Teach me everything about anemia from harrisons
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Loading Image
I now have everything needed from Harrison's to write a comprehensive, well-organized teaching guide. Here is the complete lesson:
Anemia - Everything from Harrison's Principles of Internal Medicine (22nd Ed., 2025)
1. Definition
Anemia is defined as blood counts below normal for a given population. In practical terms, this means low hemoglobin and hematocrit detected on a complete blood count (CBC).
- Harrison's, Ch. 66
2. Classification
Harrison's presents two complementary classification systems:
A. By Red Cell Size (MCV)
| Category | MCV | Causes |
|---|---|---|
| Microcytic | Low | Thalassemia, Iron deficiency, Anemia of chronic disease/inflammation, Sideroblastic anemias |
| Macrocytic - Oval macrocytes | High | B12 deficiency, Folate deficiency, Medications (chemo, anti-seizure), Myelodysplasia |
| Macrocytic - Round macrocytes | High | Alcohol use, Dysproteinemia, Hypothyroidism, Hypoxia, Liver disease, Reticulocytosis, Smoking |
| Normocytic | Normal | Aplastic anemia, Endocrinopathies, Marrow invasion, Myeloma, Pure red cell aplasia, Renal disease |
The key insight: microcytosis always reflects impaired hemoglobin production - less hemoglobin means smaller cells. Thalassemia causes a defect in globin chain synthesis; iron deficiency prevents heme synthesis; sideroblastic anemias have defects in heme synthesis; anemia of chronic disease blocks iron delivery.
B. By Mechanism (Reticulocyte-Based)
The reticulocyte count is the critical first indicator:
Elevated reticulocyte count → Loss or destruction of RBCs:
- Bleeding
- Hemolysis (acquired: autoimmune, mechanical; congenital: hemoglobinopathies, enzyme defects, membrane defects)
Low/inappropriately normal reticulocyte count → Underproduction:
- Nutritional deficiency (iron, B12, folate, copper, Vitamin C)
- Absence of red cell precursors (aplastic anemia, pure red cell aplasia)
- Lack of erythropoietin (renal disease, anemia of inflammation, anemia of aging)
- Marrow replacement (infection, cancer, granulomas)
- Stem cell defects (myelodysplasia, leukemia)
At least 75% of all cases of anemia are hypoproliferative. The most common cause is mild to moderate iron deficiency or inflammation.
- Harrison's, Ch. 66
3. Signs & Symptoms
Signs and symptoms are unreliable predictors of hematocrit level. Patients who develop anemia gradually over months can tolerate amazingly low hemoglobin.
Key features:
- Tiredness, shortness of breath (reduced O2 delivery)
- Pallor of mucosa and conjunctiva
- Resting tachycardia
- In atherosclerosis: angina, TIA, or stroke from ischemic symptoms
- In nutritional deficiency: pica (iron), neuropathy (B12)
- Flow murmur on cardiac auscultation
- Harrison's, Ch. 66
4. Compensatory Mechanisms
The body compensates through three physiologic mechanisms:
| Mechanism | Timeframe | How it works |
|---|---|---|
| Increased cardiac output | Minutes | O2 delivery = cardiac output × Hgb; if Hgb falls, CO rises. Limits the symptoms in cardiac-compromised patients |
| Increased 2,3-DPG | Hours to days | 2,3-diphosphoglyceric acid stabilizes deoxyHgb, reducing O2 affinity. This increases O2 delivery to tissues (Bohr effect analogy). High alveolar pO2 still ensures full oxygenation |
| Increased plasma volume | Weeks | Preserves cardiac output and BP; lowers viscosity. Can overwhelm the heart → edema and heart failure |
The implication: inherited or slowly-developing anemias are better tolerated than acute ones.
