Various techniques for uncinectomy 10 marks answer for ms ent exam
Reading File
Finding Sources
Finding Sources
Searching the Web
uncinectomy techniques FESS endoscopic sinus surgery ENT exam
Reading File
Reading File
Reading File
Reading Web Page
https://www.researchgate.net/publication/352311309_Review_of…
Reading File
Loading Image
Loading Image
I now have excellent, comprehensive content from three major ENT textbooks (Cummings, Scott-Brown's, KJ Lee's) plus endoscopic images. Let me compile a thorough 10-mark MS ENT exam answer.
Techniques of Uncinectomy
Introduction
Uncinectomy - the removal of the uncinate process (UP) - is the first and most important step in Functional Endoscopic Sinus Surgery (FESS). It provides access to the ethmoid infundibulum and the natural ostium of the maxillary sinus, and is the gateway to all further sinus dissection.
Anatomy Relevant to Uncinectomy
The uncinate process is a crescent/boomerang-shaped, mucosal-lined bone of ethmoid origin. It has:
- A vertical segment (superior 2/3): attaches anteriorly to the lacrimal line (anterior maxillary line)
- A horizontal segment (inferior 1/3): attaches inferiorly to the inferior turbinate
- A free posterior edge facing the hiatus semilunaris
- Medially it forms the lateral wall of the middle meatus; laterally lies the lamina papyracea (LP)
The superior attachment of the UP determines frontal sinus drainage:
- Attachment to LP (80%) → frontal drains medial to UP into middle meatus (recessus terminalis formed superiorly)
