Hypocalcaemia management
Reading File
Finding Sources
Searching PubMed
"hypocalcemia"[MeSH Terms] AND "management"[MeSH Terms]
Finding Sources
Searching PubMed
"hypocalcemia" AND "treatment"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive, well-cited response.
Hypocalcaemia: Management
Definition & Diagnostic Thresholds
- Total serum calcium < 8.5 mg/dL (2.1 mmol/L); or ionised calcium < 4.4 mg/dL (1.1 mmol/L)
- Always correct for albumin: for every 1 g/dL drop in albumin below 4 g/dL, measured calcium falls ~0.8 mg/dL — but ionised calcium is not affected and is more accurate
- Ionised calcium < 0.8 mmol/L = severe; > 0.8 mmol/L = moderate
Diagnostic Approach
Use the algorithm below (based on serum albumin → urinary calcium → PTH → phosphate):
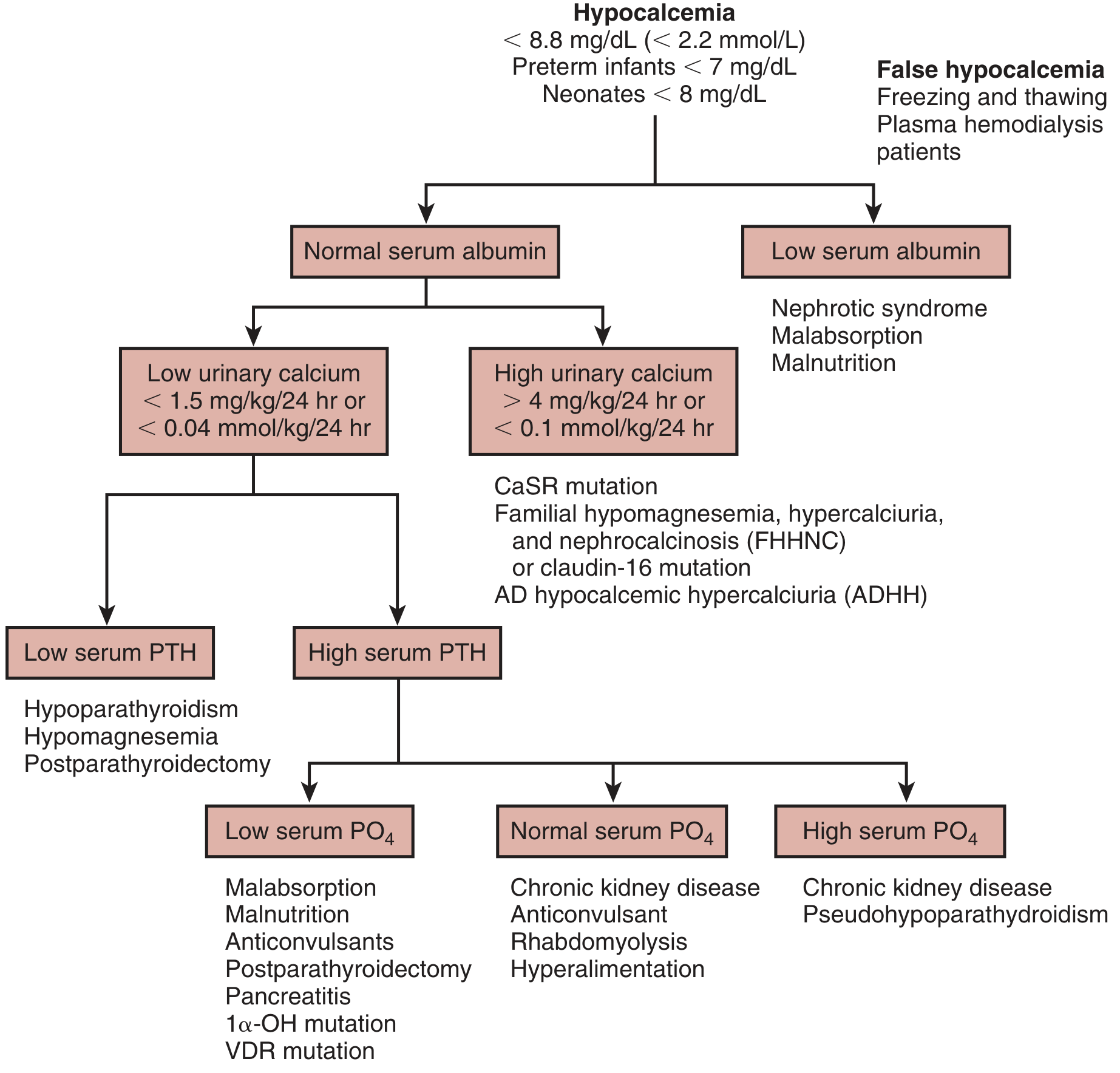
Key investigations: serum albumin, ionised calcium, phosphate, PTH, magnesium, creatinine, 25(OH)D, 24-hour urinary calcium.
