Anatomyof shoulder joint
Anatomy of the Shoulder Joint (Glenohumeral Joint)
1. Articular Surfaces
- Humeral head - large, rounded, covered in hyaline cartilage; oriented superomedially
- Glenoid cavity - shallow, pear-shaped fossa on the lateral angle of the scapula; covers only about one-third of the humeral head surface area
- Glenoid labrum - fibrocartilaginous rim that deepens the glenoid cavity only slightly, but increases the contact area and contributes to joint stability; the tendon of the long head of biceps brachii attaches at its superior aspect (supraglenoid tubercle)
2. Joint Capsule
- Fibrous capsule attached proximally to the margins of the glenoid cavity (outside the labrum) and distally to the anatomical neck of the humerus (except inferiorly, where it descends to the surgical neck)
- The capsule is loose and thin posteriorly, allowing great mobility
- Anteriorly it is reinforced by the glenohumeral ligaments
- It has two established openings:
- Anterior opening for communication with the subscapularis bursa
- Opening for the tendon of the long head of biceps brachii into the intertubercular groove
3. Ligaments
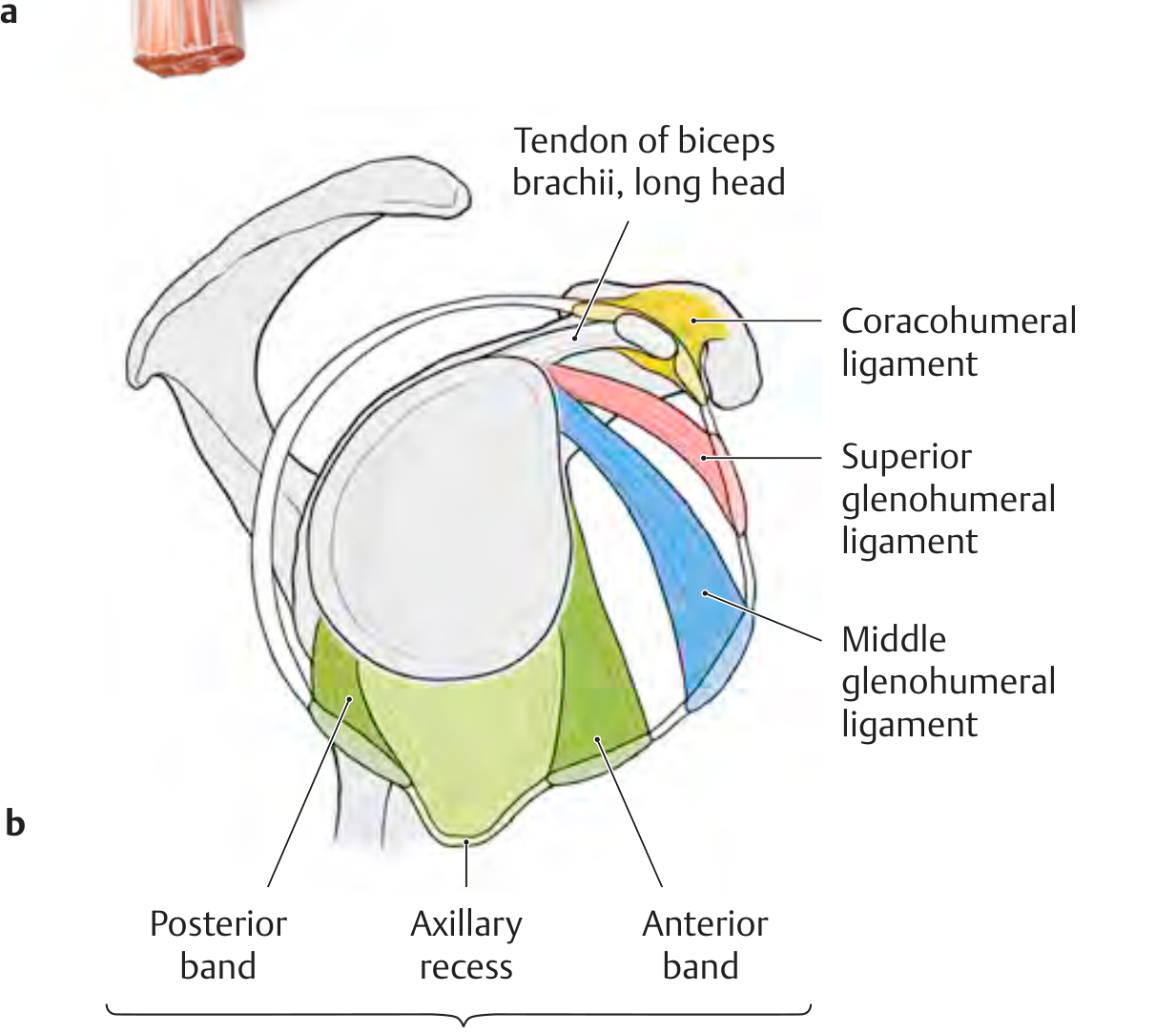
Glenohumeral Ligaments (anterior capsule reinforcement)
| Ligament | Origin | Insertion | Role |
|---|---|---|---|
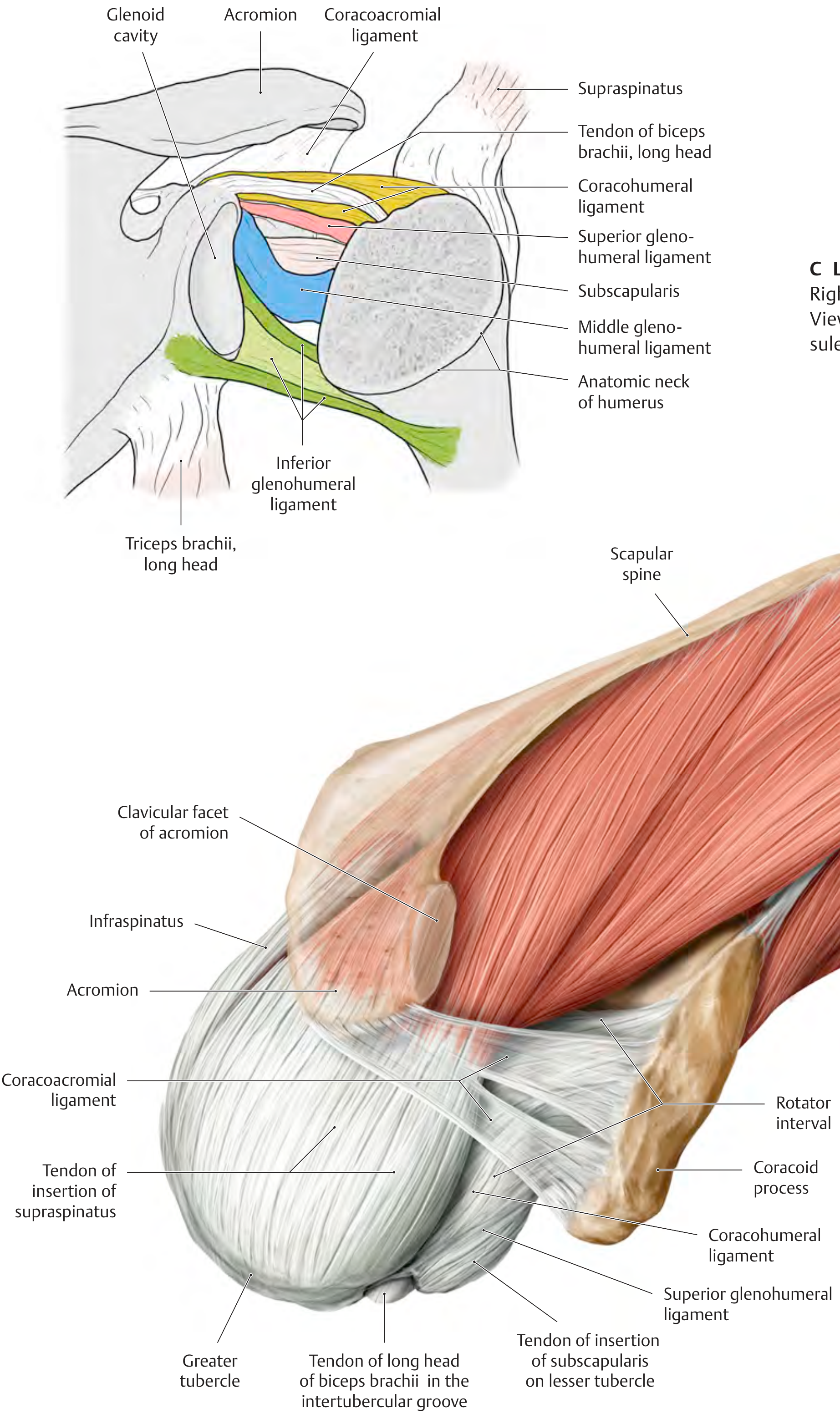
| Superior GHL | Upper margin of glenoid cavity | Intertubercular groove / lesser tubercle | Forms the rotator interval with CHL |
| Middle GHL | Upper margin of glenoid cavity | Anatomic neck of humerus | Passes at ~90° to subscapularis tendon |