- Attachment to fovea ethmoidalis or middle turbinate (20%) → frontal drains lateral to UP into infundibulum
Key danger: the lamina papyracea (orbit) lies immediately lateral. Violation = orbital injury.
Instruments Used
| Instrument | Role |
|---|---|
| Freer's elevator / ball-tipped probe | Identify free edge, medialize UP |
| Pediatric backbiter / back-biting forceps | Safe retrograde incision (inferior portion) |
| Sickle knife | Anterograde incision (superior portion only) |
| J-curette | Reflect superior segment medially |
| 90°-angled graspers (push-pull motion) | Remove vertical segment |
| Side-biting / through-biting forceps | Remove horizontal segment |
| Microdebrider | Remove freed uncinate, clean edges |
| 2 mm Kerrison's punch | Remove rough edges |
| Double right-angled ball probe | Dislodge UP forward; probe maxillary ostium |
Techniques of Uncinectomy
1. Retrograde Uncinectomy (Preferred / Standard Technique)
This is the preferred and safer technique as it reduces the risk of orbital penetration.
Steps:
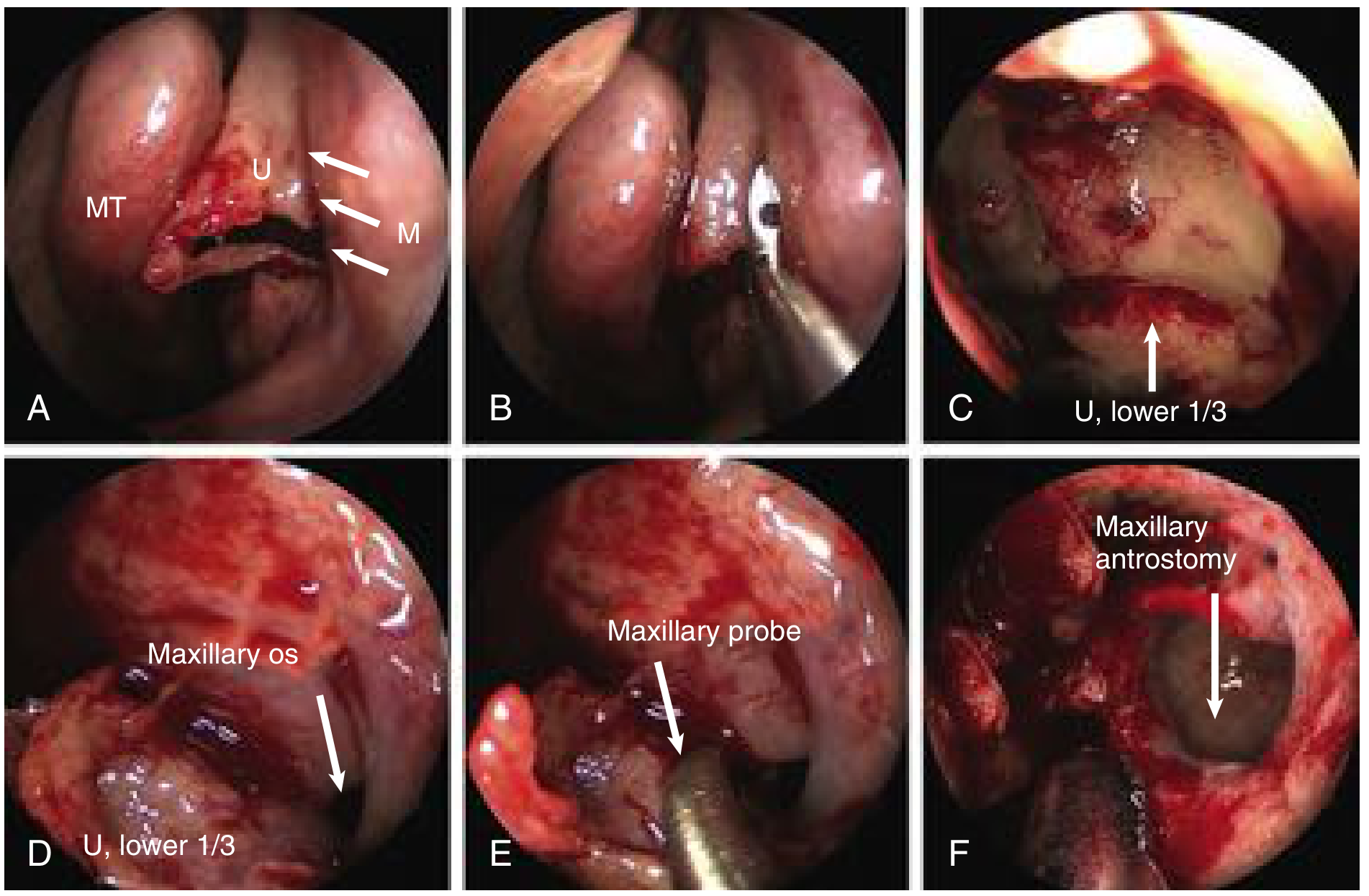
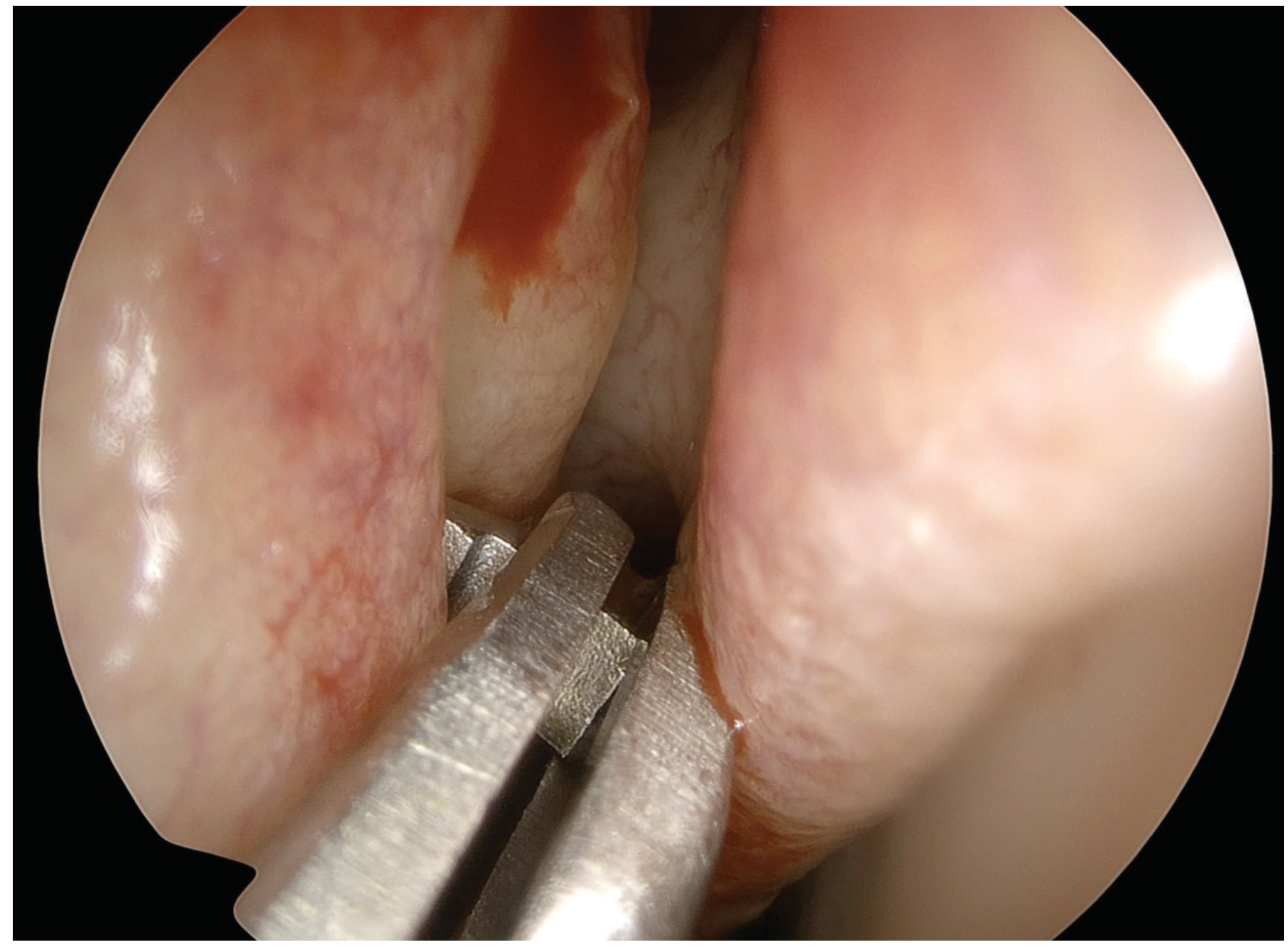
- The uncinate process is identified with a 0° endoscope as a sickle-shaped structure. The posterior free margin (often with a rolled or everted edge when polyps present) is located.
- A ball-tipped probe is slid into the infundibulum behind the posterior free edge to medialize the UP away from the lamina papyracea - especially useful when the UP is atelectatic over the orbit (Silent Sinus Syndrome).
