Immunotherapy in orthopaedics ms ortho 20 marks answer with proper diagrams .
immunotherapy in orthopaedics MS ortho exam answer 2024
immunotherapy orthopaedic musculoskeletal tumours
Medical education diagram titled "Immunotherapy in Orthopaedics" showing a structured flowchart and classification table. Include: 1) A classification box at top showing three branches: A) Biologic DMARDs (TNF-alpha inhibitors: Infliximab, Etanercept, Adalimumab; IL-6 inhibitors: Tocilizumab; IL-1 inhibitors: Anakinra; T-cell co-stimulation blockers: Abatacept; B-cell depleters: Rituximab), B) Checkpoint Inhibitors (PD-1/PD-L1, CTLA-4 - for bone and soft tissue tumors), C) Other Immunotherapies (Tumor vaccines, CAR-T cell therapy, monoclonal antibodies). 2) A central diagram showing mechanism of action: Antigen presenting cell presenting antigen to T-cell, showing CD80/86 - CD28 co-stimulation pathway, TNF-alpha pathway, IL-6 receptor pathway, with drugs blocking each pathway labeled. 3) A lower table showing Clinical Applications: Rheumatoid Arthritis (biologics), Ankylosing Spondylitis (TNF inhibitors), Psoriatic Arthritis, Osteosarcoma/Ewing's sarcoma (checkpoint inhibitors), Osteoporosis (RANKL inhibitor Denosumab). Clean medical textbook style, white background, clear labeled arrows, professional anatomy diagram style.
Medical diagram showing mechanism of action of TNF-alpha inhibitors and biologics in rheumatoid arthritis for orthopaedic surgery textbook. Show: synovial joint cross-section with inflamed synovium. Label macrophages producing TNF-alpha, IL-1, IL-6. Show T-lymphocyte with CD28 and CD80/86 costimulation. Show B-cell producing autoantibodies (RF, anti-CCP). Show effects: pannus formation, cartilage destruction, bone erosion. Then show drug intervention points with labeled arrows: Infliximab/Adalimumab/Etanercept blocking TNF-alpha; Tocilizumab blocking IL-6 receptor; Abatacept blocking CD80/86; Rituximab depleting B-cells; Anakinra blocking IL-1. Include RANKL/OPG pathway at bone surface showing Denosumab blocking RANKL to prevent osteoclast activation. Professional medical textbook diagram, clean white background, color-coded pathways, clearly labeled arrows and structures.
Medical diagram for MS Orthopaedics exam showing immune checkpoint pathway and immunotherapy in bone and soft tissue tumors (osteosarcoma, Ewing sarcoma, chondrosarcoma). Show: Tumor cell with PD-L1 expression. T-cell with PD-1 receptor. Show PD-L1/PD-1 interaction causing T-cell exhaustion/anergy. Show CTLA-4 on T-cell interacting with APC. Then show checkpoint inhibitors: Pembrolizumab/Nivolumab blocking PD-1; Atezolizumab blocking PD-L1; Ipilimumab blocking CTLA-4 - allowing T-cell activation and tumor cell killing. Include CAR-T cell therapy box showing: T-cell extraction, genetic engineering, CAR-T cell infusion, tumor targeting. Also show tumor microenvironment with regulatory T-cells, MDSCs causing immunosuppression. Professional medical textbook style, clean labels, educational diagram format.
429 Too Many Requests. {'message': '{\n "error": {\n "code": 429,\n "message": "Resource exhausted. Please try again later. Please refer to https://cloud.google.com/vertex-ai/generative-ai/docs/error-code-429 for more details.",\n "status": "RESOURCE_EXHAUSTED"\n }\n}\n', 'status': 'Too Many Requests'}
We encountered an error while processing your request. Please try again or reach out to us for help.
Immunotherapy in orthopaedics ms ortho 20 marks answer with proper diagrams .
