Supine x ray in SBO
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, well-sourced information. Here is the full answer:
Supine X-Ray in Small Bowel Obstruction (SBO)
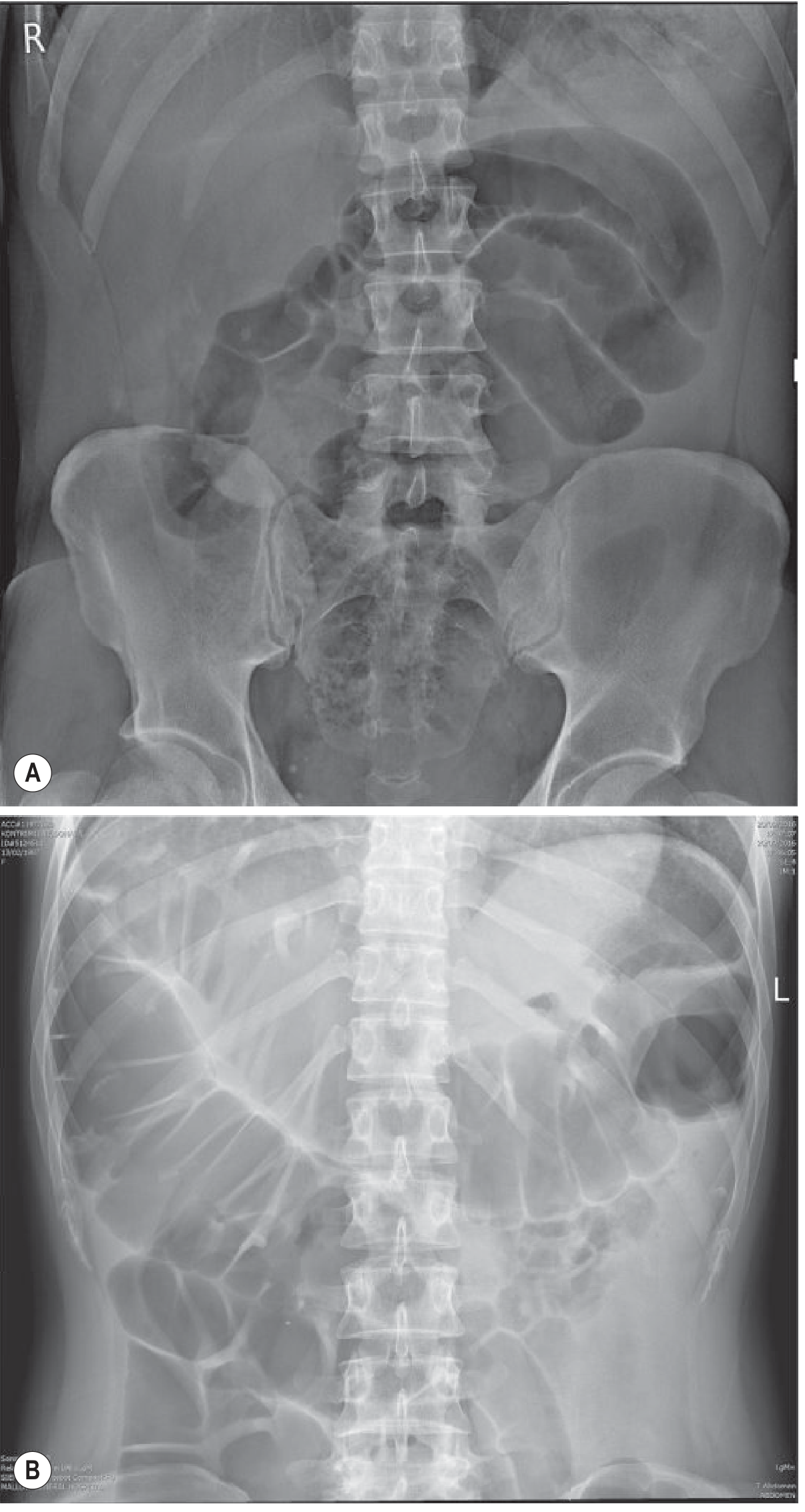
Fig. 18.11 (A) Supine AXR in SBO: centrally located distended small bowel loops with thin, frequent valvulae conniventes. (B) Large bowel obstruction showing peripheral loops with haustra. - Grainger & Allison's Diagnostic Radiology
Key Radiological Features on Supine AXR
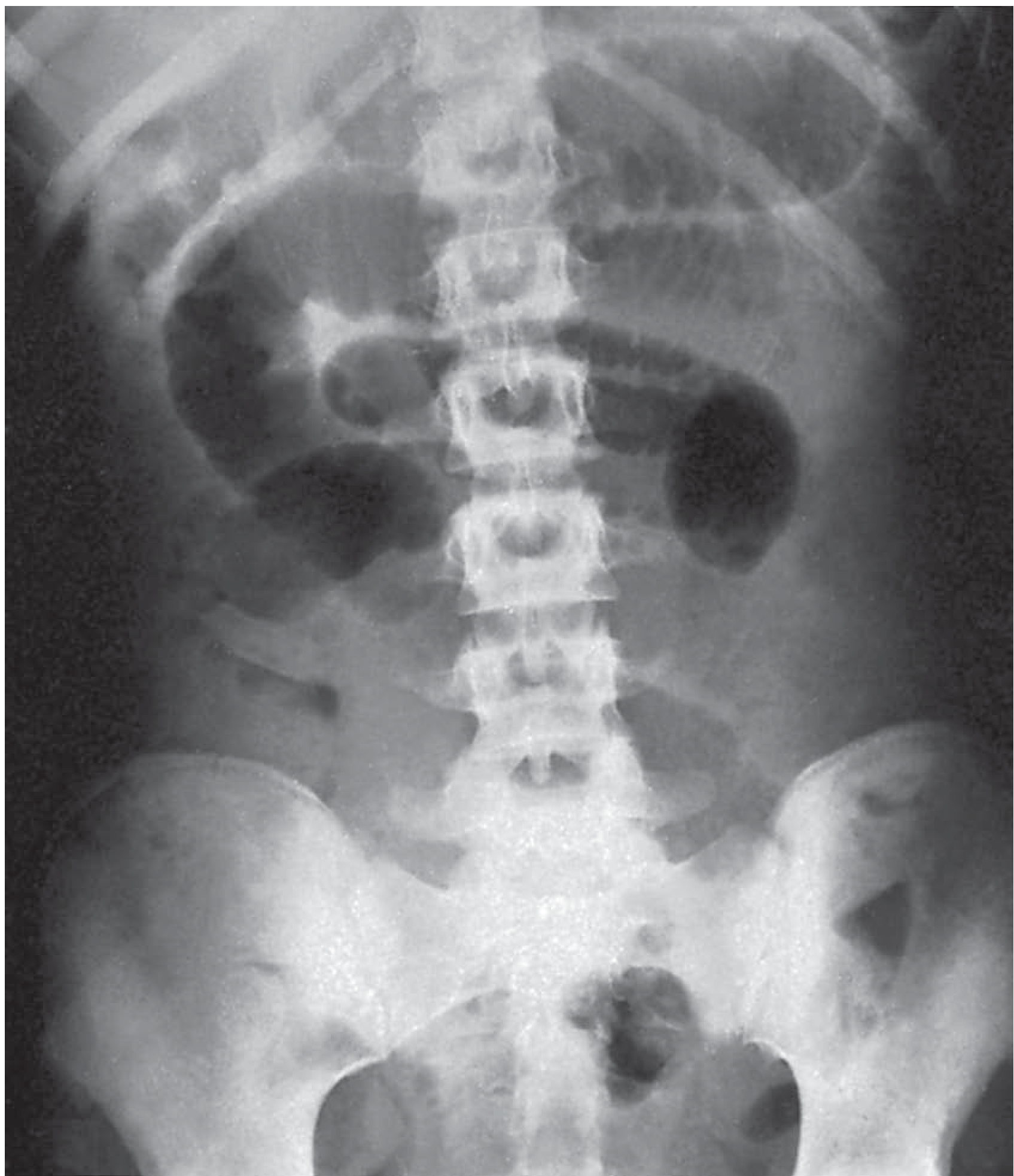
1. Dilated Small Bowel Loops
- Calibre >3 cm (up to 3.5-5 cm) is considered dilated
- Loops lie centrally in the abdomen (vs large bowel which is peripheral)
- Multiple loops arranged in a ladder or step-ladder pattern
2. Valvulae Conniventes (Plicae Circulares)
- The hallmark of small bowel on X-ray
- These folds cross the entire width of the lumen (unlike haustra of the colon, which are incomplete)
- Regularly spaced, giving a "concertina" or "stack of coins" effect - most prominent in jejunum
- The ileum is largely featureless - smooth walls without prominent folds
3. Absent or Minimal Colonic Gas
- Gas is absent from the colon distal to the obstruction - this is an important differentiating feature
- Contrast to paralytic ileus, where both small and large bowel are dilated with gas throughout
4. String of Beads Sign
- Seen when dilated small bowel loops are almost completely fluid-filled (very little gas)
- Residual gas is trapped between valvulae conniventes, forming a line of small gas bubbles
