Amuptation management based on othropeidcs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from Campbell's Operative Orthopaedics 15th Ed (2026), Rockwood & Green's Fractures, and Bradley & Daroff's Neurology. Let me compile the full structured answer.
Amputation Management in Orthopaedics
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Rockwood & Green's Fractures in Adults 10th Ed 2025; Bradley & Daroff's Neurology in Clinical Practice
1. Definition and Perspective
Amputation should not be viewed as a failure of treatment. It is a reconstructive procedure - "the function of a limb with a properly fitted prosthesis after amputation often is better than a painful extremity with limited usefulness." Amputation is typically the most reliable surgery for failed reconstruction. - Campbell's Operative Orthopaedics, p. 3751
2. Indications for Amputation
Absolute / Reconstruction-failed:
- Reconstruction has initially failed or failed multiple times
- A proposed plan of reconstruction would likely result in less satisfactory function than amputation + prosthesis
- The danger of major operations outweighs anticipated benefit
- The damaged part (e.g. a finger) cannot be restored enough to avoid interfering with overall extremity function
- Reconstruction is impossible
Specific orthopaedic indications:
- Malignant transformation of chronic osteomyelitis
- Multiple failed surgical debridements or reconstructive procedures
- Uncontrolled, debilitating pain (at patient's request)
- Uncontrollable infection (e.g. Charcot arthropathy with severe infection)
- Tuberculous osteomyelitis causing marked limb shortening in children
- Extensive amyloid disease with extensive lower extremity involvement
Risk factors predicting reconstruction failure (favouring early amputation):
- Severe / unaddressed peripheral vascular disease
- Diabetes mellitus
- Malnutrition
- Smoking
- Type of pathogen isolated
Early amputation literature increasingly supports it in cases with expected poor outcomes - compared to limb reconstruction, early amputation can lead to faster recovery and equivalent or superior functional outcomes. - Rockwood & Green, p. 976
3. Levels of Amputation
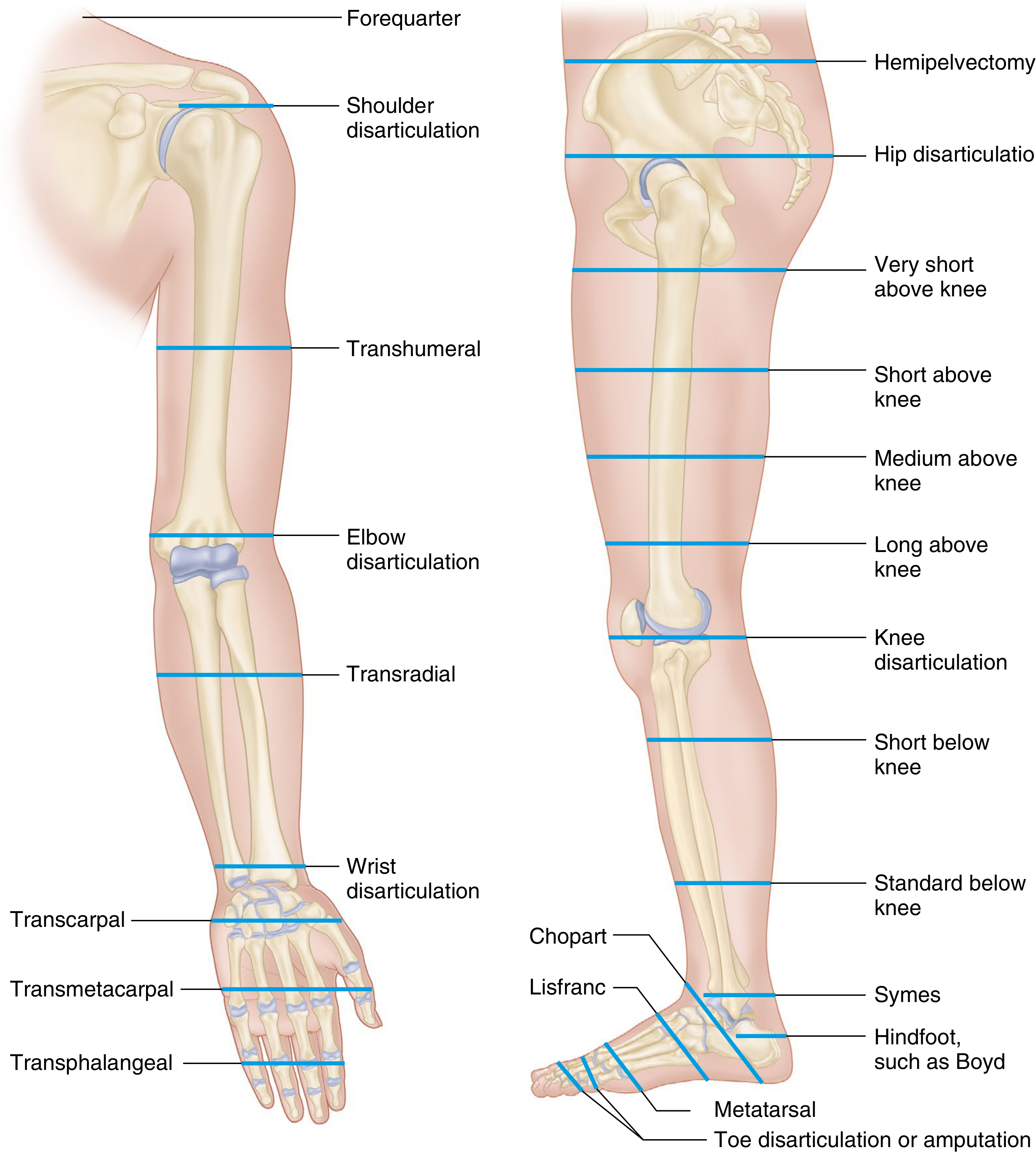
FIGURE 16.5 - Levels of amputation: more distal levels = increased function; more proximal levels = decreased complication rate. - Campbell's, p. 839
Lower Extremity (distal to proximal)
| Level | Notes |
|---|---|
| Toe disarticulation / amputation | Most distal |
| Transmetatarsal | |
| Lisfranc | Tarsometatarsal joint |
| Chopart | Talonavicular-calcaneocuboid |
| Syme (hindfoot / Boyd) | Ankle disarticulation; allows ambulation without complex prosthesis |
| Standard below-knee (transtibial) | Best chance of walking with prosthesis; preserves knee |
| Short below-knee | |
| Knee disarticulation | Best for non-ambulatory patients; longer lever arm, stable sitting |
| Transfemoral (above-knee) | Short / medium / long variants |
| Hip disarticulation | |
| Hemipelvectomy | Most proximal lower extremity level |
Upper Extremity (distal to proximal)
- Transphalangeal → Transmetacarpal → Transcarpal → Wrist disarticulation → Transradial (forearm) → Elbow disarticulation → Transhumeral → Shoulder disarticulation → Forequarter amputation
Key Energy Cost Data
Walking energy cost increases with level of amputation:
