may i have complete treatment guideline for chronic diarrea and weakness as GP
Reading File
Finding Sources
Finding Sources
Searching PubMed
"chronic diarrhea"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
I now have comprehensive data from the most authoritative textbooks. Let me compile a complete GP-focused treatment guideline.
Complete GP Treatment Guideline: Chronic Diarrhea with Weakness
Based on Harrison's Principles of Internal Medicine 22E (2025), Sleisenger & Fordtran's GI & Liver Disease, and The Washington Manual of Medical Therapeutics
1. DEFINITION & RED FLAGS
Chronic diarrhea = diarrhea lasting >4 weeks (loose/watery stools >3/day or >200 g/day).
🚨 Alarm Features — Refer/Investigate Urgently
| Feature | Concern |
|---|---|
| Blood per rectum | Colorectal cancer, IBD, ischemia |
| Weight loss >5 kg | Malignancy, malabsorption, IBD |
| Nocturnal diarrhea (wakes patient) | Organic disease (not functional) |
| Age >50, new onset | Colorectal cancer |
| Fever | Infection, IBD |
| Progressive weakness + edema | Protein-losing enteropathy, malabsorption |
| Family history of IBD/celiac | IBD, celiac disease |
| Palpable abdominal mass | Malignancy |
2. DIAGNOSTIC FRAMEWORK (Management Algorithm)
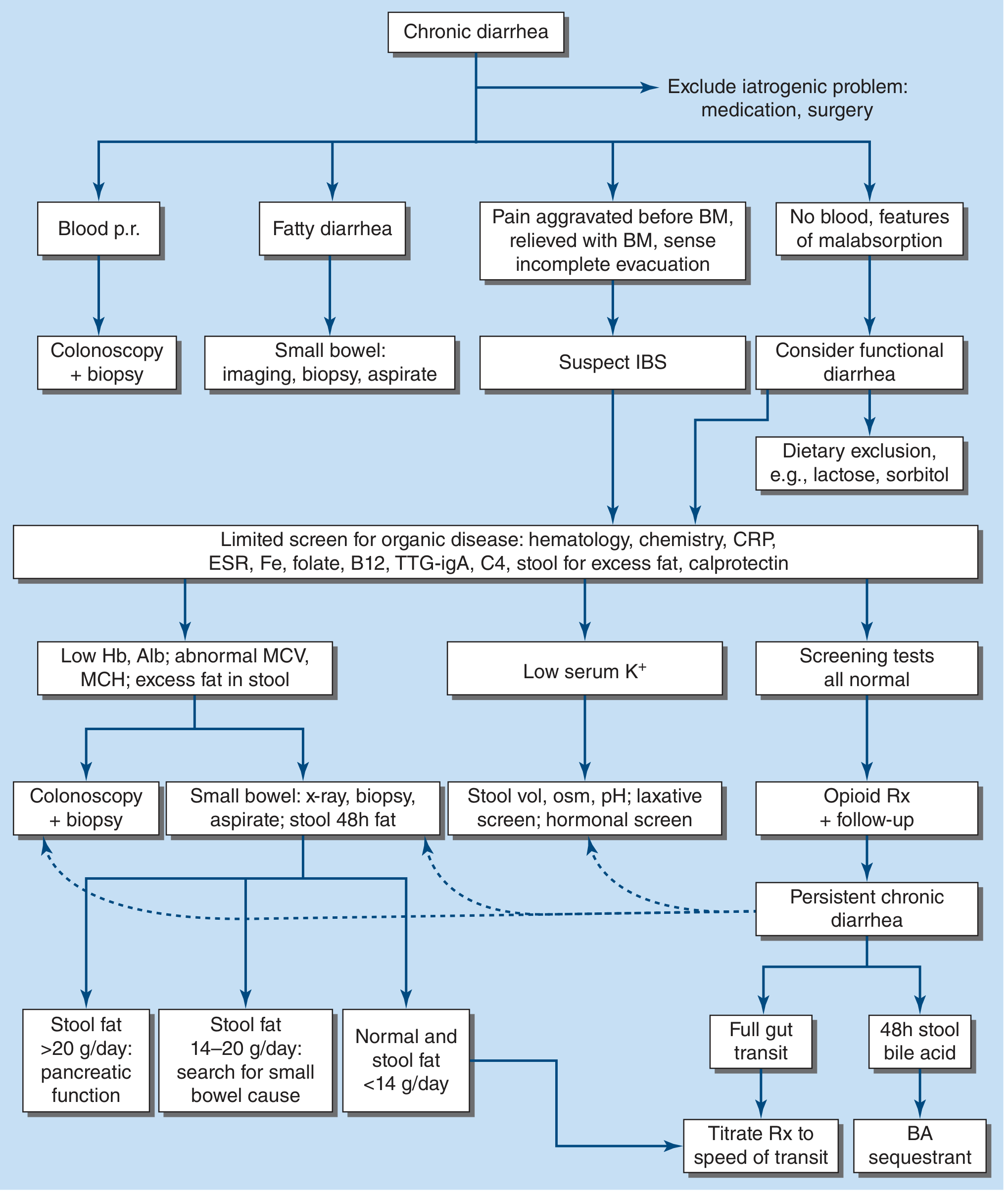
Step 1 — Classify by Symptom Pattern
| Pattern | Consider |
|---|---|
| Blood PR | Colonoscopy + biopsy |
| Fatty/greasy stools, weight loss, steatorrhea | Malabsorption workup (small bowel imaging, biopsy, aspirate) |
| Pain before BM, relieved by BM, bloating | IBS with diarrhea |
| Watery, no blood, no fat | Secretory or functional |