| Inferior GHL | Inferior margin of glenoid cavity | Anatomic/surgical neck of humerus | Most important; 3 parts: anterior band, posterior band, axillary recess |
Coracohumeral Ligament (CHL)
- Arises from the base of the coracoid process as a strong, broad band
- Passes to the greater and lesser tubercles of the humerus (two parts)
- Stabilizes the tendon of the long head of biceps brachii and forms the "roof" of the biceps pulley in the rotator interval
Coracoacromial Ligament
- Passes from the coracoid process to the acromion
- Forms the coracoacromial arch (together with the coracoid and acromion), the rigid roof over the subacromial space
- Prevents superior escape of the humeral head
Transverse Humeral Ligament
- Passes between the greater and lesser tubercles, bridging the intertubercular groove
- Holds the long head of biceps tendon in the groove
4. Rotator Interval
5. Subacromial Space and Bursae
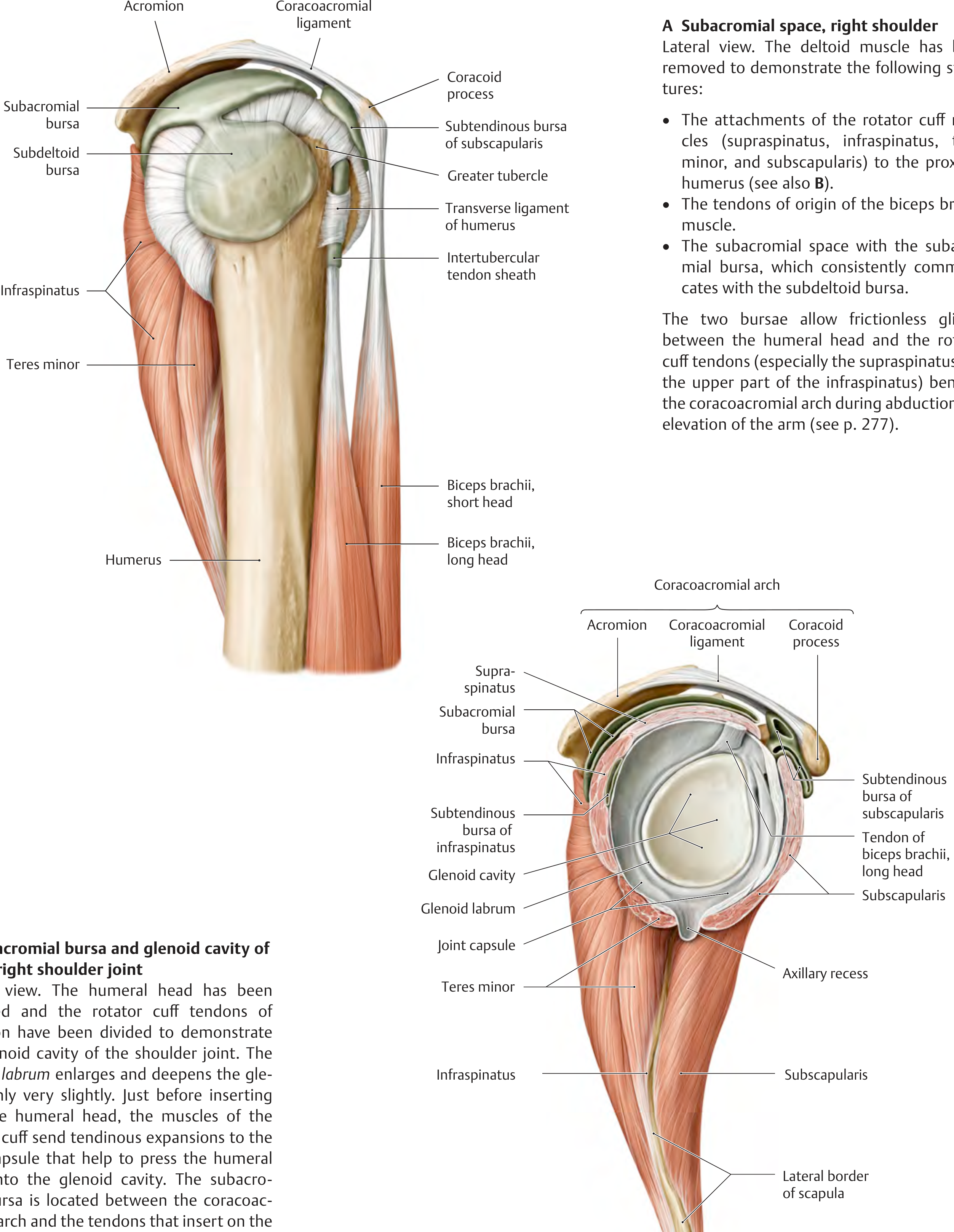
- Subacromial bursa - lies between the coracoacromial arch superiorly and the rotator cuff tendons (especially supraspinatus) inferiorly; consistently communicates with the subdeltoid bursa
- Together these bursae allow frictionless gliding of the humeral head and rotator cuff beneath the arch during abduction and elevation
- Subtendinous bursa of subscapularis - communicates with the joint cavity through the anterior capsule opening
- Subtendinous bursa of infraspinatus - posterior; may communicate with the joint
6. Rotator Cuff (SITS Muscles)