- Self-selected walking velocity in vascular amputees: 66% (Syme), 59% (transtibial), 44% (transfemoral) vs. controls
- In traumatic amputees (younger): 87% (transtibial), 63% (transfemoral) vs. controls
- Vascular transfemoral amputees often exceed 50% of maximal aerobic capacity even for minimal ambulation → anaerobic mechanisms engaged → decreased endurance - Campbell's, p. 839
4. Preoperative Assessment
Determining Amputation Level
- Vascular surgery consultation should be obtained - revascularisation may allow preservation of partial foot/ankle even if not full-limb salvage
- Screen for nutritional status and immunocompetence (malnourished / immunocompromised patients have markedly increased perioperative complications)
- Discourage tobacco use
Assessment of Skin Flap Perfusion / Healing Potential
- Clinical assessment: skin colour, hair growth, skin temperature (initial screening)
- Arteriograms: little help for wound healing prediction
- Segmental systolic pressures: often falsely elevated due to arteriosclerotic noncompliant vessels
- Skin perfusion pressures: some benefit
- Thermography / laser Doppler flowmetry: described but less preferred
- Transcutaneous oxygen measurement (TcPO2) - most beneficial:
- Probe heated to 45°C for 10 minutes before measurement
- Cutoff range studied: 20-40 mmHg for "good" healing potential
- Increase of ≥10 mmHg after 100% O₂ inhalation = good healing indicator
- Decrease >15 mmHg after 3 minutes of elevation = poor prognostic sign
- Must be interpreted alongside age, comorbidities, ambulatory potential - Campbell's, p. 839
5. Surgical Principles
Skin and Muscle Flaps
- Best flap type is defined for each level; atypical flaps may be necessary
- Scar location is rarely important with modern total-contact prosthetic socks as long as it is not adherent to bone (adherent scar breaks down with prosthetic use)
- Redundant soft tissue creates prosthetic fitting problems
- Muscles divided at least 5 cm distal to intended bone resection
- Myodesis (suturing muscle/tendon to bone) vs. Myoplasty (suturing to periosteum/fascia):
- Myodesis is preferred: supplies stronger insertion, maximises strength, minimises muscle atrophy
- Transected muscle atrophies 40-60% over 2 years if not securely fixed
- Myodesed muscles counterbalance antagonists, preventing contractures
- Myodesis may be contraindicated in severe ischaemia due to increased wound breakdown risk - Campbell's, p. 840
Open Amputations
- Skin not closed over stump end
- Indicated in: infections and severe traumatic wounds with extensive tissue destruction and gross contamination
- Must be followed by secondary closure, reamputation, revision, or plastic repair
- Modern approach: Vacuum-Assisted Closure (VAC) applied to open stump
- Debridements at 48-hour intervals; VAC reapplied after each until wound ready for closure
- Provides improved blood flow, accelerated granulation tissue, decreased edema, enhanced lymphatic drainage - Campbell's, p. 841
Key Surgical Goals (Rockwood & Green)
- Stump accommodated easily with orthotic/prosthetic device
- Stump is durable and resistant to pressure breakdown
- Muscle imbalances are avoided
- Wound healing by primary intention where possible
- Preserve maximum limb length and sensibility
6. Postoperative Management
Multidisciplinary Team