- Harrison's, Ch. 66
5. Laboratory Evaluation
The CBC
Electronic cell counters directly measure:
- Red cell number/L
- MCV (mean corpuscular volume)
- Hemoglobin
Derived values:
- Hematocrit = (RBC count × MCV) / 10
- MCH (mean corpuscular hemoglobin) = Hgb / RBC count
- MCHC (mean corpuscular hemoglobin concentration) = Hgb / Hematocrit
- RDW (red cell distribution width) = standard deviation of RBC size / MCV × 100 (normal ~11.5-14.5%)
Iron Studies
| Test | Normal Range | Significance |
|---|---|---|
| Serum iron | 9-27 μmol/L (50-150 μg/dL) | Available iron |
| TIBC | 54-64 μmol/L (300-360 μg/dL) | Iron-binding capacity (reflects transferrin) |
| Transferrin saturation | 25-50% | Iron:TIBC × 100 |
| Serum ferritin | 15-200 μg/L (men), 15-150 μg/L (women) | Iron stores |
In iron deficiency: low ferritin, low serum iron, elevated TIBC, low transferrin saturation, high RDW.
Reticulocyte Count
The production index corrects for anemia severity:
Reticulocyte Production Index (RPI) = (% reticulocytes × patient Hct / normal Hct) / maturation factor
An RPI >2 suggests increased production (hemolysis/bleeding); <2 suggests underproduction.
