labor
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information for a complete answer. Let me compile it.
Labor (Parturition) - Obstetrics
Definition
Labor is the process of childbirth consisting of progressive uterine contractions that produce cervical effacement and dilation, leading to fetal expulsion and placental delivery. It is a continuous physiologic process divided into stages for clinical management. - The Developing Human: Clinically Oriented Embryology
True vs. False Labor
Before managing labor, the distinction between true and false labor must be made:
| Feature | True Labor | False Labor (Braxton Hicks) |
|---|---|---|
| Contraction rhythm | Regular | Irregular |
| Intervals | Gradually shorten | Unchanged |
| Intensity | Gradually increases | Unchanged |
| Discomfort location | Back AND abdomen | Lower abdomen only |
| Effect of sedation | No relief | Usually relieved |
| Cervical dilation | Yes | No |
False labor contractions do not produce cervical change and are treated with hydration and rest. - Tintinalli's Emergency Medicine
Stages of Labor
First Stage - Cervical Dilation
From the onset of regular uterine contractions to full cervical dilation (10 cm).
Divided into two phases:
- Latent phase: Irregular, infrequent contractions. Cervix softens, effaces, and dilates slowly. This is the preparatory phase.
- Active phase: Begins once the cervix reaches 3-4 cm dilation. Cervix dilates at:
- 1.2 cm/hour in nulliparous women
- 1.5 cm/hour in multiparous women
Average duration:
- Primigravidas (first birth): ~12 hours total
- Multigravidas: ~7 hours
Second Stage - Fetal Expulsion
From full dilation (10 cm) to delivery of the infant.
- Mean duration: 54 minutes for nulliparous women, 20 minutes for multiparous women
- The fetus descends through the cervix and vagina via the six cardinal movements
Third Stage - Placental Delivery
From delivery of the infant to expulsion of the placenta and membranes.
- Usually lasts <10 minutes; 90% complete within 15 minutes
- Active intervention typically not needed until >30 minutes
- A placenta not expelled within 60 minutes is classified as retained placenta
- After delivery, uterine retraction reduces the placental attachment area; a hematoma forms deep to the placenta and separates it from the uterine wall. Myometrial contractions constrict spiral arteries to prevent excessive bleeding.
(A fourth stage - the first 1-2 hours postpartum - is clinically recognized for monitoring maternal hemostasis.)
Cardinal Movements of Labor (Second Stage)
The fetal head negotiates the maternal pelvis through six movements in vertex presentation:
- Engagement - the widest diameter of the fetal head passes below the pelvic inlet
- Flexion - chin onto chest to present the smallest head diameter
- Descent - downward progress through the birth canal
- Internal rotation - head rotates to align with the anteroposterior pelvic outlet
- Extension - head extends under the pubic symphysis at delivery
- External rotation (restitution) - head rotates to align with fetal shoulders after delivery
- Tintinalli's Emergency Medicine, Textbook of Family Medicine 9e
Cervical Assessment
- Dilation: Diameter of the internal cervical os, 0 to 10 cm (full dilation)
- Effacement: Thinning/shortening of the cervix, expressed as a percentage
- Station: Level of the presenting fetal part relative to maternal ischial spines
- Above spines = negative station (-1, -2, -3)
- At spines = 0 station
- Below spines = positive station (+1, +2, +3)
- +3 station = fetal scalp visible at introitus (imminent delivery)
Rupture of Membranes
- Spontaneous rupture occurs in active labor in most patients; ~8% rupture before labor onset
- Confirmed by nitrazine paper (amniotic fluid pH 7.0-7.4 turns paper dark blue; vaginal pH 4.5-5.5 stays yellow)
- Also confirmed by ferning (NaCl crystals on dried amniotic fluid under microscopy)
- 50% of women with premature rupture deliver within 5 hours; 95% within 28 hours
Fetal Heart Rate (FHR) Monitoring
Normal FHR: 120-160 bpm. Bradycardia: <110 bpm. Tachycardia: >160 bpm.
