Urinary bladder innervation and types of bladder
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
I have enough material for a comprehensive answer. Here is the full response:
Urinary Bladder Innervation and Types of Bladder
Innervation of the Urinary Bladder
The lower urinary tract (LUT) receives three types of innervation: parasympathetic, sympathetic, and somatic, all coordinated by higher centers in the brainstem and cerebral cortex.
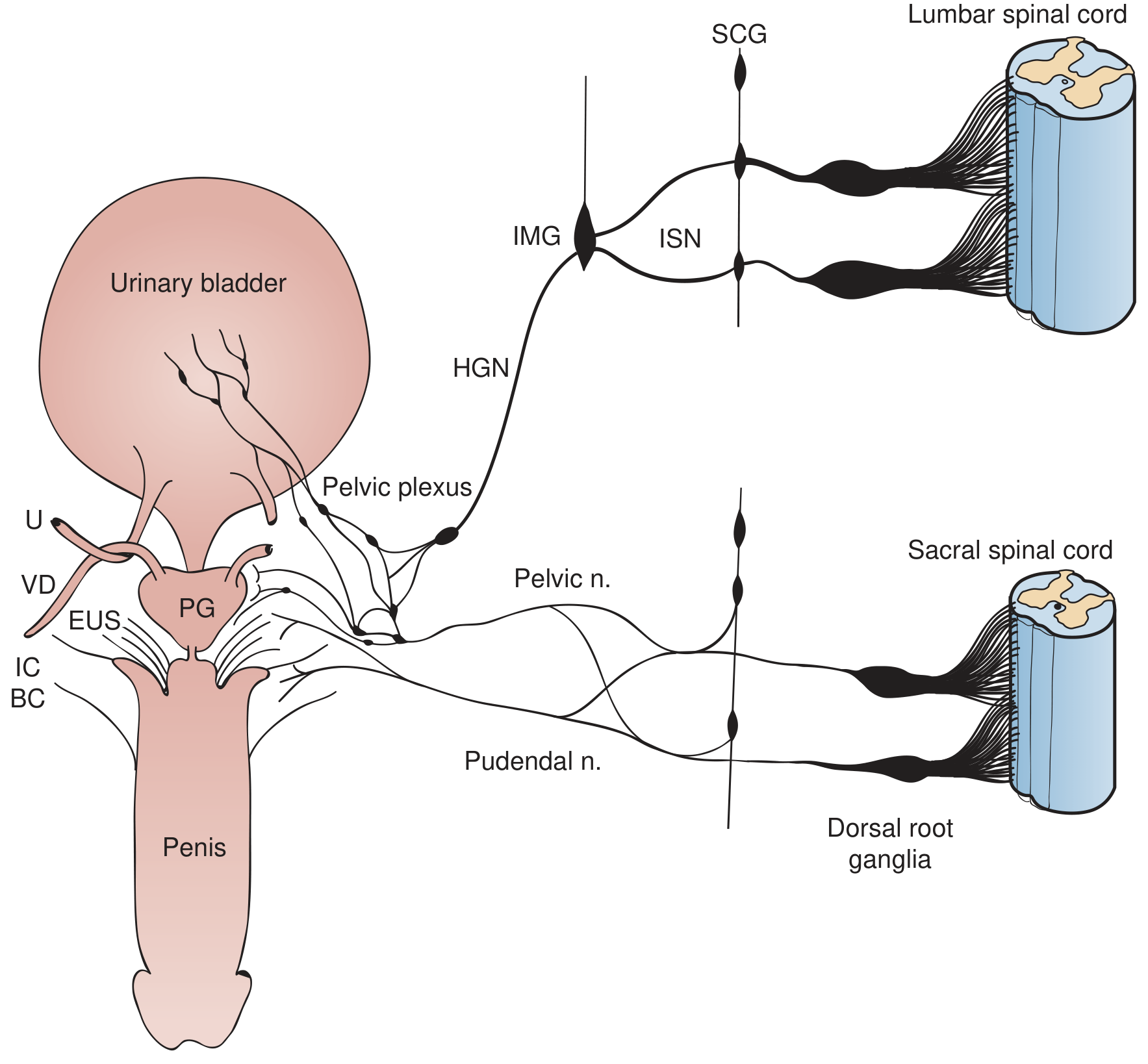
Fig. 110.22 - Campbell-Walsh Wein Urology: Sympathetic preganglionic pathways emerge from the lumbar spinal cord → sympathetic chain ganglia (SCG) → inferior splanchnic nerves (ISN) → inferior mesenteric ganglia (IMG) → hypogastric nerve (HGN) → pelvic plexus. Parasympathetic preganglionic axons originate in the sacral spinal cord and pass via the pelvic nerve. The pudendal nerve carries somatic fibers to the external urethral sphincter (EUS).