- A pediatric backbiter punch is introduced via the hiatus semilunaris and used to retrogradely incise the UP in an axial plane at the junction of the inferior 1/3 and superior 2/3 - this low position avoids inadvertent orbital penetration and corresponds to the natural maxillary ostium.
- The incision is continued anteriorly until the harder lacrimal bone (anterior maxillary line) is encountered. Penetrating further damages the nasolacrimal duct.
- The middle third is removed with cutting instruments or the microdebrider.
- The superior third may be preserved (to prevent frontal recess scarring) or used later to assist frontal recess dissection.
- The inferior horizontal segment is rotated medially with a maxillary sinus probe and removed with a downbiting instrument and microdebrider.
2. Anterograde (Antegrade) Uncinectomy
An alternative approach using an anterior-to-posterior direction.
Steps:
- A sickle knife (or Freer elevator) is used to make a vertical incision starting on the anterior aspect of the uncinate.
- The incision is continued inferiorly and posteriorly along the crescent-shaped anterior margin of the UP.
- The freed UP is then removed using graspers or microdebrider.
Caution: Use of a sickle knife on the inferior portion of the uncinate should be discouraged as orbital penetration can easily occur here, since the orbit is less protected inferiorly. The sickle knife can be used safely only superiorly, where the hard bone of the frontal process of the maxilla relatively protects the orbit.