Clean medical education classification diagram titled "IMMUNOTHERAPY IN ORTHOPAEDICS - Classification" on white background. Show a hierarchical flowchart tree: Top box "IMMUNOTHERAPY IN ORTHOPAEDICS" branching into 4 main categories: 1. BIOLOGIC DMARDs (shaded blue) with sub-boxes: TNF-alpha Inhibitors (Infliximab, Etanercept, Adalimumab, Certolizumab, Golimumab), IL-6 Inhibitors (Tocilizumab, Sarilumab), IL-1 Inhibitors (Anakinra, Canakinumab), T-cell Costimulation Blocker (Abatacept), B-cell Depleter (Rituximab), IL-17 Inhibitors (Secukinumab, Ixekizumab) 2. JAK INHIBITORS (shaded green): Tofacitinib, Baricitinib, Upadacitinib 3. ANTI-BONE RESORPTION (shaded orange): Denosumab - anti-RANKL monoclonal antibody 4. CHECKPOINT INHIBITORS / ANTI-TUMOR (shaded red): PD-1 inhibitors (Pembrolizumab, Nivolumab), CTLA-4 inhibitor (Ipilimumab), for Osteosarcoma/Soft Tissue Sarcoma Clinical indications labeled below each branch: Rheumatoid Arthritis, Ankylosing Spondylitis, Psoriatic Arthritis, JIA, Osteoporosis, Bone tumors. Medical textbook style, professional, no background clutter.
Detailed medical mechanism diagram titled "Pathogenesis of Bone Destruction in Rheumatoid Arthritis and Sites of Biologic Drug Action" for orthopaedic surgery exam. Show a synovial joint cross-section with inflamed synovium (pannus). Include labeled components: Macrophage releasing TNF-alpha, IL-1, IL-6. Activated T-cell (Th17) with CD28 receptor and CD80/86 on APC. B-cell producing RF and ACPA antibodies. Synovial fibroblast producing RANKL. Osteoclast on bone surface causing erosion. RANKL-RANK interaction on osteoclast precursor. OPG (osteoprotegerin) as decoy receptor. Show drug blocking sites with red inhibitory arrows labeled: INFLIXIMAB/ADALIMUMAB/ETANERCEPT blocking TNF-alpha. TOCILIZUMAB blocking IL-6 receptor. ABATACEPT blocking CD80/86 to CD28. RITUXIMAB depleting B-cell (anti-CD20). ANAKINRA blocking IL-1. DENOSUMAB blocking RANKL. Arrows showing: cartilage erosion, bone erosion, pannus formation. White background, clean professional medical illustration style, all labels clearly visible.
Medical diagram for MS Orthopaedics exam titled "Immune Checkpoint Inhibitors in Bone and Soft Tissue Tumors" on white background. Show two panels: LEFT PANEL - "Normal Immune Response: Cancer Cell Evasion" showing: Tumor cell (osteosarcoma/sarcoma) with PD-L1 on surface. T-cell with PD-1 receptor. Arrow from PD-L1 to PD-1 labeled "INHIBITORY SIGNAL - T cell anergy/exhaustion". Also show CTLA-4 on T-cell binding to B7 on APC blocking CD28 activation. Result box: "T-cell inactivated - Tumor escapes immune destruction". RIGHT PANEL - "Checkpoint Inhibitor Therapy" showing same tumor cell but now: PEMBROLIZUMAB/NIVOLUMAB blocking PD-1 receptor (red cross). ATEZOLIZUMAB blocking PD-L1 (red cross). IPILIMUMAB blocking CTLA-4 (red cross). CD28 now binds B7 freely - T-cell fully activated. Activated cytotoxic T-cell attacking and killing tumor cell. Bottom box showing "Clinical Applications in Orthopaedics: Osteosarcoma, Ewing Sarcoma, Chondrosarcoma, Giant Cell Tumor, Soft Tissue Sarcoma". Professional medical textbook diagram, clean white background.
Medical diagram titled "RANKL-OPG Pathway and Denosumab in Orthopaedics" for MS orthopaedic surgery exam. Show bone remodeling pathway: Osteoblast/stromal cell producing RANKL (receptor activator of NF-kB ligand) and OPG (Osteoprotegerin). RANKL binding to RANK on osteoclast precursor leading to osteoclast differentiation and activation, causing bone resorption (shown as bone with erosion pits). OPG acting as decoy receptor blocking RANKL. Show in Rheumatoid Arthritis context: Th17 cell and synovial fibroblasts producing excess RANKL leading to osteoclast activation and joint erosion. Show DENOSUMAB (human monoclonal antibody) blocking RANKL - labeled "Given SC every 6 months, 60mg for osteoporosis / 120mg monthly for bone metastases". Clinical applications box: Osteoporosis, Bone metastases (from prostate/breast cancer to bone), Giant Cell Tumor of Bone, Prevention of skeletal related events. White background, professional medical illustration, clearly labeled arrows and structures.