Postoperative care requires a multidisciplinary team: surgeon, physical medicine specialist, physical therapist, certified prosthetist, nurses.
Dressings and Stump Care
- Rigid plaster cast applied to stump after surgery (if no immediate weight-bearing planned)
- Pad all bony prominences; avoid proximal constriction; ensure dependable suspension
- If immediate weight-bearing planned: true prosthetic cast applied by certified prosthetist with stump socks, contoured felt padding, special suspension; metal pylon + prosthetic foot attached
- Rigid stump dressings beneficial at all amputation levels:
- Controls edema
- Prevents knee flexion contractures (in transtibial amputations)
- Decreases hospital stay and cost
- Helps upright posture (benefits respiratory, cardiovascular, urinary, GI systems)
- Allows earlier definitive prosthetic fitting
- Has psychological benefits - Campbell's, p. 841-842
Pain Management
Multimodal analgesia regimen:
| Category | Agents |
|---|---|
| Principal - Regional | Central neuraxial / peripheral nerve block (single-shot or continuous catheter); local infiltration analgesia |
| Principal - Opioid | Oxycodone, morphine, fentanyl, hydromorphone |
| Principal - Systemic nonopioid | Acetaminophen, NSAIDs |
| Adjuvants - Gabapentinoids | Gabapentin, pregabalin |
| Adjuvants - NMDA antagonists | Ketamine, memantine, dextromethorphan, magnesium |
| Adjuvants - Alpha-2 agonists | Clonidine |
| Adjuvants - Glucocorticoids | Dexamethasone |
| Other adjuvants | Antidepressants, calcitonin, capsaicin, cannabinoid, lidocaine |
Long-acting local anaesthetics like liposomal bupivacaine reduce narcotic consumption. - Campbell's, p. 841
Mobilisation and Exercise
- Drains removed at 48 hours
- Stump elevated (foot of bed raised) to manage edema and pain; never left in dependent position
- Transfemoral amputation precaution: no pillow between thighs or under stump; no flexion/abduction posture (prevents contracture)
- Muscle-setting exercises begin day after surgery under physical therapist supervision
- Bed to chair mobilisation: first postoperative day
- Parallel bar ambulation: within first several days
- Ambulation with walker/crutches: when patient can control limb comfortably - Campbell's, p. 842
7. Phantom Limb Phenomena
Phantom Limb Sensations
- Almost universal; patient should be educated that they are normal
- "Telescoping": during first year, phantom limb gradually shortens toward end of residual limb
Phantom Limb Pain
- Truly bothersome phantom limb pain: less than 10% of amputees (though some reports state up to 80%, due to non-differentiation from sensations)
- More common with:
- Proximal amputations (forequarter / hindquarter)
- Pain in the limb before amputation
- Mechanism: cortical reorganisation - somatosensory cortex shifts, spinal dorsal horn hyperexcitability, thalamic reorganisation; neuroma in stump may increase central reorganisation
Treatment of Phantom Limb Pain
Diverse modalities; no single universally effective method:
- Massage, ice, heat, increased prosthetic use
- Relaxation training, biofeedback
- Sympathetic blockade
- Oral medications: opioids, calcitonin, and ketamine (proven effective in controlled studies); tricyclic antidepressants; gabapentinoids; sodium channel blockers
- Local / epidural nerve blocks
- TENS (minor benefit reported)
- Dorsal column stimulator placement
