Fracture disease what's it causes and etiology pathology signs and symptoms and investigations treatment of this explain in detail with appropriate illustrative diagrams and images
fracture disease definition causes pathology signs symptoms treatment orthopedics
https://www.ncbi.nlm.nih.gov/books/NBK559077
https://www.ncbi.nlm.nih.gov/books/NBK559077
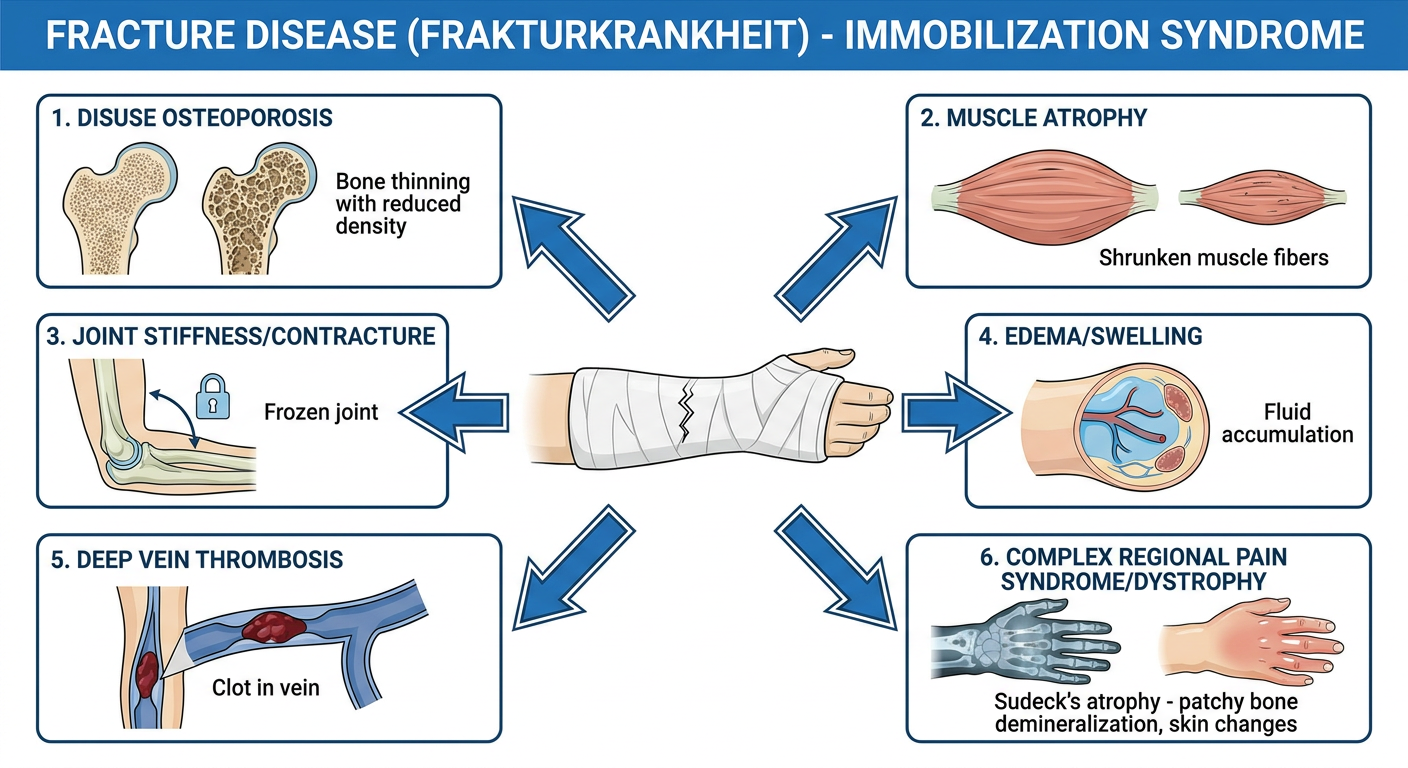
Medical educational diagram titled "Fracture Disease (Frakturkrankheit) - Immobilization Syndrome" showing a central image of a fractured limb in a cast, with arrows pointing outward to labeled boxes showing the six main complications: 1. Disuse Osteoporosis (bone thinning with reduced density), 2. Muscle Atrophy (shrunken muscle fibers), 3. Joint Stiffness/Contracture (frozen joint), 4. Edema/Swelling (fluid accumulation), 5. Deep Vein Thrombosis (clot in vein), 6. Complex Regional Pain Syndrome/Dystrophy (Sudeck's atrophy - patchy bone demineralization, skin changes). Clean, professional medical illustration style with labeled arrows and anatomical detail.