- Virtually diagnostic of SBO when present
- Supine film may appear deceptively normal in fluid-filled SBO (the loops appear as soft-tissue density with no gas to outline them)
5. Normal-Appearing Film (Pitfall)
- In a proportion of SBO cases, the supine AXR is normal or equivocally abnormal
- This occurs when dilated loops are predominantly fluid-filled, with no gas to be seen
- A normal plain film does not exclude SBO - CT is mandatory if clinical suspicion persists
Summary Table: SBO vs LBO on Supine AXR
| Feature | Small Bowel (SBO) | Large Bowel (LBO) |
|---|---|---|
| Position | Central | Peripheral |
| Calibre at obstruction | 3.5-5 cm | 5-8 cm |
| Fold pattern | Valvulae conniventes (complete, regular) | Haustra (incomplete, irregular) |
| Fold appearance | Cross entire diameter, opposite each other | Do not cross full diameter |
| Colonic gas | Absent/minimal | Present proximal to block |
| Caecal gas | May be absent | Usually prominent (rounded, RIF) |
Important Additional Signs
- Hernia: Always inspect below the inguinal ligament on the supine film. A gas-filled loop passing into the inguinal region suggests a strangulated hernia as the cause (especially in women aged >60).
- Pneumobilia (Gallstone Ileus triad - Rigler's triad): SBO + pneumobilia + ectopic gallstone - present in ~38% of cases of gallstone ileus.
- Soft-tissue mass: May indicate intussusception. A "target sign" (concentric rings) is seen if the intussusception is orientated end-on.