IMMUNOTHERAPY IN ORTHOPAEDICS
MS Orthopaedics | 20 Marks Essay Answer
INTRODUCTION
CLASSIFICATION
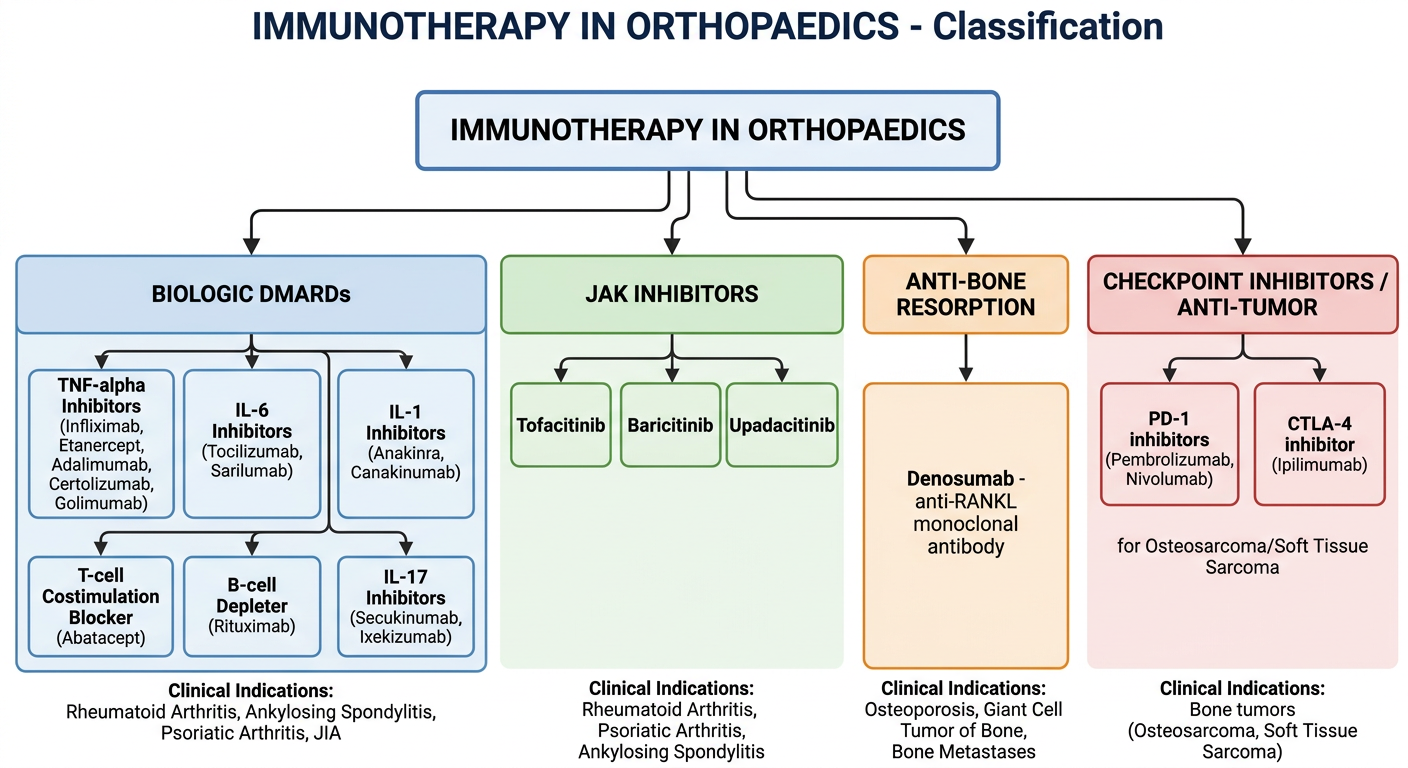
| Category | Agents | Orthopaedic Application |
|---|---|---|
| Biologic DMARDs - TNF-α inhibitors | Infliximab, Etanercept, Adalimumab, Certolizumab, Golimumab | RA, AS, PsA, JIA |
| Biologic DMARDs - IL-6 inhibitors | Tocilizumab, Sarilumab | RA |
| Biologic DMARDs - IL-1 inhibitors | Anakinra, Canakinumab | RA, Systemic JIA |
| T-cell costimulation blocker | Abatacept | RA, PsA |
| B-cell depleter | Rituximab (anti-CD20) | RA |
| IL-17 inhibitors | Secukinumab, Ixekizumab | PsA, AS |
| JAK inhibitors | Tofacitinib, Baricitinib, Upadacitinib | RA, PsA, AS |
| Anti-RANKL | Denosumab | Osteoporosis, GCT bone, Bone metastases |
| Checkpoint inhibitors | Pembrolizumab, Nivolumab, Ipilimumab | Osteosarcoma, STS |
PART 1: BIOLOGICS IN INFLAMMATORY ARTHROPATHIES
Pathogenesis (Basis for Therapy)
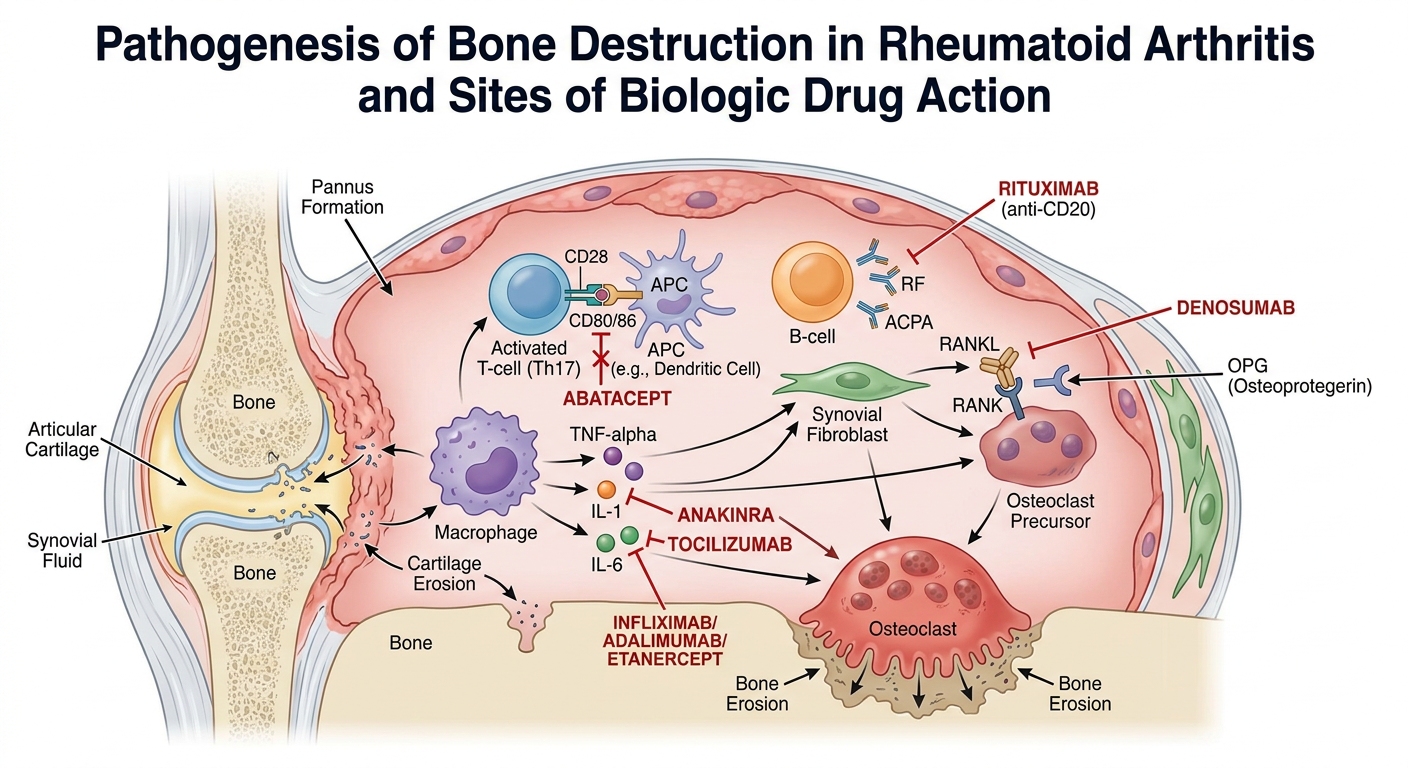
A. TNF-alpha Inhibitors
- IgG1 chimeric monoclonal antibody (mouse Fab + human Fc)
- Dose: 5 mg/kg IV at weeks 0, 2, 6, then every 6-8 weeks
- Used with methotrexate to prevent human anti-chimeric antibodies
- Indicated in RA, AS, PsA, Crohn's disease
- Recombinant TNF receptor p75 fused to IgG1 Fc domain (fusion protein, not a true antibody)
- Dose: 50 mg SC once weekly (or 25 mg twice weekly)
- Self-administered; does NOT require MTX co-therapy
- Approved from age 2 years in JIA
- Fully human monoclonal IgG1 antibody
- Dose: 40 mg SC every 2 weeks
- Broadest indication among TNF inhibitors
- PEGylated Fab' fragment of humanized anti-TNF antibody (no Fc region)