Blood Smear - Key Morphologic Findings
A review of the blood smear is a critical part of any evaluation for anemia.
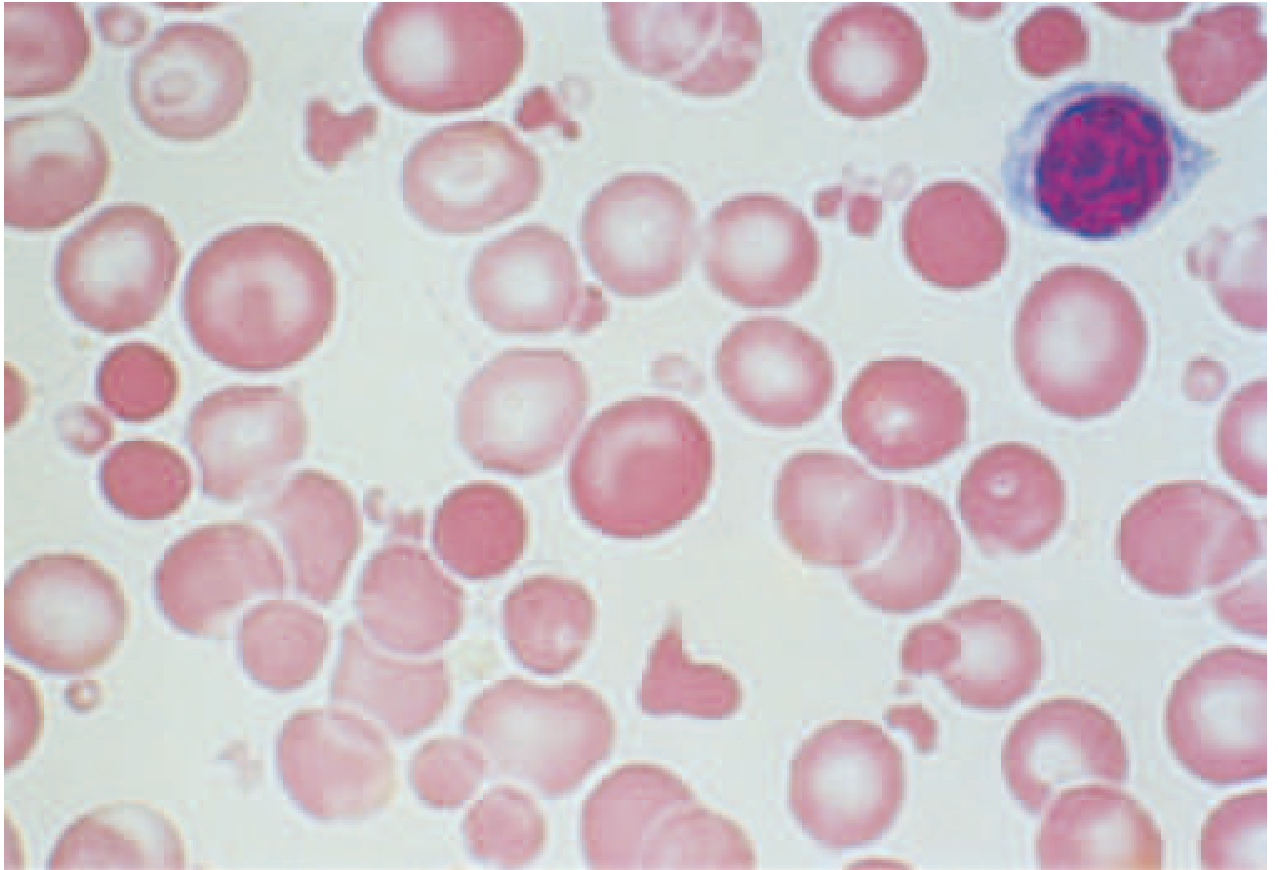
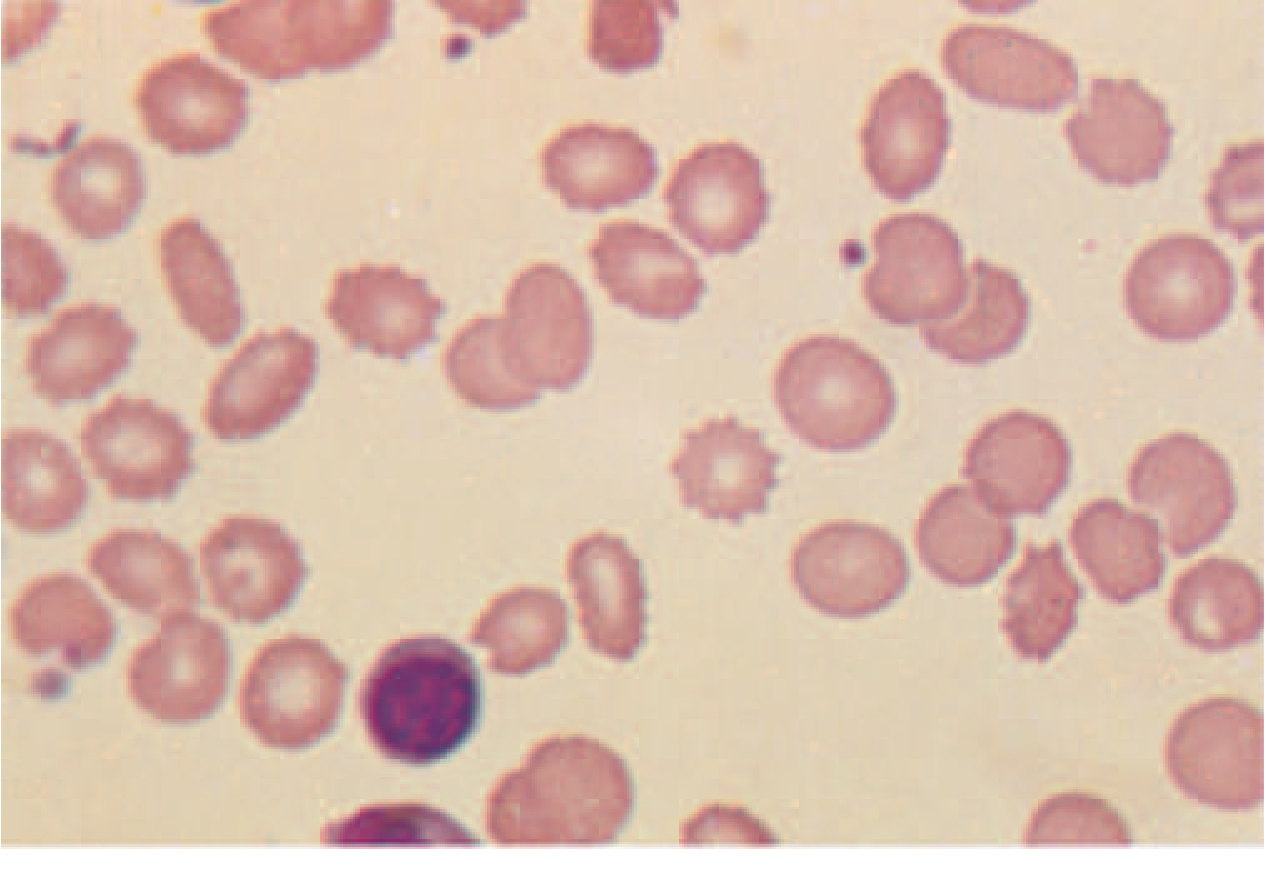
| Morphology | Description | Associated Conditions |
|---|---|---|
| Schistocytes | Fragmented RBCs disrupted by fibrin/platelet blockage or external forces | TTP, HUS, DIC, prosthetic heart valves, thermal injury |
| Echinocytes (burr cells) | Small, regularly-spaced spiny projections | Uremia, artifact |
| Acanthocytes (spur cells) | Irregular thorn-like projections | Liver disease, abetalipoproteinemia |
| Macro-ovalocytes | Large, oval-shaped RBCs | B12/folate deficiency, certain drugs, bone marrow disorders |
| Nucleated RBCs | Nucleus retained (normally cleared by spleen) | Asplenia, severe marrow stress, marrow fibrosis |
| Spherocytes | Small, dense, no central pallor | Hereditary spherocytosis, autoimmune hemolytic anemia |
- Harrison's, Ch. 66
6. Specific Causes of Anemia
6a. Iron Deficiency Anemia
The most common nutritional deficiency worldwide. Particularly prevalent in premenopausal women due to obligate menstrual losses.