| Weakness, edema, anemia | Malabsorption/protein-losing/IBD |
Step 2 — First-Line Investigations (GP Level)
Blood Tests:
- CBC (anemia → blood loss or nutritional deficiency; eosinophilia → parasites)
- CMP (electrolytes — hypokalemia in secretory diarrhea; albumin — protein loss)
- CRP/ESR (inflammation screen)
- IgA tissue transglutaminase (TTG-IgA) + total IgA → celiac disease
- Thyroid function (hyperthyroidism can cause diarrhea + weakness)
- Iron, folate, B12, vitamin D (malabsorption markers)
- Blood glucose (diabetic diarrhea/autonomic neuropathy)
Stool Tests:
- Fecal occult blood
- Fecal calprotectin or lactoferrin (sensitivity ~92%/specificity ~82% for inflammatory diarrhea)
- Stool culture, ova & parasites, Giardia and Cryptosporidium antigen (or multiplex PCR)
- Stool fat (Sudan stain — sensitivity 76–94% for steatorrhea)
3. CAUSES BY MECHANISM (Major Categories)
Secretory Diarrhea
Watery, large-volume, painless, persists with fasting; no osmotic gap
- Stimulant laxatives, chronic ethanol, drugs (olmesartan, metformin, SSRIs, colchicine)
- Hormone-producing tumors (VIPoma, carcinoid, gastrinoma, medullary thyroid cancer)
- Addison's disease, bile acid diarrhea, congenital electrolyte defects
Osmotic Diarrhea
Stops with fasting; osmotic gap present
- Lactase deficiency, sorbitol/fructose/FODMAPs, osmotic laxatives (Mg²⁺, PO₄³⁻)
Steatorrheal / Malabsorptive Diarrhea (major cause of weakness)
Fatty, foul-smelling, floating stools; weight loss, weakness, nutritional deficiencies
- Celiac disease (most common in adults — screen all!)