- Safe in pregnancy (does not cross placenta due to absent Fc)
- Dose: 200 mg SC every 2 weeks or 400 mg every 4 weeks
- Fully human monoclonal antibody
- SC 50 mg monthly or IV 2 mg/kg
Key orthopaedic significance: Biologics have produced a significant reduction in rheumatoid hand surgery by preventing disease progression, including MCP subluxation, boutonniere/swan-neck deformities, and extensor tendon ruptures. (Campbell's Operative Orthopaedics 15e)
- Active or latent tuberculosis (screen with Mantoux/IGRA before starting)
- Serious infections, sepsis
- Heart failure (NYHA class III/IV)
- Demyelinating disease (MS, optic neuritis)
- Active malignancy
B. IL-6 Receptor Inhibitors
- Humanized monoclonal antibody against IL-6 receptor
- Effective in RA refractory to TNF inhibitors
- IV 8 mg/kg every 4 weeks or SC 162 mg weekly
- Particularly useful in systemic JIA (IL-6 is central to systemic features)
- Monitor: liver enzymes, lipids, neutrophil count
C. T-Cell Co-stimulation Blocker
- Soluble fusion protein: CTLA-4 extracellular domain + IgG1 Fc
- Blocks CD80/CD86 on APC from binding CD28 on T cells - prevents T-cell activation
- SC 125 mg weekly or IV weight-based monthly
- Indicated in RA, PsA, polyarticular JIA
- Shows decreased cardiovascular risk compared to TNF inhibitors (Katzung's Pharmacology 16e)
D. B-Cell Depletion
- Chimeric monoclonal antibody against CD20 on B cells
- B-cell depletion reduces RANKL levels in synovium, thus reducing joint erosion
- Dose: 1000 mg IV x 2 doses (2 weeks apart), repeated every 6 months
- Preferred in RA with hepatitis B (safer than TNF inhibitors for this) and lymphoma history
E. IL-1 Inhibitors