Pathophysiology: Iron is essential - 4 atoms per hemoglobin molecule, ~1 billion iron atoms per red cell. Depletion proceeds in stages:
- Depletion of iron stores (ferritin falls)
- Iron-deficient erythropoiesis (transferrin saturation falls, RDW rises)
- Iron-deficiency anemia (hemoglobin falls, microcytic hypochromic picture)
Prevention: Special concern in:
- Low- to middle-income countries (malnutrition + helminth infections)
- Malaria-endemic regions (iron supplementation paradox - iron deficiency confers some protection from malaria; WHO recommends iron supplementation only when concomitant malaria prevention strategies are in place)
- Frequent blood donors (each unit contains ~200 mg iron)
- Pre-surgical patients: preoperative IV iron preferred if surgery is within 6 weeks
- Harrison's, Ch. 102
6b. Anemia of Inflammation (Anemia of Chronic Disease)
The preferred term is now "anemia of inflammation" because acute conditions (sepsis, trauma, major surgery) share the same mechanisms. It spans from hyperacute (macrophage activation syndrome) to subclinical (CHF, diabetes, obesity).
Three cytokine-driven mechanisms:
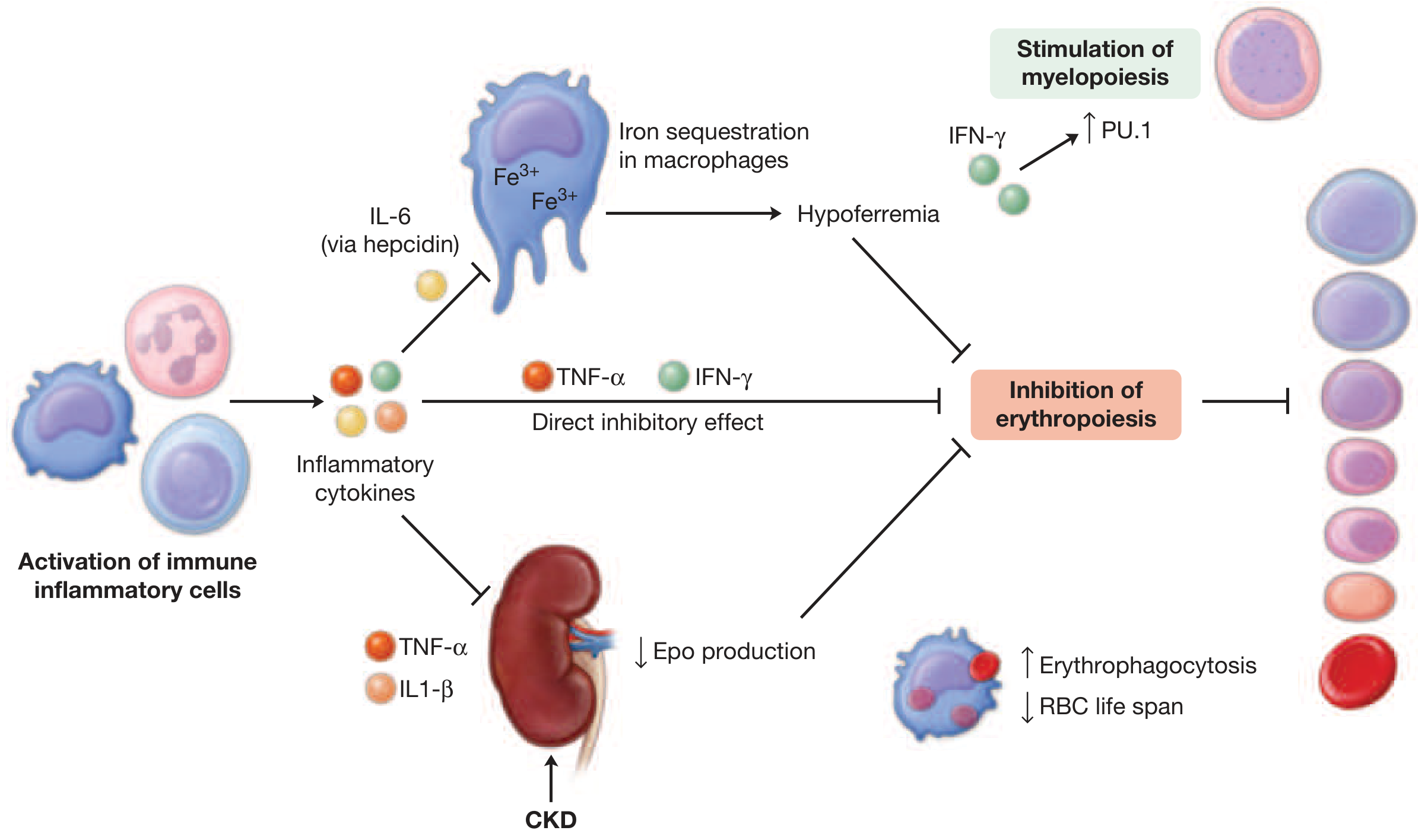
- IL-6 → hepcidin → macrophage iron sequestration → hypoferremia (iron trapped, unavailable for erythropoiesis)
- TNF-α and IL-1β → suppressed EPO production from kidneys
- IFN-γ → blunted erythroid progenitor response to EPO
- Bonus: bone marrow progenitor commitment is reprogrammed toward myeloid lineage (via PU.1 transcription factor)
Lab findings: Low serum iron, low TIBC (unlike iron deficiency where TIBC is high), normal/high ferritin, low transferrin saturation. Often normocytic but can be microcytic.
Treatment:
- Treat the underlying disorder (anti-IL-6 agents such as tocilizumab work in rheumatoid arthritis/Castleman's disease)
- ESAs (erythropoiesis-stimulating agents) in CKD - target Hgb <11.5 g/dL
- IV iron: maintain transferrin saturation 30-40%, ferritin 200-700 μg/L in CKD
- Ferric citrate (oral): binds intestinal phosphate, provides iron, reduces phosphate (useful in advanced CKD)
- Prolyl hydroxylase inhibitors (HIF-stabilizers): approved in some countries - stabilize HIF-2α, upregulate both EPO and duodenal iron absorption
- In CHF: IV iron if ferritin <100 μg/L or transferrin saturation <20% with ferritin 100-300 μg/L
- Harrison's, Ch. 102
6c. Anemia of Aging
- Prevalence: ~10% at age 65, ~25% in >85-year-olds, ~50% in hospitalized/institutionalized elderly
- Typically mild (Hgb 11-12 g/dL), multifactorial, often underestimated
- Negative impact on quality of life, muscle weakness, falls, fractures, and independent mortality association