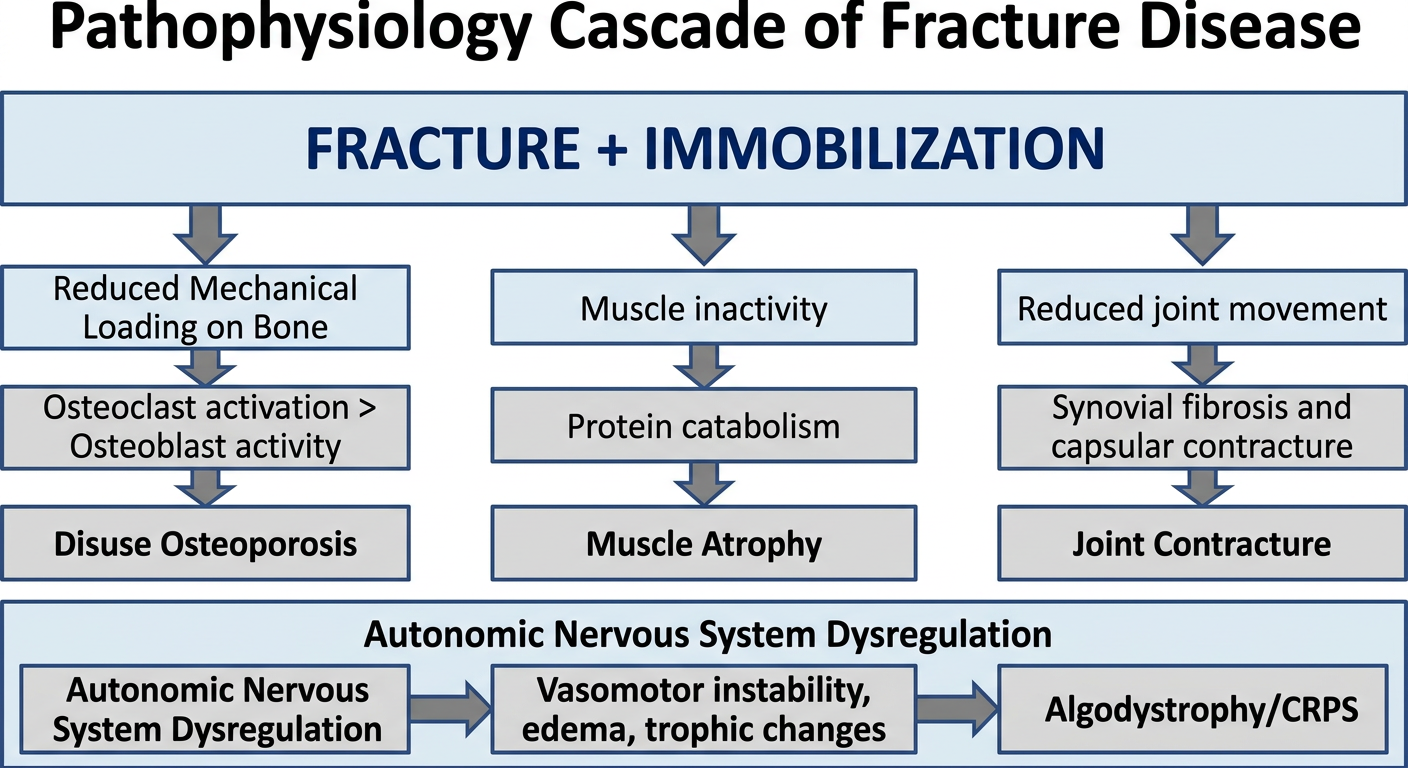
Medical diagram showing the pathophysiology cascade of fracture disease: Starting with "FRACTURE + IMMOBILIZATION" at the top, arrows flowing down to "Reduced Mechanical Loading on Bone" leading to "Osteoclast activation > Osteoblast activity" causing "Disuse Osteoporosis". Parallel pathway shows "Muscle inactivity" leading to "Protein catabolism" causing "Muscle Atrophy". Another branch shows "Reduced joint movement" leading to "Synovial fibrosis and capsular contracture" causing "Joint Contracture". Bottom shows "Autonomic Nervous System Dysregulation" leading to "Vasomotor instability, edema, trophic changes" labeled as "Algodystrophy/CRPS". Clean flowchart style, medical textbook quality.