- Fluid levels: More prominent on erect film; the number of fluid levels is proportional to the degree and site of obstruction (more levels = more distal obstruction). On supine alone, fluid levels are not visible.
Limitation of Supine AXR
Supine AXR has significant limitations - it can appear normal in up to a third of cases. CT abdomen with contrast is now the modality of choice for:
- Identifying the transition point (dilated proximal loops + collapsed distal loops)
- Determining the aetiology (adhesions, hernia, mass, volvulus, intussusception)
- Detecting complications - strangulation, ischaemia, perforation, closed-loop obstruction
"A normal plain radiograph does not exclude an obstruction - if there is persistent concern, further imaging is indicated; CT is the modality of choice." - Bailey & Love's Surgery, 28th Ed.
Sources: Grainger & Allison's Diagnostic Radiology (p. 464-465); Bailey & Love's Short Practice of Surgery, 28th Ed. (p. 158, 1405); S Das Manual on Clinical Surgery, 13th Ed.
How to check air fluid levels in x ray for sbo
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have everything needed. Here is the complete, well-illustrated answer:
How to Check Air-Fluid Levels in X-Ray for SBO
First, the Critical Point: Supine vs Erect
You CANNOT see air-fluid levels on a supine (lying flat) X-ray.
On supine, gas floats to the top and fluid layers at the bottom - but because you are shooting through the patient from front to back, the gas-fluid interface is horizontal and parallel to the beam. It is therefore invisible. You only see the gas pattern (dilated loops, valvulae conniventes).