- Black patients experience adverse effects at Hgb levels ~1 g/dL lower than white patients
Causes (each ~1/3):
- Nutritional (especially iron deficiency)
- Inflammation including CKD
- "Unexplained anemia of aging" - testosterone decline (males), stem cell exhaustion, EPO reduction
Special considerations:
- Ferritin cutoff for iron deficiency in elderly is higher (45-70 μg/L vs standard lower cutoffs)
- Gastrointestinal malignancy must always be ruled out
- Aspirin for primary CV prevention in elderly → 20% higher risk of anemia/iron deficiency vs placebo
- Harrison's, Ch. 102
6d. Acquired Hemolytic Anemia
Markers of hemolysis:
- Elevated LDH (abundant in RBCs)
- Low haptoglobin (scavenges free hemoglobin - exhausted when hemolysis is ongoing)
- Elevated blood/urine free hemoglobin (hemoglobinuria)
- Elevated reticulocyte count
- Abnormal smear (schistocytes, spherocytes)
Causes:
1. Mechanical destruction:
- March hemoglobinuria (marathon runners, barefoot ritual dancing, bongo drum playing) - acute, self-inflicted intravascular hemolysis
- Prosthetic heart valves (chronic, microangiopathic) - especially with paraprosthetic regurgitation
2. Infection:
- Malaria - the most frequent infectious cause in endemic areas
- Shiga toxin-producing E. coli O157:H7 - the main cause of HUS (more common in children)
- Clostridium perfringens - life-threatening intravascular hemolysis via lecithinase toxin; seen with open wounds, septic abortion, or contaminated blood units
3. Immune hemolytic anemias:
Two mechanisms:
- Drug-related (innocent bystander) - antibody vs drug catches RBCs in the reaction
- True autoimmune - antibody directly against RBC antigen
Two types by thermal amplitude:
| Type | Antibody | Clinical |
|---|---|---|
| Warm AIHA | IgG, reacts at body temperature (37°C) | Chronic, extravascular hemolysis, spherocytes on smear, treat with steroids/rituximab/splenectomy |
| Cold agglutinin disease | IgM (usually), reacts at cold temperatures (<30°C) | Acrocyanosis, Raynaud's, intravascular hemolysis; avoid cold; treat with rituximab |
- Harrison's, Ch. 105
6e. Anemia Due to Acute Blood Loss
Three clinical/pathophysiologic stages:
-
Hypovolemia dominates - the CBC does NOT show anemia yet (hemoglobin concentration unchanged acutely). Clinical signs: tachycardia, tachypnea, decreased pulse pressure, cold pale mottled skin, decreased urine output. Threat to brain and kidneys from hypoperfusion.
-
