Theories of phonation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Here is a thorough account of the theories of phonation, drawn from Cummings Otolaryngology, Scott-Brown's Otorhinolaryngology, and K.J. Lee's Essential Otolaryngology.
Theories of Phonation
Background
The role of the larynx in sound production has been recognized for centuries, but the precise mechanism by which it generates sound from exhaled air was not understood until the mid-20th century. Two major competing theories emerged, with the current understanding refined by the body-cover/mucosal wave model.
1. Neurochronaxic (Neurochroaxic) Theory - Husson, 1950
Proposed by Raoul Husson in 1950, this theory held that:
- Each single vibration (oscillation) of the vocal folds is triggered by a separate, discrete nerve impulse from the recurrent laryngeal nerve
- Glottic vibrations are caused by rhythmic nerve impulses that are synchronous with the frequency of sound produced
- The vocal folds would therefore contract actively with each cycle
Why it was rejected:
This is considered a physiologically impossible hypothesis. The human voice can reach frequencies of 1000 Hz or more (during falsetto), meaning the recurrent laryngeal nerve would have to fire 1000 times per second - far beyond the maximum firing rate of any motor nerve. Nerve conduction velocity and chronaxie measurements made this untenable. The theory has been largely discredited and is now of historical interest only.
(Cummings Otolaryngology, p. 1023)
2. Myoelastic-Aerodynamic Theory - Van den Berg, 1950s (Current Accepted Theory)
Proposed by Janwillem van den Berg in the 1950s after using high-speed motion pictures to document vocal fold motion, this is the currently accepted and widely endorsed theory of phonation.
The theory holds that vocal fold vibration results from the interaction of aerodynamic forces and the mechanical (myoelastic) properties of the laryngeal tissues. No active muscular contraction occurs with each vibratory cycle; the folds vibrate passively.
The Vibratory Cycle (Step by Step)
-
Pre-phonatory phase: The vocal folds abduct briefly for inspiration, then are rapidly adducted by contraction of the lateral cricoarytenoid muscles. The folds are positioned near the midline with a small gap.
-
Subglottic pressure builds: Exhaled air is forced against the adducted vocal folds. Subglottic pressure rises until it overcomes the resistance (myoelastic tension) of the adducted folds.
-
Inferior separation: The vocal folds are blown apart, beginning at their inferior border - the folds "peel apart" from the bottom upward.
-
Bernoulli effect: As air passes through the narrowed glottis, its velocity increases and lateral pressure drops (Bernoulli's principle). This negative pressure sucks the vocal fold mucosa back toward the midline.
-
Elastic recoil: The myoelastic forces (elastic tension in the vocal fold tissue) also contribute to the return of the folds to midline.
-
Closure: The inferior margins close first. When the vocal folds return to midline, subglottic pressure builds again and the cycle repeats.
Each cycle produces a puff of air released into the supraglottic vocal tract, generating the acoustic signal.
(Cummings Otolaryngology, p. 1023; K.J. Lee's Essential Otolaryngology, p. 916; Scott-Brown's Otorhinolaryngology, p. 945)
Requirements for Normal Phonation (Box 53.1 - Cummings)
- Adequate breath support
- Approximation of vocal folds (appropriate gap)
- Favorable vibratory properties (mucosal pliability)
- Favorable vocal fold shape (3D contour)
- Control of length and tension
3. Body-Cover Theory and the Mucosal Wave Model
A refinement of the myoelastic-aerodynamic theory, proposed by Hirano and elaborated further by others, including the two-mass model (Ishizaka and Flanagan).
The key insight is that the vocal fold is not a homogeneous structure and vibrates in three dimensions:
- Body: The vocalis muscle (thyroarytenoid) forms a firm, relatively static inner core
- Cover: The overlying mucous membrane (epithelium + superficial lamina propria) is loose and pliable, blown by the expiratory airstream
The mucosal wave is a traveling wave that propagates from the inferomedial surface upward (inferiorly to superiorly) along the vocal fold with each cycle:
- As the inferior edges separate, a puff of air is released
- The superior edges remain in contact briefly longer, creating a temporal lag
- This traveling wave can only be visualized using laryngostroboscopy or high-speed photography
The two-mass model explains why the superior and inferior edges of the vocal folds are out of phase: as the superior edges separate, divergent glottic airflow generates greater negative pressure at the lower edge, accelerating closure of the inferior glottis first.