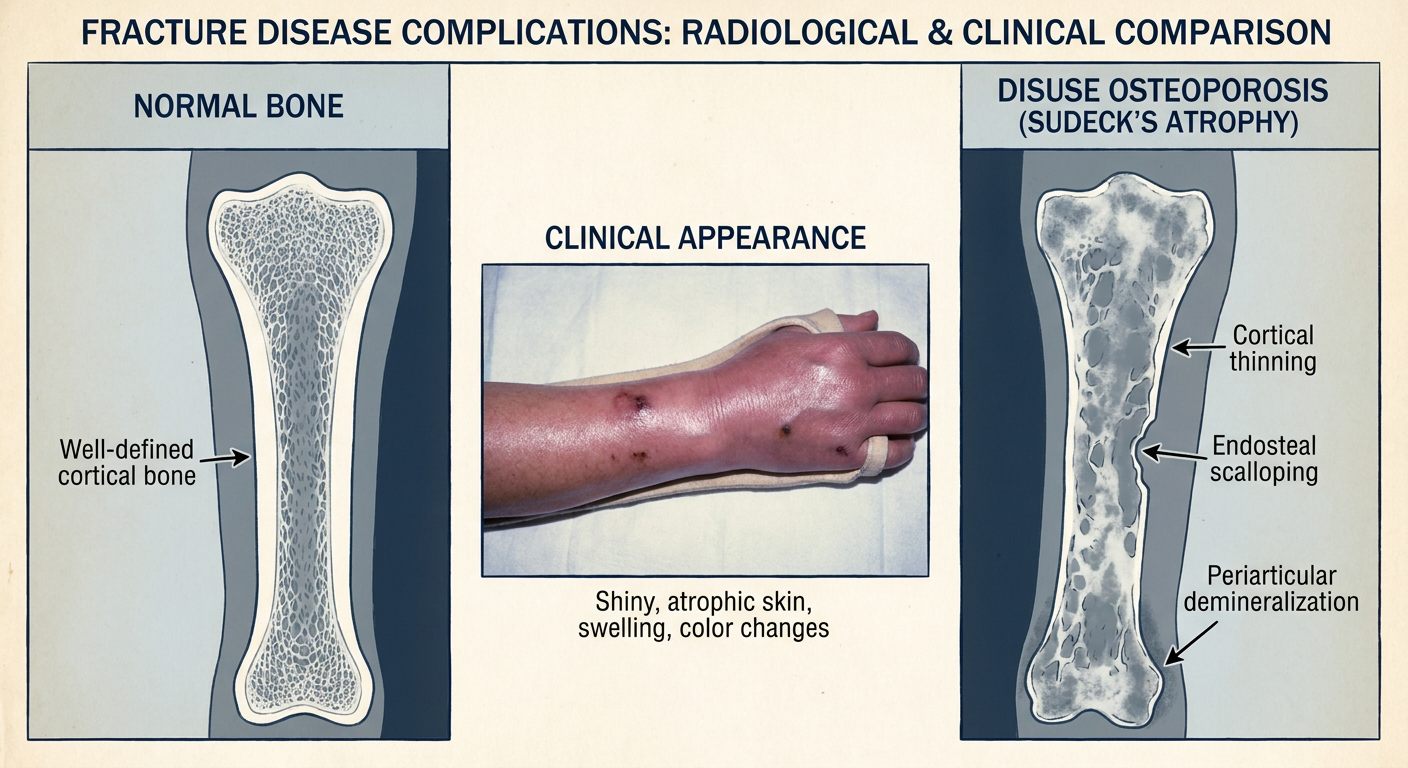
Medical radiology comparison diagram showing X-ray appearance of fracture disease complications: Left panel labeled "Normal Bone" showing dense, well-defined cortical and trabecular bone. Right panel labeled "Disuse Osteoporosis (Sudeck's Atrophy)" showing patchy/mottled demineralization, thinned cortex, sparse trabeculae - characteristic spotty osteoporosis pattern. Center panel showing clinical photo of limb with fracture disease showing shiny, atrophic skin, swelling, and color changes. Labels pointing to key radiological features: cortical thinning, endosteal scalloping, periarticular demineralization. Medical textbook illustration style.
