What is apparent and true shortening of the limb according to orthopedics in examination? Also explain the method of examination.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough answer. Here is the comprehensive response:
Apparent and True Shortening of the Limb in Orthopedic Examination
Definitions
True Shortening
True shortening is an actual reduction in the length of the bony segment(s) of the limb. It is measured between fixed bony landmarks - typically from the anterior superior iliac spine (ASIS) to the medial malleolus. True shortening occurs due to actual loss of bone length and is caused by:
- Fractures with overlap or comminution (e.g., fracture neck of femur)
- Dislocation of the hip
- Bone destruction (tuberculosis, Perthes' disease, septic arthritis)
- Congenital dislocation of the hip (CDH)
- Slipped capital femoral epiphysis (SCFE)
- Congenital coxa vara
- Acetabular dysplasia
Apparent (Functional) Shortening
Apparent shortening is not a true reduction in bone length but rather a perceived shortening due to a postural or positional deformity of the pelvis or joint. The actual measured bone length between fixed bony landmarks (ASIS to medial malleolus) on both sides is equal - but the limb appears shorter because of:
- Adduction contracture of the hip (most common cause - the adducted limb appears shorter)
- Pelvic tilt secondary to scoliosis
- Fixed flexion deformity of the hip
- Abduction contracture (produces apparent lengthening instead)
Key rule: An adduction deformity causes apparent shortening; an abduction deformity causes apparent lengthening.
Method of Examination
Step 1 - Preliminary Positioning
Before any measurement, the patient lies supine with both legs fully extended. The interspinous line (line joining the two ASIS) must be brought to horizontal by abducting or adducting the affected limb together with the normal limb by the same amount. The sound limb must always be placed in the identical position as the affected one.
"If there is adduction deformity of the affected limb, the normal limb must also be adducted to the similar extent before the measurements." - S Das, A Manual on Clinical Surgery
Mark the bony landmarks with a skin pencil before measuring.
Step 2 - Measuring True Length (True Shortening)
- Whole limb: Measure from the ASIS to the tip of the medial malleolus
- Thigh only: Measure from the ASIS to the joint line of the knee (the joint line, not the adductor tubercle or upper border of patella, as both of those are either moveable or hard to find in obese patients)
If the length measured from ASIS to medial malleolus is shorter on the affected side compared with the normal side, true shortening is present.
Step 3 - Measuring Apparent Length (Apparent Shortening)
- Measure from a fixed midline point on the body, usually the umbilicus, to the medial malleolus (or between the medial and lateral malleoli)
If the length from the umbilicus to the medial malleolus is shorter on one side but the ASIS-to-malleolus measurement is equal on both sides, the shortening is apparent (functional) only.
From Rheumatology (Elsevier, 2022): "Measurements from the umbilicus will show an apparent shortening of the leg on the side with the higher pelvis. However, when measured from the anterior superior iliac spine, the legs will have the same length."
Step 4 - Shortening Above the Greater Trochanter
Shortening in the region above the greater trochanter (e.g., in neck of femur fractures, hip dislocations) is assessed by the following special tests:
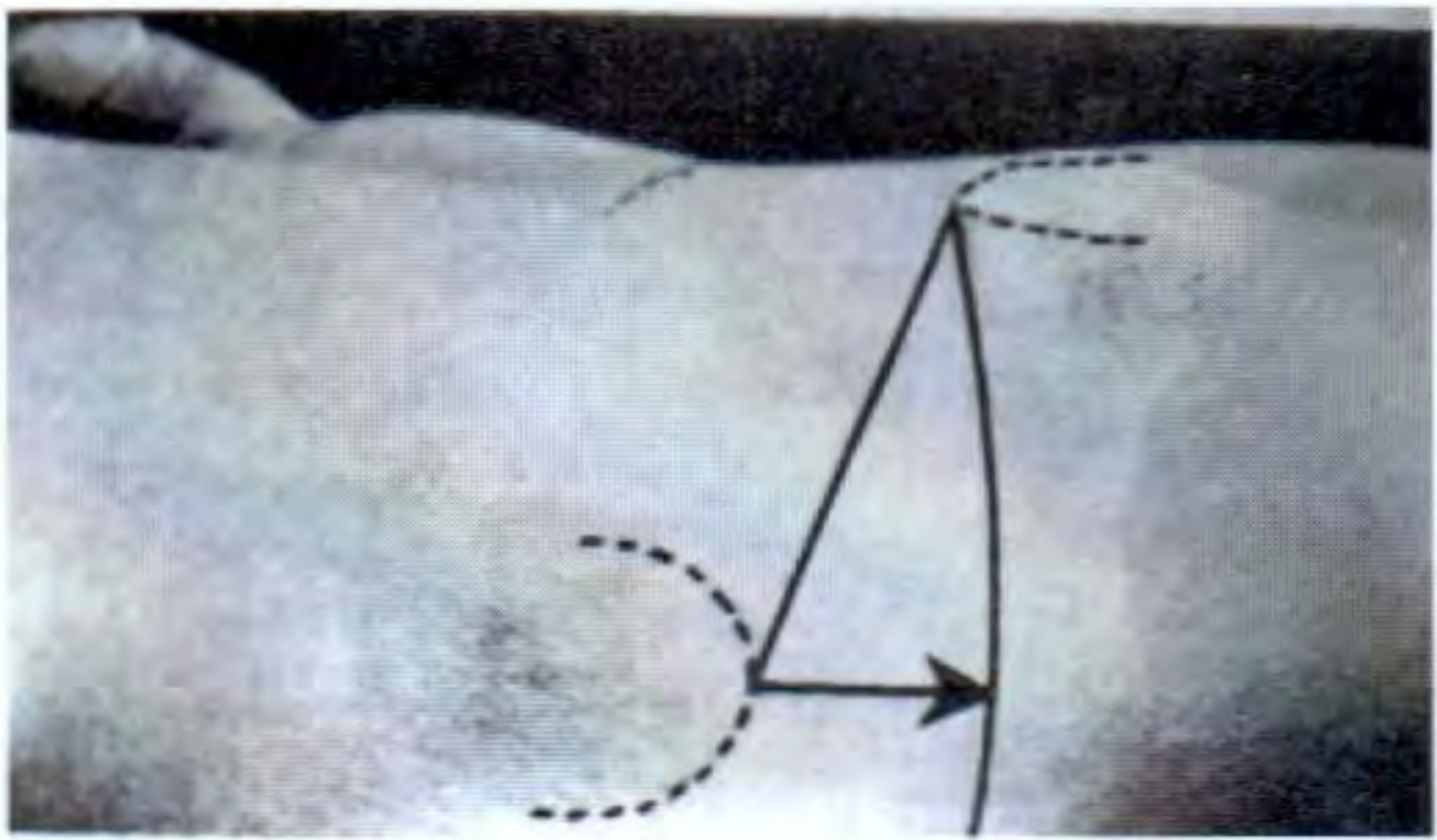