(Cummings Otolaryngology, p. 1023; Scott-Brown's Otorhinolaryngology, p. 945)
The Vibratory Cycle - 4 Phases (Box 59.1 - Scott-Brown's)
| Phase | Description |
|---|---|
| Closing phase | Vocal folds begin to close rapidly from their lower margin |
| Closed phase | Medial edges in full contact |
| Opening phase | Folds separate from lower margin upward; superior margin remains last |
| Open phase | Folds are separated (the longest part of a normal cycle) |
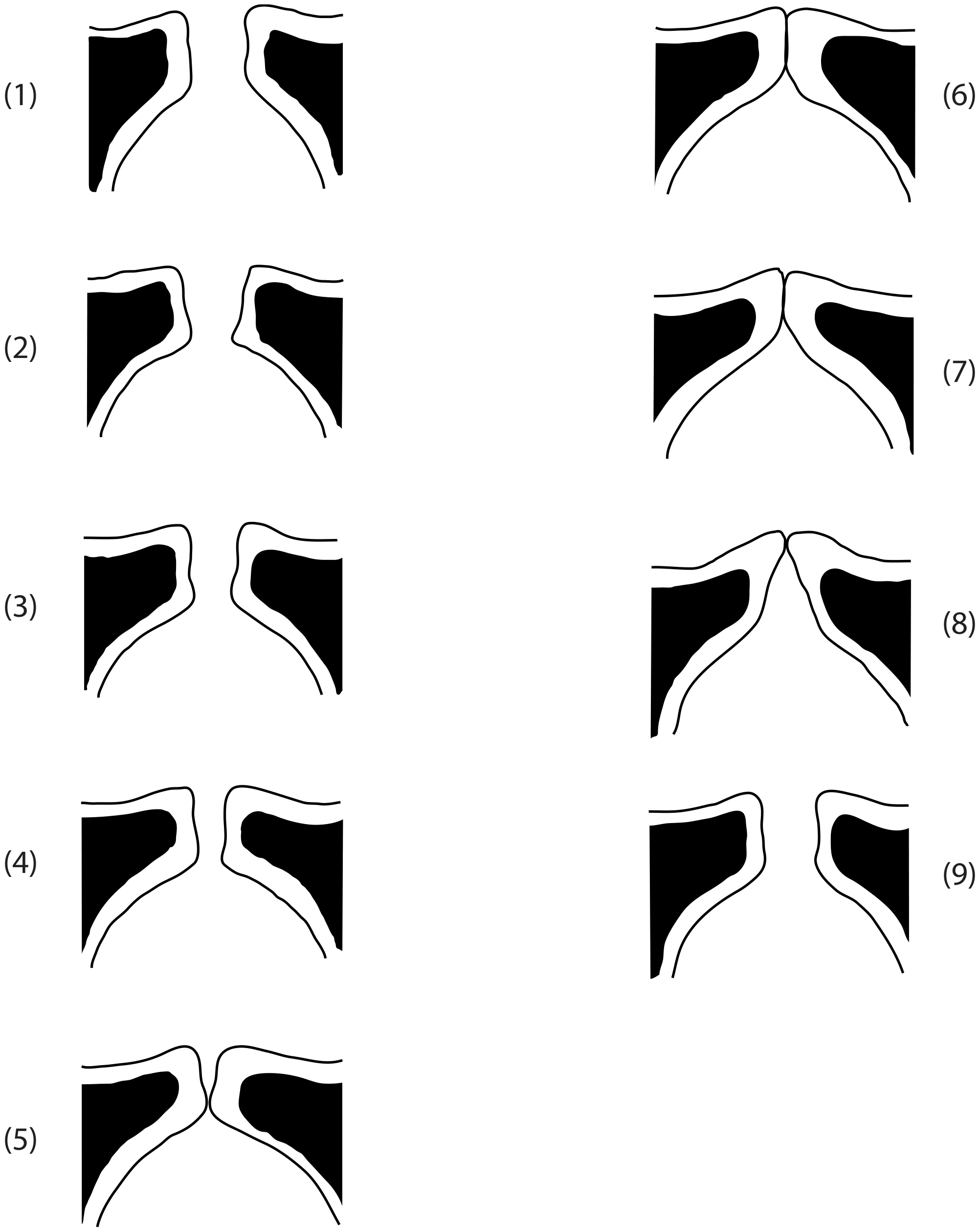
This 9-frame diagram shows the full vibratory cycle with the mucosal wave traveling from the inferior to superior aspect of each fold:
Variations by Register
| Register | Mechanism |
|---|---|
| Modal (chest voice) | Full mucosal wave; Bernoulli effect dominant in closing phase; body and cover move somewhat independently |
| Falsetto | Increased tension + decreased thickness; mucosal wave reduced/absent; elastic recoil is primary closing force; only superior edges make contact; short closing phase |
| Low pitch | Vocalis muscle relaxed; "body" participates in oscillation |
Summary Comparison
| Feature | Neurochronaxic Theory | Myoelastic-Aerodynamic Theory |
|---|---|---|
| Proposed by | Husson (1950) | Van den Berg (1950s) |
| Mechanism | Active nerve impulse per cycle | Passive aerodynamic + elastic forces |
| Role of muscles | Active contraction each cycle | Set tension; passive during vibration |
| Bernoulli effect | Not incorporated | Central to closure |
| Status | Discredited | Accepted (current standard) |
References:
- Cummings Otolaryngology Head and Neck Surgery, Section on Phonation, p. 1023
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, "The Biomechanics of Phonation" and "The Vibratory Cycle," p. 945
- K.J. Lee's Essential Otolaryngology, "Phonation," p. 916
This is a shared conversation. Sign in to Orris to start your own chat.