Fracture Disease (Frakturkrankheit) - Complete Guide
Definition
Edema + Muscle Atrophy + Dystrophy (algodystrophy/CRPS)
Illustrative Overview Diagram
1. ETIOLOGY AND CAUSES
Primary Causes
| Cause | Mechanism |
|---|---|
| Fracture treated with cast/plaster | Rigid immobilization prevents all movement |
| Fracture treated conservatively | Prolonged bed rest or splinting |
| Post-surgical immobilization | Rest after internal fixation before mobilization begins |
| Soft-tissue injury with immobilization | Sprains, dislocations kept immobile |
| Neurological injury co-existing with fracture | Paralysis compounds disuse |
Predisposing / Risk Factors
- Age - elderly patients have less physiological reserve
- Pre-existing osteoporosis - already reduced bone density
- Diabetes mellitus - impairs autonomic regulation and healing
- Peripheral vascular disease - reduces trophic supply
- Psychological factors - pain catastrophizing, kinesiophobia (fear of movement)
- Neurological deficit - spinal cord injury, stroke
- Duration of immobilization - longer = worse
From General Anatomy and Musculoskeletal System (THIEME Atlas): "Immediate mobilization prevents thrombosis, emboli, decubitus, and fracture disease, e.g., edema and dystrophy."
2. PATHOLOGY AND PATHOPHYSIOLOGY
A. Disuse Osteoporosis (Bone Pathology)
- Normal bone remodeling depends on Wolff's Law - bone remodels along lines of mechanical stress
- Immobilization removes mechanical loading - osteoclast activity exceeds osteoblast activity
- Rapid bone mineral loss: up to 1-3% per week in immobilized limbs
- Sclerostin (an osteoblast inhibitor) rises, further suppressing bone formation
- Thinned cortex with endosteal scalloping
- Reduced trabecular density and spacing
- Periarticular (juxta-articular) demineralization is the hallmark
- Pattern is "spotty/patchy" - distinguishes it from systemic osteoporosis
B. Muscle Atrophy
- Loss of nerve stimulation and mechanical loading leads to protein catabolism
- Type II (fast-twitch) muscle fibers atrophy fastest
- Histology: reduced fiber diameter, increased connective tissue infiltration
- Rate: ~3% muscle mass lost per day in complete immobilization
C. Joint Contracture / Stiffness
- Reduced synovial fluid circulation leads to synovial fibrosis
- Joint capsule and periarticular structures undergo fibrous contracture
- Intra-articular adhesions form
- Cartilage softening (chondromalacia) from reduced compression loading
D. Edema
- Reduced muscle pump action impairs venous and lymphatic return
- Capillary stasis and increased hydrostatic pressure in the limb
- Protein-rich interstitial edema accumulates in soft tissues
E. Deep Vein Thrombosis (DVT)
- Virchow's Triad in fracture disease:
- Stasis - immobilization reduces venous flow
- Hypercoagulability - injury-related coagulation activation
- Endothelial injury - direct trauma to vessel walls
- Proximal DVT (femoral, popliteal) can lead to pulmonary embolism
F. Complex Regional Pain Syndrome (CRPS) / Algodystrophy / Sudeck's Atrophy
- Reflex Sympathetic Dystrophy (RSD)
- Sudeck's Atrophy
- Algodystrophy / Algoneurodystrophy
- Post-traumatic painful osteoporosis
- Shoulder-hand syndrome (when upper limb affected)
- Poorly understood - involves dysregulation of the autonomic nervous system
- Central and peripheral sensitization of pain pathways
- Sympathetic nervous system activation causes vasomotor instability
- Neurogenic inflammation (substance P, bradykinin, neuropeptides)
- Disuse and kinesiophobia (fear of movement) perpetuate and worsen the syndrome
- Inflammatory mediators cause trophic skin and bone changes
From Rockwood and Green's Fractures in Adults (10th ed., 2025): "CRPS refers to an unexplained pain syndrome...characterized by disproportionate pain and accompanying autonomic and motor disturbances...Nowadays it is considered a rare, devastating complication of minor injury caused by disuse and seen in any patient at every age."
