Portal hypertension.causes,clinical features and management.TIPSS
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
TIPS transjugular intrahepatic portosystemic shunt procedure diagram
Searching PubMed
"portal hypertension" AND "TIPS" AND management
I now have all the material needed for a comprehensive answer. Let me compile it:
Portal Hypertension
Definition
Portal hypertension is defined as elevation of the hepatic venous pressure gradient (HVPG) above 5 mmHg. Clinically significant portal hypertension (CSPH) is defined as HVPG ≥ 10 mmHg, at which point decompensation risk substantially rises. Variceal development and bleeding risk begins when HVPG exceeds 12 mmHg.
— Harrison's Principles of Internal Medicine, 22E
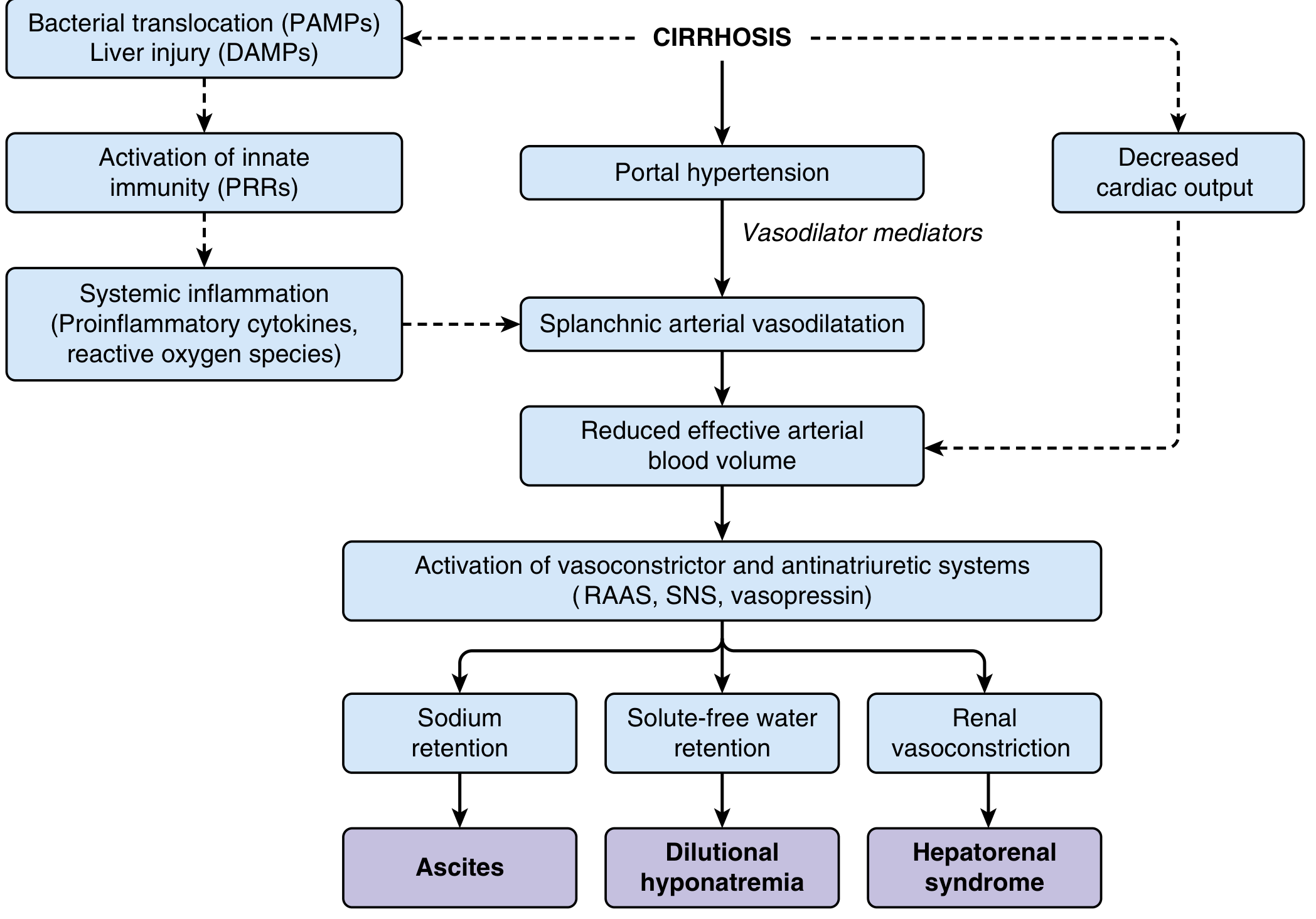
Pathophysiology
Two simultaneous hemodynamic processes combine:
- Increased intrahepatic resistance — cirrhosis causes architectural distortion, collagen deposition in sinusoids (space of Disse), and contraction of hepatic stellate cells (HSCs), raising resistance to portal flow
- Increased splanchnic blood flow — vasodilator mediators (primarily NO) cause splanchnic arterial vasodilation → hyperdynamic circulation → further increases portal inflow
As the disease advances:
- Splanchnic vasodilation → reduced effective arterial blood volume → activation of RAAS, sympathetic nervous system, and ADH → sodium and water retention
- Systemic inflammation via PAMPs (bacterial translocation) and DAMPs (liver injury) amplifies circulatory dysfunction
Causes
Classified by site of obstruction:
Prehepatic
| Cause |
|---|
| Portal vein thrombosis |
| Splenic vein thrombosis |
| Massive splenomegaly (Banti's syndrome) |
| Arteriovenous fistula (excessive inflow) |
| Congenital thrombosis of the portal vein |
Intrahepatic (>95% of all cases)
Presinusoidal
- Schistosomiasis
- Congenital hepatic fibrosis
- Primary biliary cholangitis
- Nodular regenerative hyperplasia
- Idiopathic portal hypertension
Sinusoidal (most common overall)
- Cirrhosis (alcohol, viral hepatitis, NAFLD/NASH — most common in Western countries)
- Alcoholic hepatitis
- Infiltrative liver diseases
- Polycystic liver disease
Postsinusoidal
- Hepatic sinusoidal obstruction syndrome (veno-occlusive disease)
Posthepatic
| Cause |
|---|
| Budd-Chiari syndrome |
| IVC webs or thrombosis |
| Congestive heart failure |
| Constrictive pericarditis |
| Restrictive cardiomyopathy |
Cirrhosis is overwhelmingly the most common cause in North America; worldwide, schistosomiasis and portal vein thrombosis are frequent. Noncirrhotic causes account for ~10% of cases.
— Harrison's 22E; Current Surgical Therapy 14E
Clinical Features
Gastroesophageal Varices
- ~50% of cirrhotics have esophageal varices; ~5–15% develop new varices per year
- One-third of patients with varices will bleed
- Variceal hemorrhage mortality: 20–30% per episode (up to 68% in Child-Pugh C)
- Risk predictors: Child-Pugh class, MELD score, HVPG height, varix size/location, red wale signs, cherry red spots, hematocystic spots, tense ascites
Ascites
- Results from portal hypertension → splanchnic vasodilation → RAAS/SNS activation → sodium and water retention
- Diagnosed clinically and confirmed by serum-ascites albumin gradient (SAAG ≥ 1.1 g/dL = portal hypertensive cause)
- Complications: spontaneous bacterial peritonitis (SBP), dilutional hyponatremia, hepatorenal syndrome (HRS)
Hepatic Encephalopathy (HE)
- Due to gut-derived neurotoxins (ammonia, mercaptans, false neurotransmitters) bypassing the liver