- Pancreatic exocrine insufficiency (stool fat >20 g/day → pancreatic function test)
- Bacterial overgrowth (SIBO), Whipple's disease, Crohn's disease
- Stool fat 14–20 g/day → search for small bowel cause
- Stool fat >20 g/day → assess pancreatic function
Inflammatory Diarrhea (IBD)
Bloody/mucousy, fever, cramps, elevated calprotectin/CRP
- Crohn's disease, ulcerative colitis, microscopic colitis (lymphocytic/collagenous)
- Infectious: Giardia, Entamoeba, C. difficile, tuberculosis
Functional / IBS-D
Meets Rome IV criteria; no alarm features; normal investigations
- Pain aggravated before BM, relieved by BM, urgency, bloating
- Diagnosis of exclusion
4. TREATMENT BY CAUSE
A. Specific / Curative Treatments
| Condition | Treatment |
|---|---|
| Celiac disease | Strict gluten-free diet (lifelong) |
| Lactase deficiency | Lactose-free diet; lactase enzyme supplements |
| Giardiasis | Tinidazole 2 g PO single dose OR metronidazole 500 mg q8h × 7 days OR nitazoxanide 500 mg q12h × 3 days |
| Amebiasis | Metronidazole 500 mg q8h × 7–10 days → then iodoquinol or paromomycin (cyst eradication) |
| SIBO | Rifaximin 550 mg TID × 14 days (non-absorbed antibiotic) |
| C. difficile | Vancomycin PO 125 mg QID × 10–14 days (preferred) OR fidaxomicin |
| IBD (UC/Crohn's) | 5-ASA (mesalamine), corticosteroids for flares; refer to gastroenterology |
| Microscopic colitis | Budesonide 9 mg/day × 8 weeks; stop offending drugs (NSAIDs, SSRIs, PPIs) |
| Pancreatic insufficiency | Pancreatic enzyme replacement therapy (PERT) with meals |
| Bile acid malabsorption | Cholestyramine 4 g 1–3×/day; colesevelam |
| Whipple's disease | Ceftriaxone IV × 2 weeks → TMP-SMX × 1–2 years |
| Drug-induced | Discontinue offending drug (metformin, olmesartan, colchicine, laxatives) |
| Hyperthyroidism | Treat thyroid disease (methimazole, propylthiouracil) |
| Carcinoid/VIPoma | Octreotide (somatostatin analogue); refer to oncology |
| Gastrinoma | PPI (high dose); refer for surgical evaluation |
| Addison's disease | Hydrocortisone + fludrocortisone replacement |
| Colorectal cancer | Surgical referral |
B. Symptomatic / Empirical Treatments (When Cause Not Identified or as Adjunct)
Antidiarrheal / Antimotility Agents
| Drug | Dose | Notes |
|---|---|---|
| Loperamide | 2–4 mg after each loose stool; max 16 mg/day | First-line; OTC; no CNS effects |
| Diphenoxylate/atropine | 5 mg PO QID → taper | Mild-moderate diarrhea |
| Codeine | 15–60 mg PO q4–6h | For severe diarrhea refractory to loperamide |
| Cholestyramine | 4 g PO 1–4×/day | Bile acid diarrhea; also empirical trial |
| Octreotide | 50–200 µg SC TID | Secretory diarrhea, carcinoid, VIPoma, dumping syndrome |
| Clonidine | 0.1–0.3 mg PO BID | Diabetic autonomic diarrhea (monitor BP — hypotension risk) |
| Alosetron / Ondansetron | Alosetron 0.5 mg BID; Ondansetron 4 mg TID | 5-HT3 antagonists for IBS-D |
| Eluxadoline | 100 mg PO BID with food | IBS-D; avoid if no gallbladder (pancreatitis risk) |
| Rifaximin | 550 mg TID × 14 days | IBS-D, SIBO |
Stool-Modifying / Adjunctive
- Psyllium (bulk-forming): improves stool consistency; useful with fecal incontinence
- Calcium 1–2 g/day: may reduce stool frequency via unknown mechanism
- Pectin: delays proximal transit; adjunctive
- Probiotics: modest evidence; may help antibiotic-associated and travelers' diarrhea
5. MANAGEMENT OF WEAKNESS (Complication of Chronic Diarrhea)
Weakness accompanying chronic diarrhea usually reflects one or more of:
A. Fluid & Electrolyte Depletion
- Oral rehydration solution (ORS) — central to management; isotonic solutions preferred
- For sport drinks: adequate for mild cases; WHO-ORS or Pedialyte preferred for moderate
- Potassium replacement: low K⁺ is a hallmark of chronic secretory diarrhea → oral KCl supplements; dietary potassium (bananas, potatoes)
- IV fluids (Ringer's lactate or NS) if oral intake inadequate or severe dehydration
