neurology, 12th ed.; Bradley and Daroff's Neurology in Clinical Practice
3. Phase 1 — The Initial "Catch": Group Ia-Mediated Resistance
When a spastic limb is moved briskly:
- Stretch is imposed rapidly → intrafusal fibres are stretched.
- Group Ia afferents fire intensely — they detect the velocity of stretch. In spasticity, tonic γ-dynamic overactivity keeps the dynamic nuclear bag fibres under tension, pre-sensitising Ia endings so they are already near-threshold.
- Ia afferents enter the spinal cord and monosynaptically excite α-motor neurons of the homonymous muscle, generating a strong, velocity-dependent contraction — the felt "catch."
- Simultaneously, Ia afferents inhibit antagonist motor neurons via Ia interneurons (reciprocal inhibition).
This is the mechanism of velocity-dependent hyperreflexia: fast stretch → massive Ia discharge → reflex contraction. Slow stretch produces little or no tone change, which is the hallmark distinguishing spasticity from rigidity.
"When the muscles are stretched briskly, the limb moves freely for a very short distance, after which there is an abrupt catch with rapidly increasing muscular resistance." — Adams and Victor's Principles of Neurology, 12th ed.
4. Phase 2 — The "Knife Snap": Group II and Golgi Tendon Organ-Mediated Release
As stretch continues and tension in the muscle builds:
4a. Group II (secondary afferent) contribution
- Group II afferents encode sustained muscle length. As passive stretch is maintained and muscle length increases, Group II discharge rises progressively.
- Unlike Ia fibres, Group II afferents are not strongly velocity-sensitive but are tonically active at increased lengths.
- In spasticity, Group II afferents gain increased excitatory influence (disinhibition via loss of descending GABAergic interneuron control). This sustained, polysynaptic excitatory drive contributes to the maintenance of the "catch" and sustains α-motor neuron firing even after the rapid Ia burst subsides.
- As stretch continues beyond a critical point, Group II excitatory input along with Ib-mediated inhibition from Golgi tendon organs overwhelms the excitatory Ia drive, contributing to collapse of resistance.
4b. Golgi Tendon Organ / Group Ib — the inverse stretch reflex
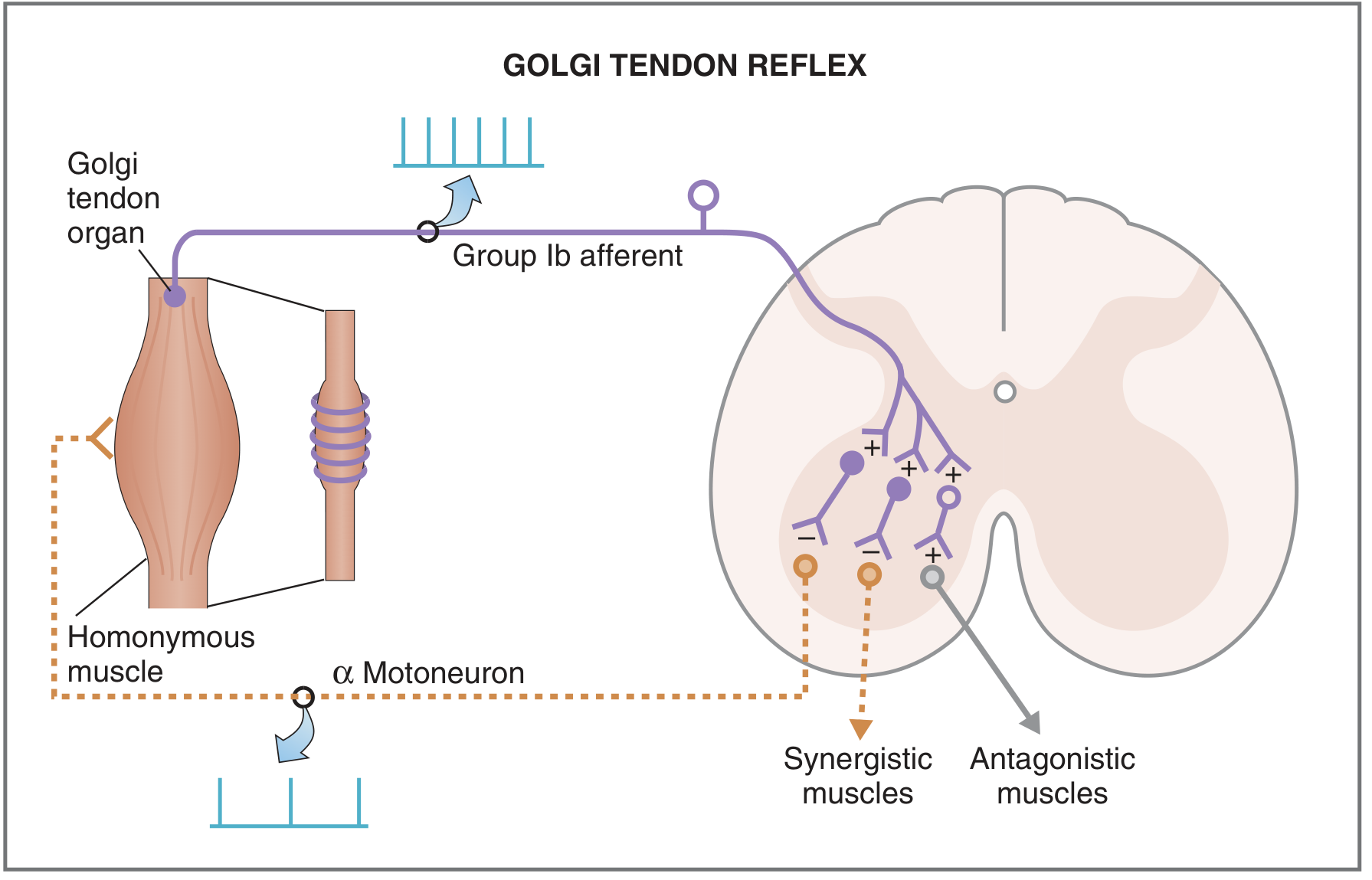
Costanzo Physiology — Golgi tendon reflex pathway. Group Ib afferents synapse on inhibitory interneurons, which suppress α-motor neurons of the homonymous muscle.
- Golgi tendon organs (GTOs) are arranged in series with muscle fibres and respond to muscle tension (not length), transmitting via Group Ib afferents.
- When tension exceeds a threshold, Ib afferents activate inhibitory interneurons (Ib inhibitory interneurons / autogenic inhibition) → inhibit the homonymous α-motor neurons → sudden relaxation.