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| Supraspinatus | Supraspinous fossa | Superior facet, greater tubercle | Initiates abduction (first 15°); compresses joint | Suprascapular (C5-C6) |
| Infraspinatus | Infraspinous fossa | Middle facet, greater tubercle | External rotation; compresses joint | Suprascapular (C5-C6) |
| Teres minor | Lateral border of scapula | Inferior facet, greater tubercle | External rotation; compresses joint | Axillary (C5-C6) |
| Subscapularis | Subscapular fossa | Lesser tubercle | Internal rotation; anterior stability | Lower subscapular (C5-C6) |
7. Other Muscles Acting on the Shoulder Joint
- Anterior fibers - flexion and medial rotation
- Middle fibers - abduction (primary bulk of abduction after initiation by supraspinatus)
- Posterior fibers - extension and lateral rotation
- Biceps brachii (long head) - weak flexion and abduction; supination
- Coracobrachialis - flexion and adduction
- Pectoralis major - adduction, medial rotation, flexion (clavicular head)
- Latissimus dorsi - extension, adduction, medial rotation
- Teres major - adduction, medial rotation
8. Neurovascular Supply
Nerve Supply
- Axillary nerve (C5, C6) - from posterior cord of brachial plexus; supplies the joint, deltoid, and teres minor; wraps around the surgical neck of humerus (vulnerable in neck fractures and dislocations)
- Suprascapular nerve (C5, C6) - supplies supraspinatus and infraspinatus
- Musculocutaneous nerve - contributes to the joint capsule anteriorly
- Lateral pectoral nerve - contributes superiorly
Blood Supply (arterial anastomosis around humeral head)
- Anterior circumflex humeral artery (primarily supplies humeral head)