- Precipitants: GI bleeding, infection, volume depletion, hyponatremia, constipation
- Clinical: confusion, personality change, asterixis ("liver flap")
- Grades I–IV
Splenomegaly & Hypersplenism
- Portal congestion → splenic enlargement → pancytopenia (thrombocytopenia most notable)
- Thrombocytopenia is often the first clue to portal hypertension
Other Complications
- Hepatorenal syndrome (HRS) — functional renal failure from severe circulatory dysfunction
- Hepatopulmonary syndrome — intrapulmonary vasodilation causing hypoxaemia
- Portopulmonary hypertension — pulmonary arterial hypertension associated with portal hypertension
- Portal hypertensive gastropathy — gastric mucosal changes from portal venous congestion
- Spontaneous bacterial peritonitis (SBP)
- Hepatic hydrothorax, dilutional hyponatremia, coagulopathy
Diagnosis
- Endoscopy: Gold standard for variceal identification and staging
- HVPG measurement: Interventional radiology; >12 mmHg = variceal bleeding risk
- Transient elastography (liver stiffness): Non-invasive; stiffness <20 kPa + no thrombocytopenia → low risk, surveillance not needed
- CT/MRI abdomen: Nodular liver, portosystemic collaterals, splenomegaly
- Liver biopsy: Gold standard for staging fibrosis but has sampling error; less frequently used
Management
1. Primary Prophylaxis (Prevention of first bleed)
Indications: Medium/large varices, or small varices with high-risk stigmata or decompensated cirrhosis
- Non-selective beta-blockers (NSBBs): Propranolol, nadolol — target heart rate 55–60 bpm; systolic BP >90 mmHg
- Carvedilol — now the preferred NSBB; additional anti-α-adrenergic vasodilating action lowers portal pressure more effectively; may prevent decompensation and improve survival
- Endoscopic Variceal Ligation (EVL) — equivalent efficacy to NSBBs for bleeding prevention; used if NSBBs not tolerated
- NSBBs are generally preferred as first-line (additional benefits beyond bleeding)
2. Active Variceal Hemorrhage
Resuscitation first, then simultaneously:
| Step | Intervention |
|---|---|
| Vasoconstriction | Octreotide, somatostatin, or terlipressin + nitroglycerin infusion |
| Endoscopy | Band ligation (EVL) — first-line; sclerotherapy if visualization difficult |
| Antibiotic prophylaxis | Ceftriaxone or norfloxacin (reduces SBP and mortality) |
| Balloon tamponade | Sengstaken-Blakemore or Minnesota tube — bridge to definitive therapy (<24 h) |
| Refractory (10–20%) | TIPS — >90% success rate |
3. Secondary Prophylaxis (Prevention of rebleed)
- Combination of NSBB + EVL is standard
- TIPS for those who fail medical/endoscopic therapy
4. Ascites Management
- Sodium restriction (88 mmol/day)
- Diuretics: Spironolactone ± furosemide
- Large-volume paracentesis + albumin (8 g/L ascites removed) for tense/refractory ascites
- TIPS for refractory ascites unresponsive to diuretics
- Liver transplantation — definitive
5. Hepatic Encephalopathy
- Identify and treat precipitants
- Lactulose (first-line) — reduces intestinal ammonia production
- Rifaximin — poorly absorbed antibiotic; reduces gut bacteria; preferred for recurrence prevention
- Avoid protein restriction; maintain nutrition
6. Definitive Treatment
- Liver transplantation — gold standard for intrahepatic portal hypertension; cures both liver dysfunction and all complications of portal hypertension
TIPS / TIPSS (Transjugular Intrahepatic Portosystemic Shunt)
Principle
TIPS creates a side-to-side portocaval shunt through the liver parenchyma, effectively reducing portal venous pressure by connecting the portal and hepatic venous systems with a stent.