- Recombinant IL-1 receptor antagonist
- Blocks both IL-1alpha and IL-1beta
- SC injection daily
- Particularly useful in Systemic JIA (Still's disease) and crystal arthropathies (gout)
F. IL-17 Inhibitors
- Target IL-17A - central cytokine in psoriatic arthritis and ankylosing spondylitis
- Secukinumab: 150-300 mg SC; Ixekizumab: 80 mg SC every 4 weeks
- Particularly effective for axial disease and dactylitis/enthesitis in PsA
G. JAK Inhibitors (Targeted Synthetic DMARDs)
| Drug | JAK Selectivity | Dose | Indication |
|---|---|---|---|
| Tofacitinib | JAK1/JAK3 | 5 mg BD or 11 mg SR | RA, PsA, AS |
| Baricitinib | JAK1/JAK2 | 2-4 mg OD | RA |
| Upadacitinib | JAK1 selective | 15-30 mg OD | RA, PsA, AS |
- Oral administration (advantage over injectable biologics)
- JAK inhibitors activate Wnt signaling, increasing osteoblast function and can induce repair of articular bone erosions in RA (Firestein & Kelley)
- Caution: increased risk of VTE, cardiovascular events, herpes zoster; Black Box warning for malignancy in ≥50 year olds with cardiovascular risk
PART 2: DENOSUMAB - ANTI-RANKL THERAPY
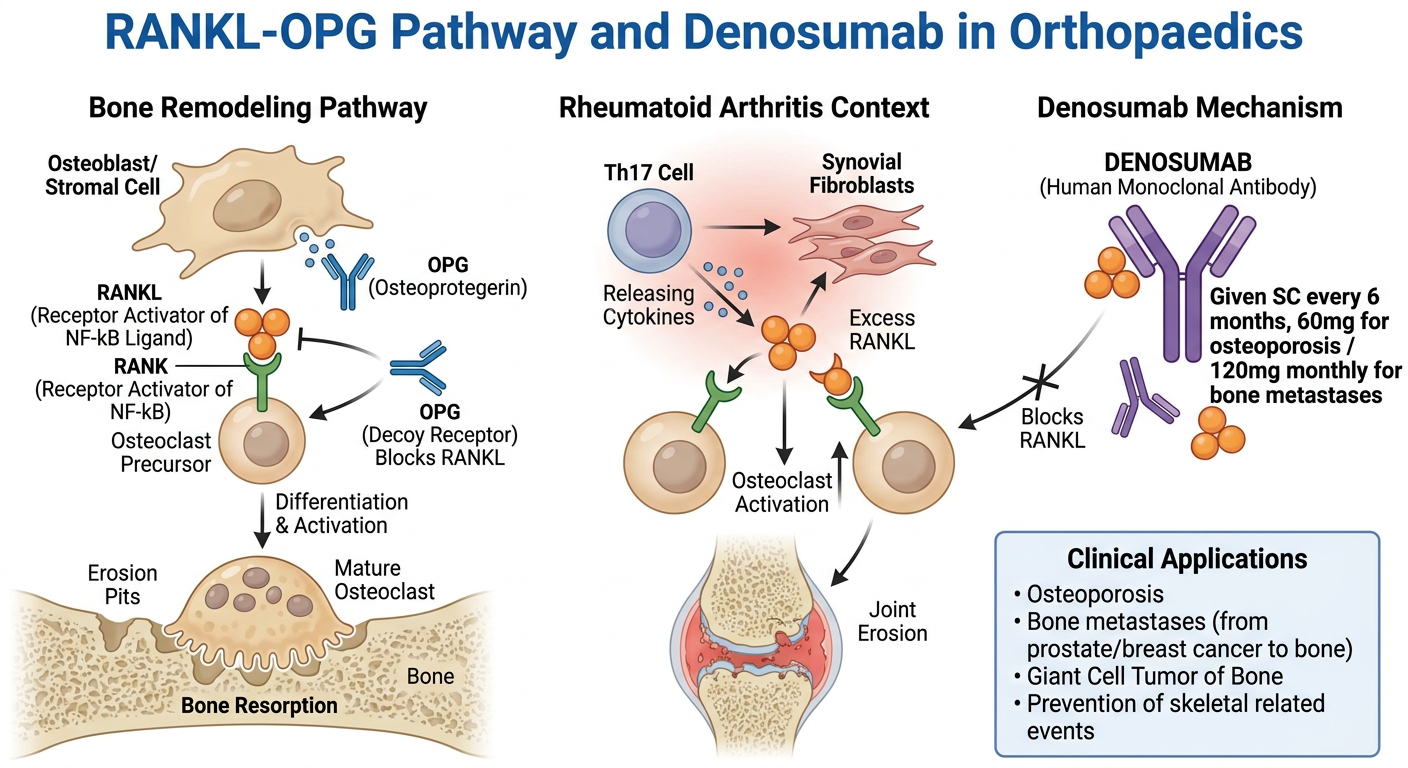
RANKL/RANK/OPG Axis
- RANKL is produced by osteoblasts, synovial fibroblasts, Th17 cells - binds RANK on osteoclast precursors to stimulate osteoclast formation, activation, and survival
- OPG (Osteoprotegerin) is a decoy receptor produced by osteoblasts that neutralizes RANKL, inhibiting osteoclastogenesis
- Denosumab is a fully human monoclonal antibody against RANKL, mimicking OPG
Clinical Applications in Orthopaedics
- 60 mg SC every 6 months (Prolia)
- Significantly reduces vertebral, hip, and non-vertebral fracture risk