Key FHR patterns:
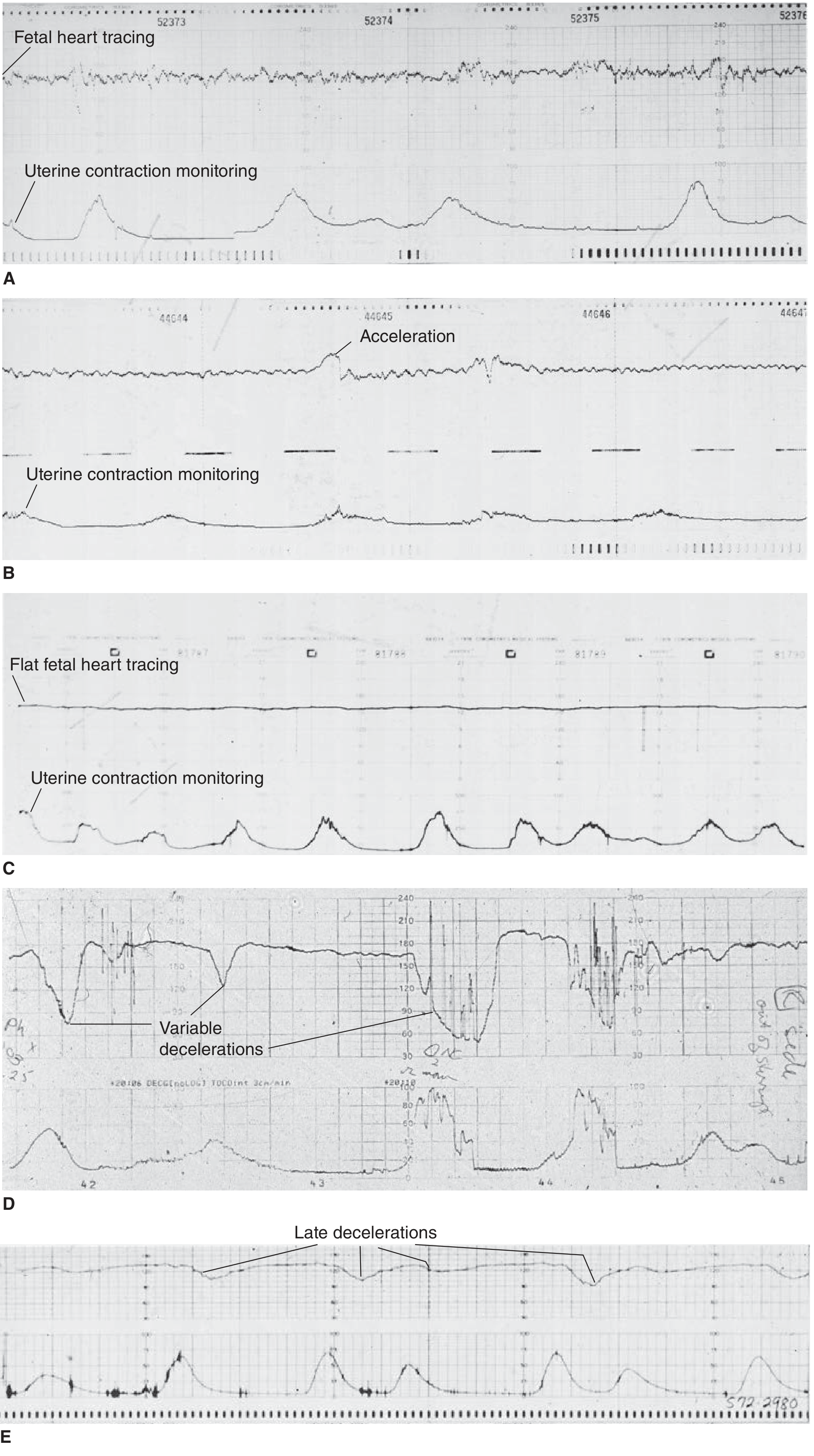
A = Good variability (reassuring) | B = Accelerations (reassuring) | C = Poor/flat variability (possible fetal hypoxia) | D = Variable decelerations (cord compression) | E = Late decelerations (uteroplacental insufficiency)
Late decelerations - drops in FHR both during and >30 seconds after a contraction - are ominous and indicate uteroplacental insufficiency and fetal hypoxia.
Management of fetal distress:
- Position mother in left lateral decubitus (reduces aortocaval compression)
- IV hydration
- Supplemental oxygen
- Emergency obstetric consultation
Initial Clinical Evaluation
When a patient >20 weeks presents with signs of labor, obtain:
- Maternal vital signs (BP, HR, RR, SpO2, temperature)
- Fetal heart rate (Doppler US)
- IV access, blood type, urinalysis
- History: contraction onset/frequency, membrane status, vaginal bleeding, fetal movement, parity, prior delivery complications, prenatal care, estimated due date
Nagele's Rule: EDD = first day of last menstrual period + 9 months + 7 days
Fundal height: In cm from pubic symphysis to fundal top = gestational age in weeks (±2 weeks) after 20 weeks
Delivery Steps & Post-Delivery
- Push only after full cervical dilation to avoid lacerations
- Episiotomy is not routine; reserve for fetal distress, shoulder dystocia, or instrumental delivery
- After delivery: keep infant warm, gentle stimulation; do not routinely suction nose/mouth (causes bradycardia)
- Delayed cord clamping: at least 1-3 minutes after birth (increases neonatal iron stores)
- Apgar scores at 1 and 5 minutes (color, tone, heart rate, respiratory effort, reflexes; score <7 requires action)
Sources:
- The Developing Human: Clinically Oriented Embryology (9780323611541)
- Tintinalli's Emergency Medicine: A Comprehensive Study (9781260019933)
- Creasy & Resnik's Maternal-Fetal Medicine (9780323828499)
- Textbook of Family Medicine, 9e (9780323239905)
This is a shared conversation. Sign in to Orris to start your own chat.