B. Nutritional Deficiencies (Malabsorption)
| Deficiency | Clinical Features | Replacement |
|---|---|---|
| Iron | Microcytic anemia, fatigue | Ferrous sulfate 325 mg TID; IV iron if severe |
| Folate | Macrocytic anemia, fatigue, neuropathy | Folic acid 5 mg/day × 4 months |
| Vitamin B12 | Macrocytic anemia, neurological symptoms | IM hydroxocobalamin 1 mg × 6 doses, then monthly |
| Vitamin D | Bone pain, muscle weakness, fatigue | Cholecalciferol 1000–4000 IU/day |
| Vitamin A, E, K | Night blindness, neuropathy, bleeding | Fat-soluble vitamin supplementation |
| Zinc | Dermatitis, immune dysfunction, weakness | Zinc sulfate 220 mg/day |
| Magnesium | Muscle cramps, weakness | Oral magnesium glycinate (IV if severe) |
| Protein/Albumin | Edema, muscle wasting | High-protein diet; nutritional support |
C. Underlying Disease Causing Weakness
- Celiac disease → GFD corrects all deficiencies
- IBD → treat inflammation; nutritional support
- Adrenal insufficiency → hydrocortisone dramatically reverses weakness
- Hyperthyroidism → antithyroid treatment restores weight and strength
- Malignancy → oncology referral
6. WHEN TO REFER (Red Line for GP)
Refer to Gastroenterology if:
- Any alarm feature present
- Diagnosis unclear after initial workup
- Positive fecal calprotectin (>200 µg/g) → IBD workup
- Suspected malabsorption (steatorrhea, weight loss, hypoalbuminemia)
- Persistent diarrhea >4–6 weeks despite empirical treatment
- Colonoscopy/small bowel imaging indicated
Refer to Endocrinology: suspected Addison's, VIPoma, carcinoid, gastrinoma, hyperthyroidism
7. GP APPROACH — PRACTICAL FLOWCHART
CHRONIC DIARRHEA (>4 weeks) + WEAKNESS
│
▼
STEP 1: Alarm features? ──YES──► Urgent colonoscopy / refer GI
│ NO
▼
STEP 2: Drug review → Stop offending drugs
│
▼
STEP 3: Exclude infection → Stool cultures, O&P, Giardia Ag, PCR
│
▼
STEP 4: Blood screen → CBC, CMP, CRP, TTG-IgA, TFTs, B12/folate/Fe, Vit D
Stool screen → Calprotectin, stool fat, FOBT
│
▼
STEP 5: Pattern-based diagnosis:
- IBS-D criteria met, normal bloods → Dietary trial (low-FODMAP), loperamide, rifaximin
- Celiac suspected → GFD + refer GI
- Malabsorption signs → Small bowel workup + nutritional replacement
- Inflammatory signs (high calprotectin/CRP) → Colonoscopy + biopsy
- Infectious → Targeted antibiotic therapy
│
▼
STEP 6: Correct Weakness
- ORS / electrolyte replacement
- Treat nutritional deficiencies (Fe, B12, folate, Vit D, Mg, Zn)
- High-protein, low-irritant diet
│
▼
STEP 7: Empirical antidiarrheal if no diagnosis
- Loperamide first-line
- Cholestyramine trial (bile acid diarrhea)
- Rifaximin trial (SIBO/IBS)
- Refer if no response in 4–6 weeks
8. DIETARY ADVICE FOR PATIENTS
- Avoid lactose (dairy) initially as a trial — if improvement, confirm lactase deficiency
- Trial low-FODMAP diet for IBS-D
- Avoid sorbitol (sugar-free gum, candies), fructose (excess fruit juice), alcohol, caffeine
- Gluten-free trial only after celiac serology — do NOT start before blood test
- Small, frequent meals; avoid high-fat meals if steatorrhea suspected
- Maintain adequate fluid intake (minimum 2 L/day); use ORS if significant ongoing losses
9. MONITORING
- Review in 2–4 weeks after initial treatment
- Repeat CBC, electrolytes, albumin at 6–8 weeks if malabsorption or significant weakness
- Track weight, stool frequency (Bristol Stool Scale), and energy levels
- If persistent: escalate investigations (colonoscopy, CT enterography, hydrogen breath test)
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 351–355 | Sleisenger & Fordtran's GI & Liver Disease, p. 233–239 | The Washington Manual of Medical Therapeutics
May i have complete treatment guideline for all skin disease at GP level
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
atopic dermatitis eczema treatment skin rash
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.