- Posterior circumflex humeral artery - larger; passes with axillary nerve through quadrangular space
- Suprascapular artery
- Subscapular artery and its branches
9. Movements and Range of Motion
| Movement | Range | Primary muscles |
|---|---|---|
| Flexion | 0-180° | Anterior deltoid, pectoralis major (clavicular), biceps |
| Extension | 0-60° | Posterior deltoid, latissimus dorsi, teres major |
| Abduction | 0-180° (first 90° at GH joint) | Supraspinatus (0-15°), then deltoid |
| Adduction | - | Pectoralis major, latissimus dorsi |
| Medial rotation | 0-70° | Subscapularis, pectoralis major, latissimus |
| Lateral rotation | 0-90° | Infraspinatus, teres minor |
| Circumduction | Combined | All of the above |
Note: Full 180° abduction requires 120° at the glenohumeral joint + 60° scapular rotation (scapulothoracic rhythm).
10. Stability Mechanisms
- Static stabilizers - glenoid labrum, joint capsule, glenohumeral ligaments (particularly inferior GHL)
- Dynamic stabilizers - rotator cuff (concavity compression), long head of biceps, deltoid
- Negative intra-articular pressure - vacuum effect within the sealed capsule
- Adhesion-cohesion - synovial fluid surface tension
11. Clinical Correlations
- Anterior dislocation (most common, ~95%) - humeral head displaces anteroinferiorly; damages inferior GHL and labrum (Bankart lesion); may injure axillary nerve
- Hill-Sachs lesion - posterosuperior humeral head impaction fracture from repeated anterior dislocations
- Rotator cuff tears - supraspinatus most commonly torn; presents with painful/weak abduction