- Reduces bone resorption markers within 3 days; effect maintained for 6 months
- At least as effective as potent bisphosphonates; preferred in renal impairment (unlike bisphosphonates)
- Risk of rebound vertebral fractures on discontinuation - transition to bisphosphonate required
- GCT stromal cells express RANKL; osteoclast-like giant cells express RANK
- Denosumab 120 mg SC monthly (Xgeva) - dramatically reduces osteoclast-rich giant cells, produces sclerotic rim, may allow limb salvage surgery
- Can convert unresectable/spine GCTB to resectable
- 120 mg SC monthly - superior to zoledronic acid in delaying SREs in prostate and breast cancer
- Used in bone metastases from any primary tumor
- Denosumab + DMARDs: significantly reduces joint destruction and increases BMD in RA (Firestein & Kelley)
PART 3: IMMUNE CHECKPOINT INHIBITORS IN MUSCULOSKELETAL TUMORS
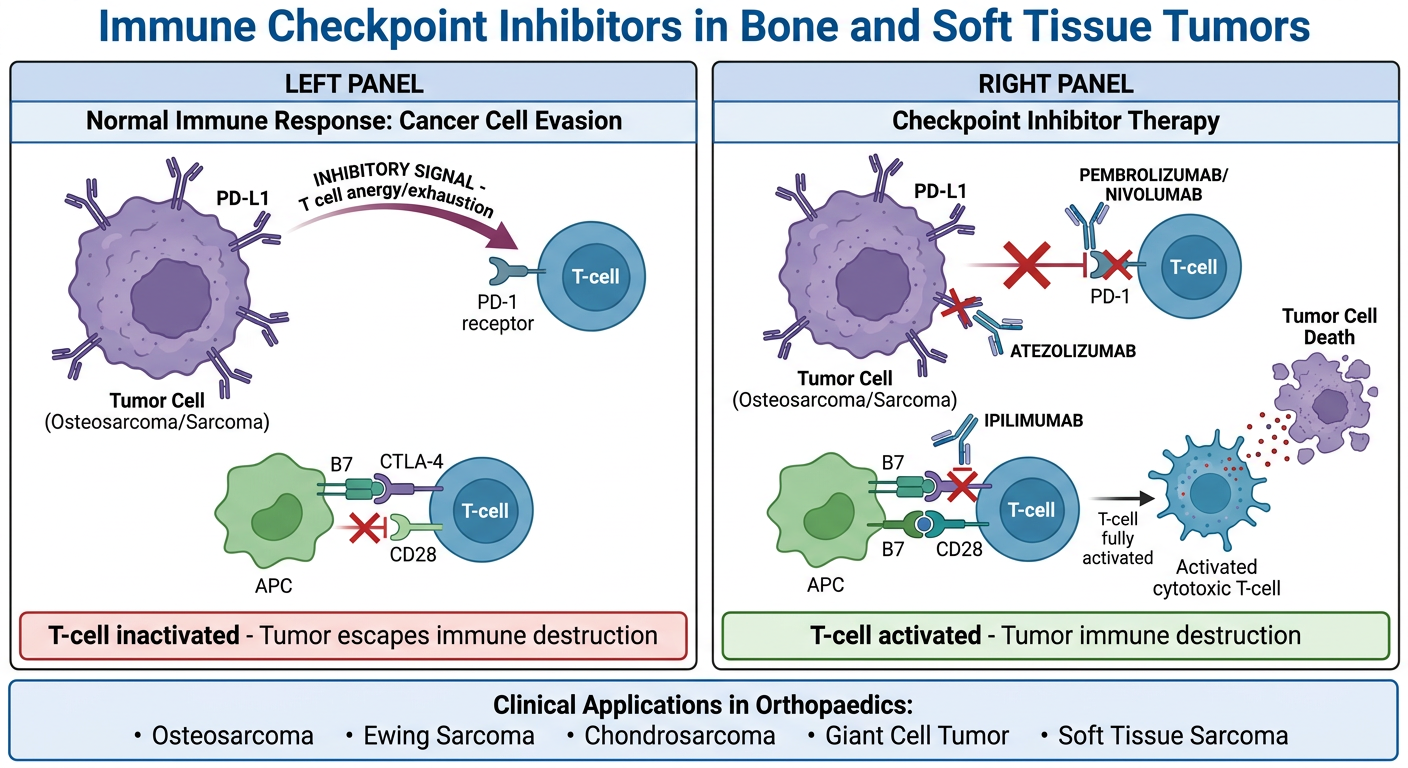
Mechanism of Tumor Immune Evasion
- PD-L1/PD-L2 overexpression - binds PD-1 on T-cells, activating phosphatases that inhibit T-cell activation (T-cell exhaustion/anergy)
- CTLA-4 upregulation - binds B7 (CD80/CD86) on APCs, blocking CD28 co-stimulation of T-cells
- TGF-beta secretion - potent immunosuppressant
- Regulatory T-cell (Treg) induction - promotes immunosuppression in tumor microenvironment
- Myeloid-derived suppressor cells (MDSC) - further suppress T-cell function
- Loss of MHC class I expression - prevents antigen presentation
Checkpoint Inhibitor Drugs
| Drug | Target | Type |
|---|---|---|
| Pembrolizumab | PD-1 | Humanized IgG4 mAb |
| Nivolumab | PD-1 | Fully human IgG4 mAb |
| Atezolizumab | PD-L1 | Humanized IgG1 mAb |