3. Backbiter Technique (Inferior Uncinectomy Incision)
Used specifically for the inferior incision when performing uncinectomy:
- Either adult or pediatric back-biting forceps are introduced behind the posterior free margin at the transition zone of the vertical and horizontal segments.
- The incision is made anteriorly to the maxillary line (junction of anterior uncinate border and medial vertical buttress of the maxilla housing the nasolacrimal duct).
- Safer than the sickle knife inferiorly due to reduced risk of orbital entry.
4. Standard KJ Lee Sequence (Step-by-Step Protocol)
As described in KJ Lee's Essential Otolaryngology, the complete uncinectomy proceeds as:
| Step | Action |
|---|---|
| 1 | Visualize the posterior (free) edge of the uncinate |
| 2 | Place pediatric backbiter behind the free margin at the vertical-horizontal transition zone |
| 3 | Cut anteriorly to the maxillary line (level of the nasolacrimal duct - do not violate) |
| 4 | Use a J-curette to reflect the superior segment medially |
| 5 | Remove the vertical segment with 90°-angled graspers (push-pull motion) |
| 6 | Remove the horizontal segment with side-biting and back-biting instruments |
5. Removal of the Horizontal Segment (Inferior Uncinectomy)
This step is often described separately as it is frequently incomplete:
- The horizontal portion extends inferior to the natural ostium of the maxillary sinus.
- Bone of the horizontal portion is dissected free from the mucosa.
- The natural ostium can be stretched open with an angled probe or sucker without removing mucosa (for minimal disease).
- For advanced disease or revision cases, mucosa is removed to create a large middle meatal antrostomy.
- Angled through-biting forceps or the UP can be dislocated forward using a double right-angled ball probe and cautiously removed with the microdebrider.
- Rough edges are removed with a 2 mm Kerrison's punch.
6. Microdebrider-Assisted Uncinectomy
- Used as an adjunct after initial incision with a backbiter or sickle knife.
- The uncinate is mobilized (medialized off the LP) and then the microdebrider is used to resect the freed uncinate in a controlled manner.
- Reduces traction, minimizes mucosal trauma, and handles difficult anatomy (atelectatic UP, polypoid disease) more safely.
- Particularly useful in revision cases where landmarks are distorted.
Key Hazards and How Techniques Address Them
| Hazard | Cause | Prevention |
|---|---|---|
| Orbital penetration | Lamina papyracea lies lateral | Medialize UP with ball probe before incision; use backbiter not sickle knife inferiorly |
| Nasolacrimal duct injury | Anterior maxillary line = NLD housing | Stop incision at anterior maxillary line |
| Frontal recess scarring | Removal of superior UP | Preserve superior 1/3 until frontal dissection |
| Incomplete uncinectomy | Retained horizontal segment | Always address horizontal portion after vertical removal |
| Recirculation | Accessory ostium not connected to natural ostium | Identify and connect natural ostium during antrostomy |
Summary
| Technique | Direction | Key Instrument | Advantage |
|---|---|---|---|
| Retrograde uncinectomy | Posterior → Anterior | Pediatric backbiter | Safest; reduces orbital risk |
| Anterograde uncinectomy | Anterior → Posterior | Sickle knife / elevator | Useful in clear anatomy |
| Backbiter inferior incision | Retrograde axial | Backbiting forceps | Safe inferior approach |
| J-curette + grasper sequence | Superior → Inferior | J-curette, 90° graspers | Systematic segment removal |
| Microdebrider-assisted | Any | Microdebrider | Revision/polypoid cases |
Key points for exam:
- Retrograde uncinectomy is preferred - reduces orbital penetration risk (Cummings, KJ Lee)
- Sickle knife is safe superiorly but dangerous inferiorly (Scott-Brown's)
- Always address the horizontal segment - retained horizontal UP is the most common cause of incomplete uncinectomy and failed maxillary antrostomy
- Stop anteriorly at the maxillary/lacrimal line to protect the nasolacrimal duct
- Ball probe medialization of the UP before incision is a critical safety step in atelectatic UP
Sources: Cummings Otolaryngology Head and Neck Surgery (Flint et al.); Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1; KJ Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.