Technique
- Access the right internal jugular vein → advance catheter into a hepatic venous branch under fluoroscopy
- Pass a needle (Colapinto) through the hepatic vein → portal vein through the liver parenchyma
- Dilate the tract
- Deploy a covered stent (e.g., Viatorr e-PTFE stent) across the tract
- Target: HVPG < 12 mmHg post-procedure
Indications
| Indication | Notes |
|---|---|
| Secondary prevention of variceal rebleeding | After failure of medical + endoscopic therapy |
| Acute refractory variceal hemorrhage | Refractory to pharmacological + endoscopic control (10–20% of cases) |
| Early TIPS in high-risk bleeders | HVPG >20 mmHg; reduces rebleeding when placed within 72 h of index bleed |
| Refractory ascites | Unresponsive to maximal diuretic therapy |
| Refractory hydrothorax | Hepatic hydrothorax not controlled medically |
| Portal hypertensive gastropathy (severe) | |
| Budd-Chiari syndrome | |
| Ectopic variceal bleeding | Systematic review 2024 (PMID 38935315) confirms efficacy |
Contraindications
- Absolute: Congestive heart failure, severe pulmonary hypertension (moderate-severe), uncontrolled hepatic encephalopathy, unrelieved biliary obstruction, severe coagulopathy
- Relative: Tricuspid regurgitation, portal vein thrombosis (relative, specialist decision)
Post-procedure Monitoring
- Doppler ultrasound to monitor shunt patency (stent stenosis/thrombosis is the main long-term issue)
- Covered stents (PTFE) significantly reduce stenosis rates vs. bare metal stents
Complications
| Complication | Notes |
|---|---|
| Hepatic encephalopathy | Most common; occurs in ~25–35% (portosystemic blood bypasses liver) |
| Intra-abdominal hemorrhage | ~1–2%; major complication |
| Heart failure | Increased venous return post-shunt → cardiac decompensation (2025 SR, PMID 40741106) |
| Contrast-induced nephropathy | |
| Hemolytic anemia | Mechanical red cell damage through stent |
| Sepsis | |
| Shunt stenosis/occlusion | Managed with balloon dilation or stent-in-stent |
Outcomes
- Success in controlling hemorrhage: >90%
- TIPS has largely replaced surgical shunt procedures in current practice
- Surgical shunts remain useful when TIPS is not feasible, or in extrahepatic portal hypertension with intact liver function
Summary: Management Algorithm
Portal Hypertension
│
├── Varices present?
│ ├── Primary prophylaxis: NSBBs (carvedilol preferred) or EVL
│ └── Active bleeding:
│ ├── Vasoactive drugs + EVL + antibiotics
│ ├── Refractory → TIPS (>90% success)
│ └── Bridge: Sengstaken-Blakemore tube (<24 h)
│
├── Ascites: Diuretics → paracentesis → TIPS → transplant
├── Encephalopathy: Lactulose + rifaximin + treat precipitants
└── Definitive: Liver transplantation
Key Sources:
- Harrison's Principles of Internal Medicine, 22E — Portal Hypertension chapter
- Current Surgical Therapy, 14E — Portal Hypertension: Role of Shunting Procedures
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease — Pathophysiology of ascites
- Miller's Anesthesia, 10E — TIPS procedural details
Recent Evidence:
- TIPS for ectopic variceal bleeding (systematic review, 2024) — PMID 38935315
- TIPS in hepatocellular carcinoma — meta-analysis, 2024 — PMID 39126599
- Cardiovascular risk and cardiac decompensation post-TIPS — systematic review, 2025 — PMID 40741106
This is a shared conversation. Sign in to Orris to start your own chat.