- Subacromial impingement - compression of supraspinatus under coracoacromial arch; exacerbated by structural (type III acromion) and dynamic factors
Create an anatomy diagram poster showing the rotator cuff and ligaments
Medical anatomy poster of the shoulder joint showing the rotator cuff muscles and ligaments. The poster should include: ROTATOR CUFF (SITS muscles) clearly labeled: - Supraspinatus (superior, inserting on greater tubercle) - Infraspinatus (posterior, inserting on greater tubercle) - Teres Minor (posterior-inferior, inserting on greater tubercle) - Subscapularis (anterior, inserting on lesser tubercle) LIGAMENTS clearly labeled: - Superior Glenohumeral Ligament - Middle Glenohumeral Ligament - Inferior Glenohumeral Ligament (with anterior band, posterior band, axillary recess) - Coracohumeral Ligament - Coracoacromial Ligament BONY STRUCTURES labeled: - Acromion - Coracoid process - Glenoid cavity - Glenoid labrum - Humeral head - Greater tubercle - Lesser tubercle - Intertubercular groove OTHER STRUCTURES: - Subacromial bursa - Biceps brachii long head tendon - Rotator interval - Coracoacromial arch Show two views side by side: anterior view and posterior view. Use a clean medical illustration style with distinct colors for each rotator cuff muscle (supraspinatus in yellow, infraspinatus in blue, teres minor in green, subscapularis in red/orange). Ligaments in white/cream. Title at top: "SHOULDER JOINT ANATOMY - Rotator Cuff & Ligaments". Include a legend. Professional medical poster format on a dark navy background with white labels.