3. SIGNS AND SYMPTOMS
Local Signs and Symptoms
| Category | Symptoms (Reported) | Signs (Observed on Exam) |
|---|---|---|
| Pain | Burning, disproportionate pain; allodynia; hyperesthesia | Hyperalgesia to pinprick; allodynia to light touch |
| Vasomotor | Skin color changes; temperature difference between limbs | Temperature asymmetry >1°C; skin color/asymmetry |
| Edema/Sudomotor | Swelling; increased/decreased sweating | Pitting or non-pitting edema; sweating asymmetry |
| Motor/Trophic | Weakness; reduced range of motion; tremor | Muscle wasting; joint stiffness; dystonia; trophic changes (nails, hair, skin) |
Stages of CRPS/Algodystrophy (Classic Three-Stage Model)
- Burning pain, hyperalgesia
- Warm, red, edematous limb
- Increased sweating
- Rapid hair and nail growth (paradoxically)
- X-ray: patchy periarticular osteoporosis beginning
- Persistent pain, allodynia
- Skin becomes cool, pale/cyanotic, shiny
- Edema becomes hard/brawny
- Joint stiffness increases
- X-ray: diffuse osteoporosis more evident
- Pain may diminish but disability is severe
- Skin atrophic, glossy, cold
- Irreversible muscle atrophy and joint contracture
- Subcutaneous tissue atrophied
- X-ray: severe diffuse osteoporosis
General Signs of Fracture Disease
- Muscle wasting visible and measurable (limb circumference)
- Pressure sores (decubitus ulcers) in bed-bound patients
- Deep vein thrombosis signs (leg swelling, Homan's sign - not specific)
- Pulmonary embolism (dyspnea, pleuritic chest pain, hemoptysis)
4. INVESTIGATIONS
Radiological Investigations
- Periarticular osteoporosis - "spotty" or "moth-eaten" pattern
- Thinning of cortex
- Reduced trabecular density
- Soft tissue swelling
- Late: severe diffuse osteoporosis
- Stage 1: Increased uptake (hot scan) - hypervascular, increased bone turnover
- Stage 3: Decreased uptake (cold scan) - atrophic, reduced perfusion
- Helpful for staging and distinguishing from other conditions
- Early bone marrow edema
- Periarticular changes
- Rules out other pathology (osteomyelitis, tumor)
- Soft tissue evaluation
- Better assessment of bone mineral density changes
- Identifies subtle cortical thinning
- Useful for planning surgical intervention
- Quantifies bone mineral density loss
- Monitors response to treatment
Laboratory Investigations
| Test | Relevance |
|---|---|
| Full blood count (FBC) | Baseline; infection screen |
| ESR/CRP | Elevated in inflammatory phase of CRPS |
| Serum calcium, phosphate, ALP | Bone metabolism markers |
| Serum D-dimer | Screening for DVT/PE |
| Urine calcium | Increased in disuse osteoporosis (hypercalciuria) |
| Urinalysis | Kidney stones (from hypercalciuria) |
Specialized Tests
- Doppler ultrasound of lower limb veins (gold standard for DVT)
- CT pulmonary angiography (if PE suspected)
- V/Q scan
- Thermography (temperature asymmetry >1°C is significant)
- Quantitative sudomotor axon reflex testing (QSART) - sweat abnormalities
- Three-phase bone scan
- Budapest Criteria assessment (clinical diagnosis - see below)
Budapest Diagnostic Criteria for CRPS (Budapest, 2003)
- Have continuing pain disproportionate to the inciting event
- Report at least 1 symptom in 3 of 4 categories:
- Sensory (hyperesthesia/allodynia)
- Vasomotor (temperature/color asymmetry)
- Sudomotor/Edema (sweating changes, edema)
- Motor/Trophic (decreased ROM, weakness, trophic changes)
- Show at least 1 sign at examination in 2 or more categories (same categories)
- No other diagnosis better explains the signs and symptoms
5. TREATMENT
A. PREVENTION (Most Important)
The best treatment is prevention through early mobilization after fracture stabilization.