- In spasticity, this autogenic inhibitory threshold is effectively exceeded at high tensions, and the muscle "gives way" — the pocket-knife snapping shut.
"An exaggerated form of the Golgi tendon reflex is illustrated by the clasp-knife reflex... if the flexion continues, tension increases in the opposing muscle and activates the Golgi tendon reflex, which then causes the opposing muscles to relax and the joint to close rapidly." — Costanzo Physiology, 7th ed.
"The sequence of resistance followed by a sudden decrease in resistance when a limb is moved passively is known as the clasp-knife effect... Passive flexion of the elbow meets immediate resistance as a result of the stretch reflex in the triceps muscle. Further stretch activates the inverse stretch reflex. The resistance to flexion suddenly collapses..." — Ganong's Review of Medical Physiology, 26th ed.
5. Integrated Mechanism Summary
PASSIVE RAPID STRETCH of spastic muscle
↓
[PHASE 1 — CATCH]
Ia afferents fire (velocity-sensitive)
→ Monosynaptic excitation of α-MNs
→ Reflex contraction / resistance
↑ enhanced by: γ-motor overactivity, ↓ presynaptic Ia inhibition
↓
Stretch continues → tension builds
↓
[PHASE 2 — RELEASE]
Group II afferents (length-sensitive) sustain excitation
+ Group Ib afferents (GTO, tension-sensitive) activate
→ Ib inhibitory interneurons suppress α-MNs
→ Autogenic inhibition (inverse stretch reflex)
→ Sudden collapse of resistance
6. Why Ia Inhibition Fails in Spasticity
Several mechanisms amplify the Ia-driven phase in UMN lesions:
| Mechanism | Normal | Spastic |
|---|---|---|
| Presynaptic inhibition of Ia terminals | Active (depresses reflex) | Reduced |
| Reciprocal Ia inhibition of antagonists | Normal | Reduced |
| Ib autogenic inhibition (GTO) | Active | Reduced threshold for release |
| γ-motor neuron bias | Balanced | Tonically elevated |
| Descending noradrenaline/serotonin | Modulated | Excess at spinal level |
The net effect: Ia afferents are hypersensitised (pre-loaded by γ-overactivity), presynaptic inhibition fails to dampen their signal, and the α-motor neuron pool fires near-threshold at rest — so even modest stretch produces large reflex contractions.
Key References
- Guyton and Hall Textbook of Medical Physiology — Receptor function of the muscle spindle
- Ganong's Review of Medical Physiology, 26th ed. — Muscle tone & clasp-knife effect
- Costanzo Physiology, 7th ed. — Stretch reflex, Golgi tendon reflex, clasp-knife reflex
- Adams and Victor's Principles of Neurology, 12th ed. — Spasticity, hyperreflexia and the Babinski sign
- Bradley and Daroff's Neurology in Clinical Practice — Spasticity and Group II afferents
This is a shared conversation. Sign in to Orris to start your own chat.