| Ipilimumab | CTLA-4 | Fully human IgG1 mAb |
Applications in Bone and Soft Tissue Tumors
- High grade, poor prognosis after metastasis
- PD-L1 expression found in ~30-40% of osteosarcomas
- Pembrolizumab used in relapsed/refractory osteosarcoma (SARC028 trial)
- Response rates modest as single agents; combination strategies under investigation
- High tumor mutation burden in some cases
- PD-1/PD-L1 inhibitors in clinical trials
- Soft tissue sarcomas with higher immune infiltrate show better checkpoint inhibitor responses
- Denosumab primarily (as above); checkpoint inhibitors for malignant transformation
Adverse Effects of Checkpoint Inhibitors (Immune-Related Adverse Events - irAEs)
| System | Adverse Event |
|---|---|
| Endocrine | Thyroiditis, hypophysitis, adrenal insufficiency, diabetes |
| Joints | Inflammatory arthritis, myositis (orthopaedic relevance!) |
| Skin | Vitiligo, rash, Stevens-Johnson |
| Gut | Colitis, diarrhea |
| Lung | Pneumonitis |
| Heart | Myocarditis |
Orthopaedic relevance of irAEs: Checkpoint inhibitors can produce immune-related inflammatory arthritis - large and small joint synovitis mimicking RA or spondyloarthritis, requiring steroid treatment. Orthopaedic surgeons must recognize and refer these cases urgently.
PART 4: PERIOPERATIVE MANAGEMENT OF PATIENTS ON BIOLOGICS
| Drug Class | Recommendation Before Elective Surgery |
|---|---|
| TNF inhibitors | Hold for 3-5 half-lives before surgery (typically 2-4 weeks) |
| Abatacept | Hold 4 weeks before surgery |
| Rituximab | Delay surgery to 3 months after last infusion |
| JAK inhibitors | Hold 3-7 days before surgery |
| Denosumab | No dose adjustment needed for most orthopaedic surgery |