1. Bryant's Triangle
- Patient lies in the dorsal (supine) position
- Three lines are drawn:
- A vertical line drawn downward from the ASIS onto the bed surface
- A line from the tip of the ASIS to the tip of the greater trochanter (the hypotenuse)
- A horizontal line from the tip of the greater trochanter to meet the first vertical line
- The horizontal line is compared with the same line on the normal side
- Diminution in the horizontal line = upward elevation of the greater trochanter (seen in transcervical/subcapital fracture of neck of femur, separation of upper femoral epiphysis)
- Diminution or increase in the hypotenuse line = anterior or posterior displacement of the trochanter (e.g., posterior dislocation of hip)
2. Nelaton's Line (Roser-Nelaton Line)
- Patient lies on the sound (normal) side
- A line (or measuring tape) is placed from the most prominent part of the ischial tuberosity to the tip of the ASIS
- Normally, with the hip in moderate flexion (~45°), this line touches the tip of the greater trochanter
- If the greater trochanter is elevated above this line, it indicates upward displacement (fracture or dislocation)
- The advantage of Nelaton's line: it does not require comparison with the other side, as upward displacement is self-evident
3. Schoemaker's Line
- Draw (or project) a line from the tip of the greater trochanter through the ASIS and extend it anteriorly
- Normally this line meets or crosses the midline at or above the umbilicus
- If the greater trochanter is elevated, the line crosses the midline below the umbilicus
4. Morris' Bitrochanteric Test
- The distance from the outer border of the greater trochanter to the symphysis pubis is measured on both sides using calipers
- Reveals medial displacement (posterior/central dislocation) or lateral displacement (anterior dislocation) of the trochanter
5. Chiene's Test
- Normally, a tape joining the tips of the greater trochanters is parallel to another tape joining the two ASIS
- When a trochanter is raised, these two lines converge towards the affected side
Standing Block Test (for functional/apparent LLD)
Place wooden blocks of known thickness (0.5 cm, 1 cm, 2 cm) under the foot of the apparently shorter limb until the pelvis is level (confirmed when both iliac crests are at the same height on palpation from behind and the anal fissure is vertical).
- If the pelvis can be leveled this way = true leg length discrepancy
- If the pelvis cannot be leveled = functional/apparent discrepancy (due to hip contracture or scoliosis that prevents correction)
Summary Table
| Feature | True Shortening | Apparent Shortening |
|---|---|---|
| Actual bone length | Reduced | Normal |
| ASIS-to-malleolus measurement | Short on affected side | Equal on both sides |
| Umbilicus-to-malleolus measurement | May also be shorter | Shorter (despite equal ASIS-to-malleolus) |
| Cause | Bone loss/fracture/dislocation | Pelvic tilt, adduction contracture |
| Bryant's triangle | Abnormal (horizontal line shortened) | Normal |
| Nelaton's line | Trochanter above the line | Normal |
Clinically important: A limb with adduction contracture (as in tuberculous hip arthritis) will show apparent shortening with a normal ASIS-to-malleolus length - only the umbilicus-based measurement will be asymmetric.
Sources: S Das, A Manual on Clinical Surgery 13th Ed; Rheumatology 2-Volume Set (Elsevier, 2022); Campbell's Operative Orthopaedics 15th Ed 2026; THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
This is a shared conversation. Sign in to Orris to start your own chat.