Hemodilution phase - baroreceptors/stretch receptors trigger vasopressin; fluid shifts from extravascular to intravascular compartment. Hypovolemia converts to anemia. Rule of thumb: if Hgb is 7 g/dL at 3 days, approximately half of total blood volume has been lost.
-
Bone marrow response - elevated reticulocytes and EPO as marrow compensates.
Signs of vascular instability appear with acute loss of ≥25% of total blood volume.
Diagnostic clues for internal bleeding:
- Grey Turner sign (flank ecchymosis) → retroperitoneal bleeding
- Cullen sign (umbilical ecchymosis) → intraperitoneal/retroperitoneal bleeding
- Dullness to chest percussion → intrapleural bleeding
- Harrison's, Ch. 106
6f. Aplastic Anemia & Bone Marrow Failure
- Normocytic anemia from absence of red cell precursors
- Pan-cytopenia (all cell lines affected)
- Diagnosis by bone marrow biopsy
- Treatment: immunosuppression (anti-thymocyte globulin + cyclosporine) or hematopoietic stem cell transplant
- Harrison's, Ch. 107
7. Stepwise Approach to Diagnosis
Four initial steps:
-
History: Previous anemia, prior therapy (iron, transfusions), family history, blood donation, menstrual history (duration, pad/tampon use, clots), symptoms of underlying disease (diarrhea → celiac/IBD)
-
Physical exam: Cardiac flow murmur (consequence), splenomegaly (hemolysis), blood in stool (GI bleeding as cause)
-
Blood smear + reticulocyte count: Morphology points to specific causes; reticulocyte count assesses bone marrow function
-
Guided workup (see algorithm below):
Reticulocyte count
│
├── HIGH → Hemolysis or Bleeding
│ ├── LDH, haptoglobin, direct antibody test (Coombs)
│ ├── Smear: schistocytes → microangiopathic
│ ├── Smear: spherocytes → AIHA or hereditary spherocytosis
│ └── Hemoglobin electrophoresis if sickle cells/thalassemia suspected
│
└── LOW/NORMAL → Underproduction → Guided by MCV
│
├── LOW MCV (microcytic)
│ ├── Check ferritin first
│ │ ├── Low ferritin → Iron deficiency
│ │ └── Normal ferritin → Consider thalassemia
│ └── RDW helps: high RDW = iron deficiency; low/normal RDW = thalassemia
│ Anemia of inflammation = diagnosis of exclusion (usually normocytic)
│
├── HIGH MCV (macrocytic) → Guided by smear
│ ├── Hypersegmented neutrophils + macro-ovalocytes → B12/folate levels
│ ├── Macro-ovalocytes with normal B12/folate → Myelodysplasia → bone marrow biopsy
│ └── Round macrocytes → History (liver disease, alcohol, hypothyroidism)
│
└── NORMAL MCV (normocytic)
├── Renal function (EPO deficiency)
├── EPO levels
├── Screen for underlying systemic diseases
└── Bone marrow exam if no cause found
- Harrison's, Ch. 66
8. Treatment Principles
Urgent indications for transfusion:
- Hypotension
- Signs of cardiac compromise (angina)