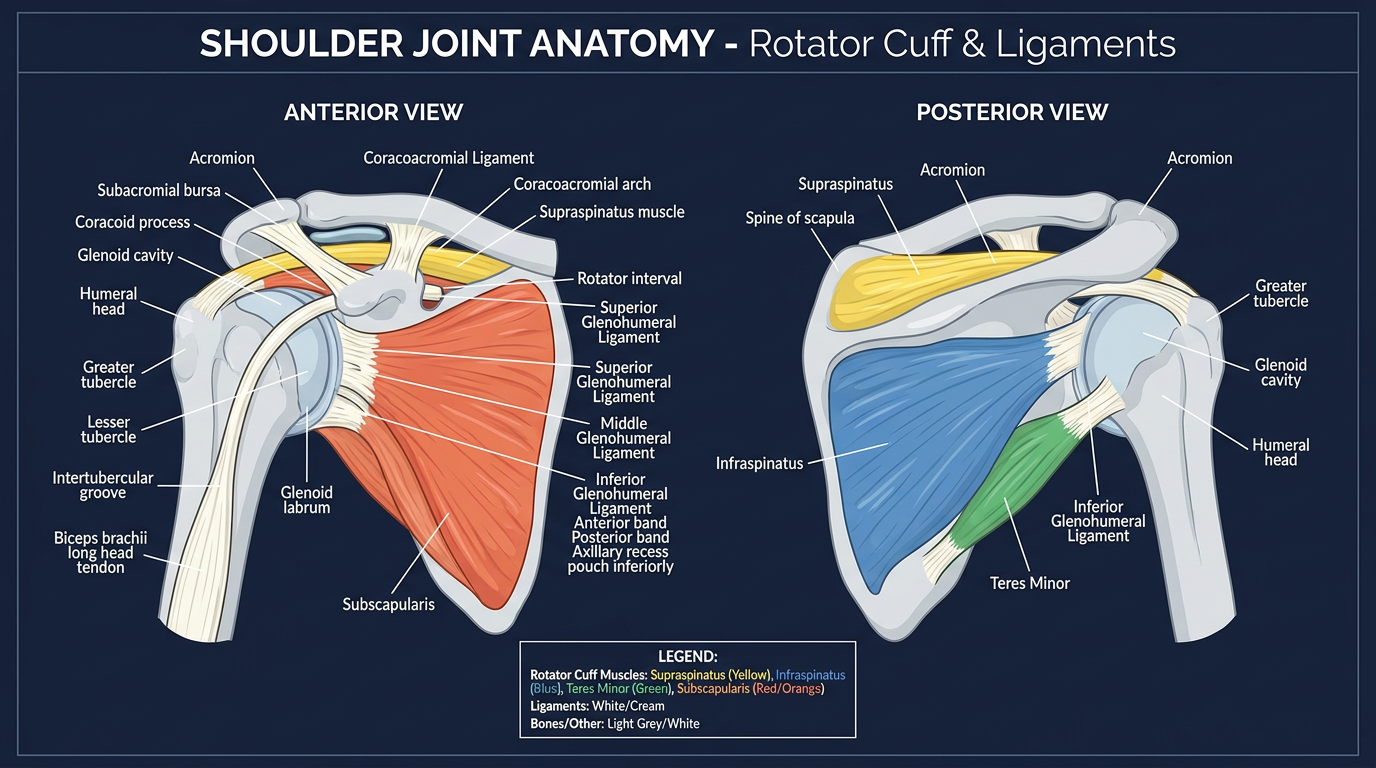
- Supraspinatus, Infraspinatus, Teres Minor, Subscapularis
- Superior, Middle, and Inferior Glenohumeral Ligaments (with the three parts of the IGHL)
- Coracohumeral Ligament
- Coracoacromial Ligament / Arch