To see air-fluid levels, you need the X-ray beam to be horizontal and the interface to be perpendicular to it. This requires:
| View | How Taken | Air-Fluid Levels Visible? |
|---|---|---|
| Supine AXR | Patient lying flat, beam vertical | No - interface parallel to beam |
| Erect AXR | Patient standing/sitting up, beam horizontal | Yes - beam cuts across interface |
| Left lateral decubitus | Patient lying on left side, beam horizontal | Yes - alternative if patient can't stand |
The Erect AXR - Step by Step
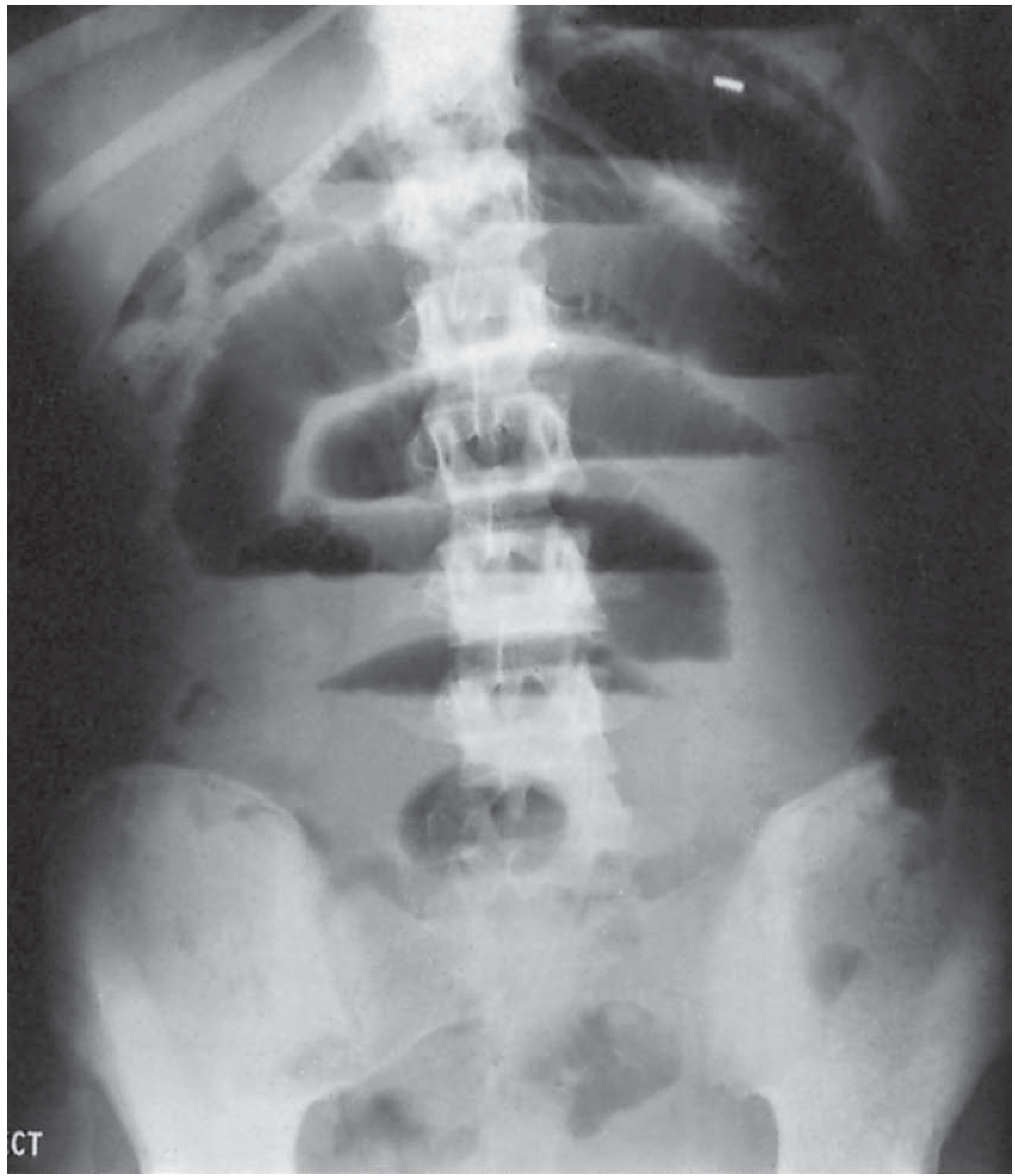
Fig 78.13 - Erect AXR in SBO: classic stepladder pattern - fluid levels with gas above. Ileal obstruction from adhesions. - Bailey & Love's Surgery, 28th Ed.
What you see on erect AXR:
- Air-fluid levels - sharp horizontal white lines at the gas-fluid interface within each bowel loop
- Gas above (dark on X-ray) + fluid below (grey/white on X-ray) within the same loop
- The levels are at different heights in different loops - this is the stepladder pattern, and is the classic SBO appearance
Specific Criteria for SBO on Erect AXR (Box 91.2, Sabiston)
| Finding | Significance |
|---|---|
| Multiple air-fluid levels (≥2) | Suggests obstruction |
| Air-fluid levels >2.5 cm long | More specific for SBO |
| Two fluid levels of unequal height within the same loop | Highly specific for SBO |
| String of beads sign | Virtually diagnostic - tiny gas bubbles trapped between valvulae in a fluid-filled loop |
"The most specific finding for SBO is the triad of: dilated small bowel loops (>3 cm), air-fluid levels on upright films, and absence of gas in the colon." - Schwartz's Principles of Surgery, 11th Ed.