- Mirror therapy (limited evidence)
- Myoelectric prosthesis use (may alleviate cortical reorganisation)
- General measures: control stump edema, decrease anxiety/stress, good sleep hygiene, decrease depression, smoking cessation - Campbell's, p. 845; Bradley & Daroff Neurology, p. 1104
Stump (Residual Limb) Pain
- Distinct from phantom pain
- Neuroma formation or pressure lesions exacerbate stump pain
- Neuroma is tender to touch/pressure on examination
- May coexist with phantom limb pain
8. Dermatologic Complications of the Stump
| Problem | Cause / Features | Treatment |
|---|---|---|
| Contact dermatitis | Residual detergent in socks; nickel, chromates, rubber antioxidants | Remove irritant, soaks, steroid cream, compression |
| Bacterial folliculitis | Hairy, oily skin; poor hygiene; shaving | Improved hygiene, socket modifications; antibiotics if cellulitis |
| Epidermoid cysts | At socket brim; occur late | Socket modification; excision if severe |
General hygiene: wash stump daily with mild antimicrobial soap, rinse thoroughly, dry completely before donning prosthesis; keep prosthesis clean and dry.
9. Prosthetics
Lower Extremity - Key Points
- A below-knee (transtibial) amputation preserves the knee joint and gives the best chance of walking with a prosthesis
- Knee disarticulation provides longer lever arm, balanced musculature, improved sitting stability/comfort - preferred for non-ambulatory patients over transfemoral
- Transfemoral prosthetics require significantly greater energy expenditure
Upper Extremity
- Wrist/transcarpal level: preserves pronation/supination (valuable even though only 50% transmitted to prosthesis)
- Myoelectric prostheses (e.g. forearm) with interchangeable terminal devices are available
- Targeted Muscle Reinnervation (TMR) should be considered for patients who are candidates for myoelectric prostheses (especially after forequarter amputation)
- Unlike lower extremity, upper extremity prosthetics must provide sensory feedback as well as terminal device function - Campbell's, p. 907
10. Amputation vs. Limb Salvage (Oncologic Context)
- No study has shown a significant difference between amputation and limb salvage regarding psychological outcome or quality of life in long-term sarcoma survivors
- Patients with amputation: difficulty on steep/rough/slippery surfaces but most active, least worried about damaging the limb
- Patients with arthrodesis: most demanding physical work but difficulty sitting
- Patients with arthroplasty: most sedentary, most protective of limb, least self-conscious
- Patient must make the final decision based on long-term goals and lifestyle - Campbell's, p. 838
Key Take-Home Points:
- Always amputate at the most distal level that will reliably heal - preserves function and reduces energy cost.
- Transcutaneous oxygen (TcPO2) is the most reliable preoperative predictor of wound healing potential.
- Myodesis is preferred over myoplasty for muscle fixation; muscles atrophy 40-60% if not secured.
- Immediate rigid dressings and early mobilisation are standard of care post-amputation.
- Phantom limb pain that is truly bothersome affects <10% of amputees; treat with multimodal approach.
- TMR should be considered for upper extremity amputees seeking myoelectric prosthetics.
This is a shared conversation. Sign in to Orris to start your own chat.