Common Causes (Quick Reference)
| Category | Examples |
|---|---|
| Most common | Hypoalbuminaemia, chronic renal failure, hypomagnesaemia |
| PTH deficiency | Post-surgical (thyroidectomy/parathyroidectomy), autoimmune, infiltrative, DiGeorge syndrome |
| PTH resistance | Pseudohypoparathyroidism (Albright hereditary osteodystrophy) |
| Vitamin D | Deficiency (malnutrition, malabsorption, liver disease, lack of sunlight), VDR mutation |
| Acute causes | Pancreatitis, massive blood transfusion (citrate toxicity), rhabdomyolysis, tumour lysis syndrome, sepsis |
| Drugs | Bisphosphonates, phenytoin, calcitonin, cinacalcet, proton pump inhibitors |
| Other | Respiratory alkalosis (shifts ionised Ca²⁺ to bound state), hydrofluoric acid/ethylene glycol toxicity |
Clinical Features
Neuromuscular (predominant):
- Perioral and fingertip paraesthesias, muscle cramps, tetanic contractions
- Chvostek sign — facial twitching on tapping the facial nerve (less specific)
- Trousseau sign — carpal spasm when BP cuff inflated 20 mmHg above systolic for 3 minutes (more specific)
- Laryngospasm, bronchospasm, generalised seizures (severe)
Cardiovascular:
- QT prolongation (ST segment lengthening on ECG — can mimic MI)
- Dysrhythmias, hypotension, heart failure, cardiovascular collapse
- Calcium < 8.95 mg/dL carries a 2.3-fold higher risk of sudden cardiac death
Chronic features: cataracts, poor dentition, dry skin, coarse hair, extrapyramidal symptoms (in pseudohypoparathyroidism)
Management
Step 1 — Determine Severity
| Severity | Features | Approach |
|---|---|---|
| Mild / asymptomatic | Mildly low Ca, no symptoms | Oral supplementation |
| Moderate asymptomatic | Ionised Ca > 0.8 mmol/L, no tetany | IV calcium gluconate intermittent boluses |
| Severe / symptomatic | Tetany, seizures, dysrhythmia, ionised Ca < 0.8 mmol/L | IV calcium immediately |
Acute / Severe Symptomatic Hypocalcaemia
First-line: IV Calcium Gluconate (preferred over calcium chloride — less risk of tissue necrosis on extravasation)
- Initial bolus: 1–2 g calcium gluconate (10–20 mL of 10% solution) in 50 mL of 5% dextrose or normal saline, given IV over 10–20 minutes, with continuous ECG monitoring
- 10 mL of 10% calcium gluconate = 93 mg elemental calcium
- Maintenance infusion: 0.3–1.0 mg elemental Ca/kg/hour; titrate to keep calcium at the lower end of normal
- Ionised calcium should be rechecked every 4–6 hours initially
Calcium chloride (272 mg elemental Ca per 10 mL): more elemental calcium but caustic — use via central venous access only; reserve for critically ill without central line
ECG monitoring is mandatory throughout IV calcium therapy.
The infusion solution must not contain phosphates or bicarbonates (precipitation risk).