1. Parasympathetic Innervation (Motor - Voiding)
- Origin: Sacral parasympathetic nucleus, spinal cord segments S2, S3, S4
- Pathway: Pre-ganglionic fibers exit via the pelvic splanchnic nerves (nervi erigentes) → synapse at ganglia near or within the detrusor wall → short post-ganglionic fibers innervate the detrusor muscle
- Neurotransmitter: Acetylcholine (ACh) stimulating M3 muscarinic receptors on the detrusor (M2 is more abundant but M3 drives contraction)
- Function: Detrusor contraction (bladder emptying/voiding)
- Note: Parasympathetic postganglionic neurons in humans are located both in the detrusor wall and in the pelvic plexus - patients with cauda equina injuries may retain some innervation via intramural ganglia
2. Sympathetic Innervation (Storage)
- Origin: Thoracolumbar spinal cord, segments T10 to L2
- Pathway: Pre-ganglionic fibers → sympathetic chain ganglia (SCG) → inferior splanchnic nerves (ISN) → inferior mesenteric ganglia (IMG) → hypogastric nerves (HGN) → pelvic plexus/ganglia → bladder and urethra
- Neurotransmitters and receptors:
- Beta-3 (β3) adrenergic receptors on the detrusor body: noradrenaline causes detrusor relaxation (storage)
- Alpha-1 (α1) adrenergic receptors on the bladder neck and urethra: noradrenaline causes smooth muscle contraction (continence)
- Dense α1-receptors are present at the bladder neck in males - important for antegrade ejaculation and continence
- Function: Facilitates urine storage by relaxing the bladder body and contracting the outlet
3. Somatic Innervation (Voluntary Sphincter Control)
- Origin: Onuf's nucleus, ventral horn of sacral spinal cord (S2, S3, S4)
- Pathway: Via the pudendal nerve
- Target: External urethral sphincter (EUS), pelvic floor muscles (levator ani)
- Neurotransmitter: ACh acting on nicotinic receptors at the neuromuscular junction (striated muscle)
- Function: Voluntary contraction of the external sphincter (maintaining continence) and voluntary relaxation during micturition
4. Afferent (Sensory) Pathways
- From the bladder wall: Stretch receptors signal bladder filling via A-delta (myelinated, tension) and C fibers (unmyelinated, pain/temperature)
- Route: Travel with the hypogastric plexus → dorsal root ganglia → spinal cord
- Stretch signals from the posterior urethra are particularly strong in triggering the micturition reflex
- Afferent signals ascend to the Pontine Micturition Center (PMC) in the brainstem, which coordinates bladder-sphincter synergy
- Higher control: Cerebral cortex and hypothalamus provide voluntary inhibition of micturition until socially convenient
5. Non-Adrenergic, Non-Cholinergic (NANC) Fibers
- Use purines (ATP) and nitric oxide as neurotransmitters
- Nitric oxide synthase-containing neurons found in the bladder neck and trigone - promote relaxation during voiding
- Contribution to normal contraction is small, but may become pharmacological targets in pathological states
Summary Table
| System | Spinal Level | Nerve | Receptor | Action |
|---|---|---|---|---|
| Parasympathetic | S2-S4 | Pelvic nerve | M3 muscarinic | Detrusor contraction (voiding) |
| Sympathetic | T10-L2 | Hypogastric nerve | β3-adrenergic (body) | Detrusor relaxation (storage) |
| Sympathetic | T10-L2 | Hypogastric nerve | α1-adrenergic (neck/urethra) | Outlet contraction (continence) |
| Somatic | S2-S4 | Pudendal nerve | Nicotinic | EUS contraction (continence) |
Types of Bladder (Lapides Classification - Neurogenic Bladder)
The classic Lapides Classification (1970) - a modification of McLellan's 1939 system - is the most widely used descriptive framework for neurogenic bladder types:
1. Sensory Neurogenic Bladder