- Rigid internal fixation (plates, screws, intramedullary nails, tension-band wiring) allows immediate mobilization
- Advantages over cast: exact repositioning, early movement, prevents muscle atrophy, disuse osteoporosis, DVT, and dystrophy
- External fixation for complex/open fractures - still allows partial loading
- Early weight-bearing as soon as fracture stability allows
- Active movement therapy - mobilization of joints proximal and distal to fracture
- Elevation of the limb to reduce edema
- Compression stockings/bandaging to prevent edema and DVT
B. TREATMENT OF SPECIFIC COMPONENTS
1. Disuse Osteoporosis
- Weight-bearing exercise / physical therapy
- Calcium supplementation (1000-1500 mg/day) + Vitamin D (800-1000 IU/day)
- Bisphosphonates (alendronate, zoledronic acid) if severe
- Avoid tobacco, alcohol
- Monitor with DEXA scans
2. Muscle Atrophy
- Progressive resistance exercises
- Physiotherapy - electrical muscle stimulation (EMS) for paralyzed limbs
- Protein-rich diet (1.2-1.5 g/kg/day)
- Occupational therapy for functional retraining
3. Joint Contracture
- Passive and active range-of-motion exercises
- Serial splinting / dynamic splinting
- Manipulation under anesthesia (MUA) for established contractures
- Surgical release (arthrolysis, capsulotomy) in severe cases
4. Edema Management
- Elevation of the affected limb
- Compression bandaging / stockings
- Lymphedema massage (manual lymphatic drainage)
- Diuretics - short-term use if severe
5. DVT Prevention and Treatment
- Low molecular weight heparin (LMWH) - e.g., enoxaparin - for prophylaxis
- Mechanical prophylaxis - intermittent pneumatic compression, anti-embolism stockings
- Early mobilization
- Established DVT: therapeutic anticoagulation (LMWH/DOAC for 3-6 months)
- Established PE: anticoagulation ± thrombolysis in severe cases
6. CRPS / Algodystrophy Treatment
| Modality | Details |
|---|---|
| Physical Therapy | Graded exposure, pain exposure physical therapy (PEPT), desensitization; KEY treatment |
| Analgesics | NSAIDs, paracetamol for mild; tramadol/opioids for severe |
| Neuropathic agents | Gabapentin, pregabalin for neuropathic pain |
| Corticosteroids | Short course in acute phase (prednisolone) |
| Bisphosphonates | Pamidronate, alendronate - reduce bone pain and osteoporosis |
| Calcitonin | Analgesic + antiresorptive effect (intranasal or injection) |
| Sympathetic nerve block | Stellate ganglion / lumbar sympathetic block - provides temporary relief |
| Spinal cord stimulation | For chronic refractory CRPS - reduces pain via dorsal column modulation |
| Psychological therapy | CBT, exposure in vivo, graded motor imagery - addresses kinesiophobia |
| TENS | Transcutaneous electrical nerve stimulation for pain relief |
| Mannitol IV | Free radical scavenger - used in acute severe CRPS |
| Vitamin C | 500 mg/day post-fracture shown to reduce CRPS incidence (particularly wrist fractures) |
| Amputation | Last resort in severe intractable cases with severe tissue destruction |
From Rockwood and Green's Fractures in Adults: "After the introduction of several more cognitive and behavioral treatment methods, such as pain exposure physical therapy (PEPT) and exposure in vivo, it appeared that disuse and kinesiophobia played an important role in the development and maintenance of CRPS."
6. PROGNOSIS
| Outcome Factor | Better Prognosis | Worse Prognosis |
|---|---|---|
| Duration of immobilization | Short | Long (>6 weeks) |
| Age | Young | Elderly |
| Stage of CRPS at diagnosis | Stage 1 (acute) | Stage 3 (atrophic) |
| Treatment approach | Early, multidisciplinary | Delayed, unimodal |
| Patient compliance | Good | Poor (kinesiophobia) |
| Co-morbidities | None | Diabetes, vascular disease |
- Most patients with early-stage fracture disease recover fully with appropriate physiotherapy and mobilization.
- Established CRPS (Stage 3) has a poor prognosis and can result in permanent disability.
- Suicide attempts and severe depression have been documented in long-standing CRPS cases.
Summary Concept Map
FRACTURE + PROLONGED IMMOBILIZATION
|
┌──────┴──────────────────────────────┐
| |
LOCAL EFFECTS SYSTEMIC EFFECTS
| |
┌──┴────────────────────┐ DVT / PE
| | |
Disuse Muscle Joint
Osteo- Atrophy Stiffness
porosis /Contracture
|
Sudeck's Atrophy
(CRPS - Algodystrophy)
|
├─ Pain (burning, disproportionate)
├─ Vasomotor changes (color, temperature)
├─ Edema + Sweating abnormalities
└─ Motor/Trophic changes
TREATMENT:
Prevention > Early mobilization after osteosynthesis
Rehabilitation > Physiotherapy, PEPT, graded exposure
Pharmacology > Bisphosphonates, Ca/Vit D, neuropathics
Intervention > Sympathetic blocks, SCS, surgery
- General Anatomy and Musculoskeletal System - THIEME Atlas of Anatomy, Schuenke et al.
- Rockwood and Green's Fractures in Adults, 10th Edition (2025), Chapter 27: CRPS
- Pathologic Fractures - StatPearls, Rizzo & Kenan (2023), NCBI Bookshelf NBK559077