What the "Stepladder Pattern" Means
- Multiple bowel loops, each with their own air-fluid level, but the levels are at progressively different heights across the film
- Looks like a staircase or ladder going across the abdomen
- The loops are arranged transversely, centrally, with their valvulae conniventes visible
- This pattern occurs because each loop has trapped a different amount of fluid/gas and they do not all empty into each other
Fluid Levels - What They Tell You
- Fluid levels appear later than gas shadows (gas accumulates first, then fluid catches up and separates)
- The number of fluid levels is directly proportional to:
- The degree of obstruction (more complete = more levels)
- The site of obstruction (more distal = more levels, as more loops are involved proximal to it)
- When fluid levels are very prominent and numerous, the obstruction is advanced
- Two fluid levels are normal in adults (one at duodenal cap, one at terminal ileum) - don't over-call
Normal AXR Does Not Exclude SBO
A critical pitfall:
- If dilated loops are predominantly fluid-filled (no gas), the supine film may look completely normal - described as a "gasless abdomen" or "pseudotumor sign"
- Even the erect film may show no air-fluid levels if loops contain only fluid
- Plain films miss SBO in up to 20-33% of cases
- CT is mandatory when clinical suspicion remains despite a normal or equivocal X-ray
Three-View Approach for Suspected SBO
The standard plain film workup is three views:
- Supine AXR - assess bowel gas pattern, loop size, valvulae conniventes, absent colonic gas
- Erect AXR - look for air-fluid levels, stepladder pattern, free air under diaphragm
- Erect CXR - look for free air under diaphragm (perforation)
"Free air in the peritoneal cavity, reflecting perforation of a viscus, is best diagnosed on upright or lateral views, and is easily missed on the supine view." - Mulholland & Greenfield's Surgery
Sources: Sabiston Textbook of Surgery, 21st Ed. (Box 91.2); Bailey & Love's Surgery, 28th Ed. (p. 1405); Schwartz's Principles of Surgery, 11th Ed.; Mulholland & Greenfield's Surgery, 7th Ed.
How to check air fluid levels in x ray for SBO according to Bailey and love 28th edition Supine or erect
Finding Sources
Reading File
Loading Image
Loading Image
Here is exactly what Bailey & Love's 28th Edition says, quoted directly:
Air-Fluid Levels in SBO - Bailey & Love's 28th Edition
The Direct Answer: ERECT Radiograph
Bailey & Love's is unambiguous on this. The exact quote from Summary Box 78.9 (p. 1405):
"Small bowel fluid levels may be seen on an erect abdominal radiograph"
And elaborating immediately after:
"Fluid levels seen radiologically appear later than gas shadows as it takes time for gas and fluid to separate. These are most prominent on an erect abdominal radiograph or cross-sectional imaging."
What the Two Views Show (Bailey & Love)
Figure 78.12 - Supine AXR (gas pattern only):
"Gas-filled small bowel loops illustrating valvulae conniventes; patient supine."
- On supine: you see the gas pattern and valvulae conniventes (the "concertina/ladder" folds of jejunum)
- No fluid levels are visible - gas and fluid have not separated from the viewing angle
Figure 78.13 - Erect AXR (fluid levels visible):
"Fluid levels with gas above; 'stepladder pattern'. Ileal obstruction caused by adhesions (erect abdominal radiograph)."
- On erect: fluid settles to the bottom, gas rises - you see a sharp horizontal white line (the interface) with dark gas above it
- Multiple such levels in different loops = the stepladder pattern
Bailey & Love's Key Points on Fluid Levels (p. 1405)
| Point | Bailey & Love's Statement |
|---|---|
| Which view? | Erect abdominal radiograph |
| When do they appear? | Later than gas shadows (takes time for gas and fluid to separate) |
| Most prominent on? | Erect AXR or cross-sectional imaging |
| How many are normal in adults? | Two - one at the duodenal cap, one at the terminal ileum |
| What does the number tell you? | Directly proportional to the degree and site of obstruction |
| More distal obstruction = ? | More fluid levels |
| Pronounced fluid levels = ? | Advanced obstruction |
| Paralysis during obstruction = ? | Fluid levels become more conspicuous and more numerous |
Summary (Bailey & Love's, verbatim logic)
- Supine AXR → shows dilated loops, valvulae conniventes, absent colonic gas
- Erect AXR → shows fluid levels (gas above, fluid below = stepladder pattern)
- Fluid levels appear after gas shadows, so an early SBO may show gas but no fluid levels yet
- A normal plain film does not exclude SBO
Source: Bailey & Love's Short Practice of Surgery, 28th Edition, Summary Box 78.9 and Fig. 78.12-78.13, p. 1405
Why fluid levels are seen in x ray of sbo
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
This is the exact Bailey & Love pathophysiology passage I needed. Now I have everything to give a complete, textbook-accurate answer.