- Bone marrow failure (support while awaiting definitive therapy)
Restrictive transfusion thresholds are now standard in ICU: hemoglobin 7-8 g/dL for hemodynamically stable patients.
Cause-specific treatments:
- Iron deficiency → oral or IV iron (IV preferred preoperatively if surgery <6 weeks)
- B12 deficiency → B12 supplementation
- Folate deficiency → folate supplementation
- Anemia of inflammation/CKD → ESAs + IV iron
- Hemolytic anemias → treat underlying cause; AIHA → steroids/rituximab
- Aplastic anemia → immunosuppression or bone marrow transplant
Newer targeted therapies (Harrison's 22E highlights):
- Recombinant EPO - transformed CKD patients on dialysis; reduces transfusion needs in chemotherapy patients
- TGF-β inhibitors (luspatercept) - myelodysplastic syndrome-related anemia
- Complement inhibitors (eculizumab/ravulizumab) - paroxysmal nocturnal hemoglobinuria (PNH) and atypical HUS (aHUS); can be discontinued once full remission is achieved (urine dipstick negative for hemoglobinuria for 3-6 months)
- Prolyl hydroxylase inhibitors (HIF-stabilizers) - approved in some countries for renal anemia, providing both EPO stimulation and improved iron absorption in a single oral drug
- Hepcidin-ferroportin axis inhibitors - under investigation for anemia of inflammation
- Harrison's, Ch. 66, 102, 105
9. Quick Summary Table
| Type | MCV | Reticulocytes | Key Lab Finding | Classic Clue |
|---|---|---|---|---|
| Iron deficiency | Low | Low | Low ferritin, high TIBC, high RDW | Premenopausal women, GI bleeding |
| Thalassemia | Low | Low/Normal | Normal ferritin, low RDW | Family history, ethnicity |
| Anemia of inflammation | Normal/Low | Low | Normal/high ferritin, low TIBC | Chronic disease (cancer, infection, autoimmune) |
| B12 deficiency | High | Low | Low B12, hypersegmented neutrophils, macro-ovalocytes | Neuropathy, vegan diet, pernicious anemia |
| Folate deficiency | High | Low | Low folate, no neuropathy | Alcoholism, pregnancy, poor diet |
| Hemolytic anemia | Normal | High | High LDH, low haptoglobin | Jaundice, splenomegaly, abnormal smear |
| Aplastic anemia | Normal | Low | Pancytopenia, hypocellular marrow | Bone marrow biopsy |
| Acute blood loss | Normal → Low | High (delayed) | Normal Hgb initially | Trauma, GI bleed, tachycardia |
| Renal/CKD anemia | Normal | Low | Low EPO, elevated creatinine | CKD patient |
All content sourced from Harrison's Principles of Internal Medicine, 22nd Edition (2025, McGraw Hill Medical) - Chapters 66, 102, 105, 106, and 107.
This is a shared conversation. Sign in to Orris to start your own chat.