- Resume after wound healing is confirmed (typically 2 weeks post-op, no active infection)
- All patients on biologics must be screened for latent TB before starting therapy (Mantoux/IGRA + CXR)
- Increased surgical site infection risk; meticulous technique and prophylactic antibiotics essential
SUMMARY TABLE
| Drug | Mechanism | Key Orthopaedic Use | Route/Frequency |
|---|---|---|---|
| Infliximab | Anti-TNF mAb | RA, AS, PsA | IV q6-8 wks |
| Etanercept | TNF receptor fusion protein | RA, AS, PsA, JIA | SC weekly |
| Adalimumab | Anti-TNF mAb | RA, AS, PsA | SC q2 wks |
| Abatacept | CTLA-4-Ig, blocks CD28 | RA | SC weekly / IV monthly |
| Rituximab | Anti-CD20, B-cell depletion | RA | IV x2/6 months |
| Tocilizumab | Anti-IL-6R | RA, Systemic JIA | IV/SC |
| Anakinra | IL-1 receptor antagonist | RA, Systemic JIA | SC daily |
| Secukinumab | Anti-IL-17A | PsA, AS | SC monthly |
| Tofacitinib | JAK1/3 inhibitor | RA, PsA, AS | Oral BD |
| Denosumab | Anti-RANKL mAb | Osteoporosis, GCT, Mets | SC q6m / monthly |
| Pembrolizumab | Anti-PD-1 mAb | Osteosarcoma, STS | IV q3 wks |
| Ipilimumab | Anti-CTLA-4 mAb | Bone/soft tissue tumors | IV |
CONCLUSION
- Firestein & Kelley's Textbook of Rheumatology - Osteoimmunology, TNF Inhibitors chapters
- Campbell's Operative Orthopaedics 15e (2026) - Rheumatoid Arthritis chapter
- Katzung's Basic and Clinical Pharmacology 16e - DMARDs and Biologics chapter
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Tumor Immunology chapter
- Harrison's Principles of Internal Medicine 22e - Bone Metabolism, Denosumab
- Rheumatology 2-Volume Set (Elsevier 2022) - RANKL/OPG, TNF inhibitors