Why Fluid Levels Are Seen in X-Ray of SBO
This is a two-part answer: why fluid accumulates (pathophysiology) and why it becomes visible on X-ray (physics).
Part 1: Why Fluid Accumulates in the Obstructed Bowel
Bailey & Love's 28th Edition (p. 1397) gives the definitive explanation. Distension proximal to the obstruction is caused by two factors - gas and fluid:
Gas (Dark component on X-ray)
"There is a significant overgrowth of both aerobic and anaerobic organisms, resulting in considerable gas production. Following the reabsorption of oxygen and carbon dioxide, the majority is made up of nitrogen (90%) and hydrogen sulphide."
- Bailey & Love's, p. 1397
Additional gas comes from swallowed air (aerophagia). Gas cannot pass beyond the obstruction, so it accumulates and distends the bowel proximally.
Fluid (White/grey component on X-ray)
"Fluid is made up of the various digestive juices:
- Saliva: 500 mL/24h
- Bile: 500 mL/24h
- Pancreatic secretions: 500 mL/24h
- Gastric secretions: 1 litre/24h
This accumulates in the gut lumen as absorption by the obstructed gut is retarded."
- Bailey & Love's, p. 1397
So up to 2.5 litres of digestive secretions per day pour into the gut but cannot be absorbed or pass forward. They pool behind the obstruction.
Fluid is also lost from the intravascular compartment by:
- Reduced oral intake
- Defective intestinal absorption
- Losses from vomiting
- Sequestration in the bowel lumen (the "third space")
- Transudation into the peritoneal cavity
Part 2: Why This Creates a Visible Fluid Level on X-Ray
This is basic physics of density:
| Component | Density | X-ray appearance | Position in upright bowel loop |
|---|---|---|---|
| Gas (nitrogen) | Very low | Dark (black) | Rises to the top |
| Fluid (digestive juices) | High | Grey/white | Settles to the bottom |
When the patient is erect (upright):
- Gas and fluid physically separate within each distended loop
- At the interface, there is an abrupt change from fluid density (white) below to gas density (black) above
- The X-ray beam passes horizontally across this sharp horizontal interface
- This creates the characteristic bright white horizontal line = the fluid level
When the patient is supine:
- Gas and fluid are still both present, but the interface is now parallel to the X-ray beam (both beam and interface are horizontal)
- The beam cannot "cut across" the interface → no fluid level is visible
- You only see the gas outline of the loops
Part 3: Why Fluid Levels Appear LATER Than Gas Shadows (Bailey & Love)
"Fluid levels seen radiologically appear later than gas shadows as it takes time for gas and fluid to separate."
- Bailey & Love's Summary Box 78.9, p. 1405
This is why:
- Early SBO → mostly gas pattern visible on supine, no fluid levels yet on erect
- Established SBO → gas and fluid have separated → fluid levels now visible on erect
- Advanced/paralytic SBO → fluid levels become more conspicuous and more numerous
"During the obstructive process, fluid levels become more conspicuous and more numerous when paralysis has occurred. When fluid levels are pronounced, the obstruction is advanced."
- Bailey & Love's, p. 1405
Summary Diagram (concept)
ERECT AXR - single obstructed loop:
┌───────────────┐
│ GAS (dark) │ ← nitrogen, hydrogen sulphide, swallowed air
├───────────────┤ ← FLUID LEVEL (sharp white horizontal line)
│ FLUID (white) │ ← pooled digestive secretions (up to 2.5L/day)
└───────────────┘
Multiple loops → multiple levels at different heights = STEPLADDER PATTERN
Sources: Bailey & Love's Short Practice of Surgery, 28th Ed. - Pathophysiology of Intestinal Obstruction (p. 1397); Summary Box 78.9 (p. 1405); Schwartz's Principles of Surgery, 11th Ed. - Pathophysiology of SBO
This is a shared conversation. Sign in to Orris to start your own chat.