- Lesion: Selective interruption of sensory (afferent) fibers between bladder and spinal cord/brain
- Common causes: Diabetes mellitus, tabes dorsalis, pernicious anemia
- Clinical features: Impaired sensation of bladder distension; voiding must be initiated by timed schedule
- Cystometry: Large-capacity bladder, flat high-compliance low-pressure filling curve; large residual urine if voiding is neglected
2. Motor Paralytic Bladder (Motor Neurogenic Bladder)
- Lesion: Destruction of parasympathetic motor innervation (efferent fibers)
- Common causes: Extensive pelvic surgery or trauma, herpes zoster
- Clinical features: Ranges from painful urinary retention to inability to maintain normal voiding; no voluntary detrusor contraction
- Cystometry: Normal filling curve initially, but no detrusor contraction at capacity; chronic overdistension leads to large-capacity flat low-pressure bladder
3. Uninhibited Neurogenic Bladder
- Lesion: Damage to the corticoregulatory tract (upper motor neuron lesion above sacral micturition center) - loss of cortical inhibition
- Common causes: CVA (stroke), brain or spinal cord tumor, Parkinson's disease, demyelinating disease (MS)
- Clinical features: Urgency, frequency, urge incontinence; patient can usually initiate voiding voluntarily but cannot hold
- Cystometry: Normal sensation with involuntary detrusor contractions at low filling volumes; low residual urine
4. Reflex Neurogenic Bladder
- Lesion: Complete interruption of sensory and motor pathways between sacral spinal cord and brainstem (suprasacral spinal cord lesion) - equivalent to complete upper motor neuron (UMN) lesion
- Common causes: Traumatic spinal cord injury, transverse myelitis, extensive demyelinating disease
- Clinical features: No bladder sensation; no voluntary voiding; incontinence without sensation; detrusor-sphincter dyssynergia (DSD) is the rule
- Cystometry: Involuntary contractions at low volumes; no voluntary control
5. Autonomous Neurogenic Bladder
- Lesion: Complete motor AND sensory separation from the sacral spinal cord (destruction of sacral cord, sacral roots, or pelvic nerves) - equivalent to complete lower motor neuron (LMN) lesion
- Common causes: Sacral cord destruction (tumors, trauma), cauda equina injuries, radical pelvic surgery
- Clinical features: Cannot initiate micturition, no reflex activity, no bladder sensation; bladder empties only by abdominal straining or manual compression (Crede maneuver)
- Cystometry: Flat filling curve; no detrusor contractions; large residual urine
Clinical Correlations by Spinal Level
| Level of Lesion | Bladder Type | Key Feature |
|---|---|---|
| Above brainstem (cortex/cerebellum) | Uninhibited neurogenic | Detrusor overactivity (urgency/urge incontinence) |
| Between brainstem and sacral cord (suprasacral) | Reflex neurogenic | Detrusor overactivity + DSD; risk of autonomic dysreflexia if above T6 |
| Sacral cord / cauda equina | Autonomous neurogenic | Detrusor areflexia, urinary retention |
| Selective sensory damage | Sensory neurogenic | Overflow incontinence; no urge sensation |
| Selective motor damage | Motor paralytic | Retention without sensation |
Sources:
- Campbell-Walsh Wein Urology - Innervation of the Bladder, Lapides Classification (Ch. 110-111)
- Bailey and Love's Short Practice of Surgery, 28th ed. - Innervation of the Bladder (Ch. 83)
- Berek & Novak's Gynecology - Innervation of the Bladder and Urethra (Ch. 29)
- Guyton and Hall Textbook of Medical Physiology - Physiological Anatomy and Innervation of the Bladder (Ch. 26)
- Mulholland and Greenfield's Surgery, 7th ed. - Neurogenic Bladder (Ch. 10)
This is a shared conversation. Sign in to Orris to start your own chat.