Moderate Asymptomatic Hypocalcaemia
- Repeat doses of 1–2 g calcium gluconate IV every 4 hours without continuous infusion
- Oral calcium and calcitriol can be started in parallel
Chronic / Maintenance Therapy (Oral)
Oral calcium salts — elemental calcium content varies:
| Salt | Elemental Ca content |
|---|---|
| Calcium carbonate | 40% (highest — preferred) |
| Calcium chloride | 36% |
| Calcium lactate | 12% |
| Calcium gluconate | 8% |
- Start at 500–1000 mg elemental calcium/day, increase up to 1000–2000 mg/day
- Target: low-normal serum calcium (correcting to full normal increases hypercalciuria risk)
Vitamin D — essential for chronic hypocalcaemia, especially hypoparathyroidism:
- Calcitriol (1,25-dihydroxyvitamin D) — active form, preferred in hypoparathyroidism and CKD; bypasses need for renal 1α-hydroxylation
- Colecalciferol (vitamin D3) or ergocalciferol — for nutritional deficiency
- Vitamin D receptor agonists are the conventional treatment for hypoparathyroidism
Thiazide diuretics — useful adjunct in hypoparathyroidism:
- Reduce urinary calcium excretion, thereby protecting against nephrocalcinosis/nephrolithiasis caused by high-dose calcium and active vitamin D
- Combine with low-salt diet for maximal effect
Treat Concurrent Electrolyte Abnormalities (Critical)
- Hypomagnesaemia must be corrected first — low Mg causes end-organ PTH resistance and inhibits PTH release, making hypocalcaemia refractory to treatment
- Oral: magnesium oxide/carbonate 100–300 mg elemental Mg/day
- IV: magnesium sulfate 20–40 mmol/day in D5W
- Hyperphosphataemia — correct with dietary phosphate restriction ± phosphate binders; consider dialysis if severe
- Alkalosis — correct respiratory or metabolic alkalosis, which worsens ionised hypocalcaemia by shifting Ca to bound state
Hypoparathyroidism-Specific Management
- Conventional: calcitriol + oral calcium ± thiazide
- PTH replacement (emerging/specialist):
- Teriparatide (PTH 1-34): 20 µg SC twice daily (off-label for hypoparathyroidism)
- PTH 1-84: 100 µg every other day; studied in 30 hypoparathyroid patients over 24 months with improvement/normalisation of calcium
- TransCon PTH (palopegteriparatide): Phase 3 RCT (PaTHway trial, 2025) showed efficacy and safety at 52 weeks [PMID: 39376010]
Post-Parathyroidectomy / "Hungry Bone Syndrome"
- Occurs after parathyroid or thyroid surgery due to massive calcium redistribution into bone
- Requires large doses of IV then oral calcium and active vitamin D for prolonged periods
- Monitor closely and frequently for rebound hypercalcaemia, hyperphosphataemia, and hypercalciuria
Special Populations
Neonates/Infants (symptomatic):
- Calcium gluconate 10% IV: 1 mL/kg (9 mg elemental Ca/mL) at 1 mL/min over 10 minutes; repeat as needed
- Continuous elemental Ca infusion: 1–3 mg/kg/hr if tetany/seizures persist
- If hypomagnesaemia: magnesium sulfate 50% solution, 0.1 mL/kg IV or IM
Asymptomatic infants: calcium carbonate oral, 50 mg elemental Ca/kg/day in 4 divided doses
Renal failure: use calcitriol (not standard vitamin D); monitor for hypercalciuria and hyperphosphataemia; dialysis if severe hyperphosphataemia
Monitoring
- Ionised calcium every 4–6 hours during IV therapy
- Serum Mg, phosphate, PTH, 25(OH)D — guide underlying cause
- ECG — monitor QT interval throughout acute management
- Once stable: regular outpatient monitoring to prevent hypercalciuria → nephrocalcinosis (especially in hypoparathyroidism)
Sources:
- Rosen's Emergency Medicine, 9th ed., Ch. 114
- Brenner and Rector's The Kidney, 2-Volume Set, Ch. 73
- Comprehensive Clinical Nephrology, 7th ed., Ch. 11
- Textbook of Family Medicine, 9th ed., Ch. 35
- Tintinalli's Emergency Medicine, Ch. 132
- TransCon PTH Phase 3 RCT (PaTHway trial) [PMID: 39376010] — 52-week data supporting PTH replacement in hypoparathyroidism
This is a shared conversation. Sign in to Orris to start your own chat.