Blood groups and transfusions answer simple explanation
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Here is a clear, simple explanation of blood groups and transfusions, drawn from medical textbooks.
Blood Groups and Transfusions
What is a Blood Group?
Your blood group is determined by special antigens (marker molecules) sitting on the surface of your red blood cells. Think of them as identity tags. Your immune system also carries antibodies in the blood plasma that attack any antigens it doesn't recognize as "self."
There are two major systems to know: ABO and Rh (Rhesus).
The ABO System
Discovered by Landsteiner in 1900, the ABO system is the single most important blood group for safe transfusions.
The 4 Blood Types
| Blood Type | Antigen on RBCs | Antibodies in Plasma | Universal? |
|---|---|---|---|
| A | A antigen | Anti-B | - |
| B | B antigen | Anti-A | - |
| AB | A and B antigens | None | Universal Recipient |
| O | Neither A nor B | Anti-A and Anti-B | Universal Donor |
- Group AB has no antibodies against A or B, so it can safely receive blood from anyone - universal recipient.
- Group O has no A or B antigens on cells, so nobody's antibodies will attack it - universal donor.
How the Antigens Form (Simple Chemistry)
All humans start with the same basic sugar chain on their red blood cells called the H antigen (the "bare" surface).
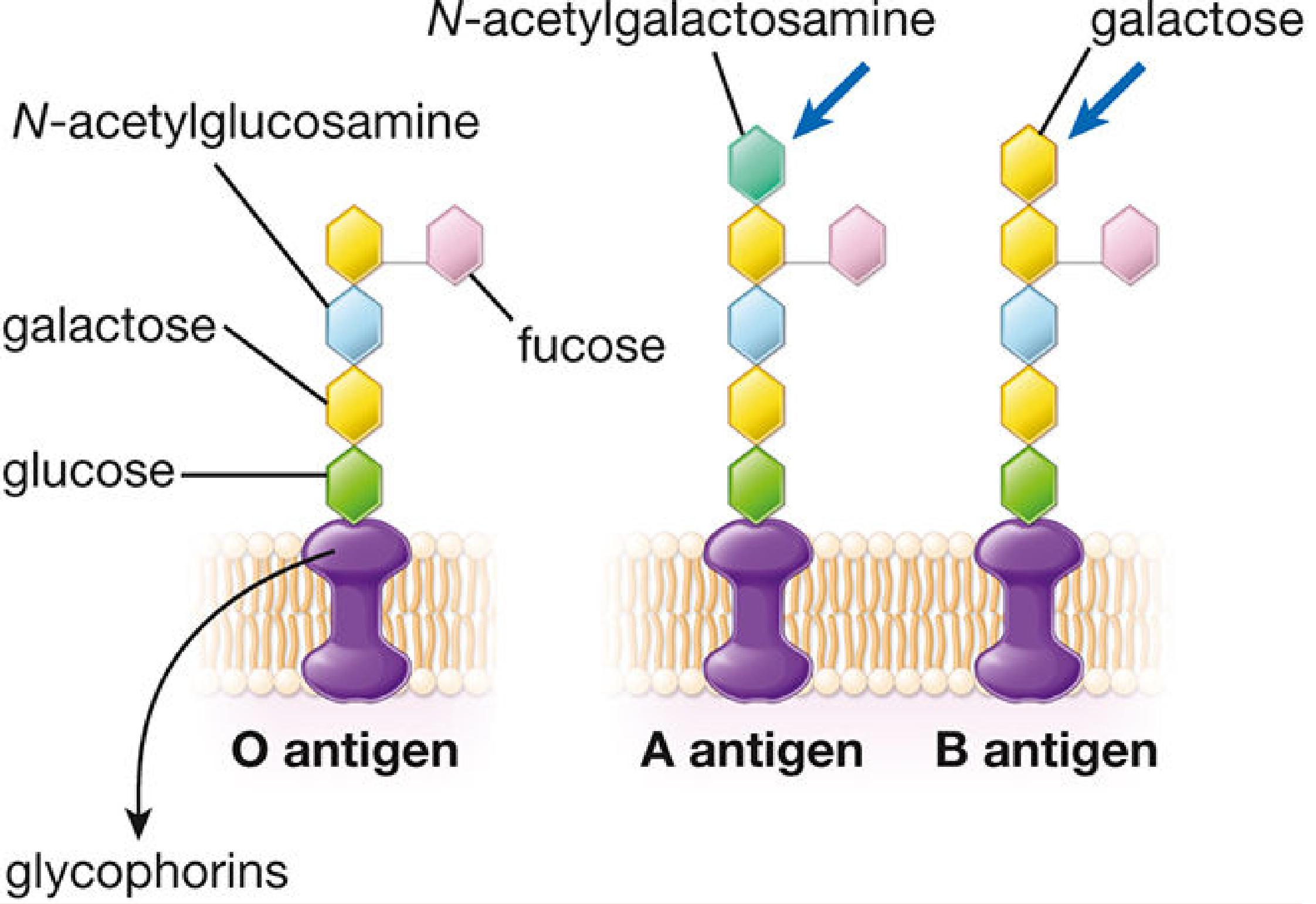
- Type A: An enzyme adds one extra sugar (N-acetylgalactosamine) to the H antigen
- Type B: A different enzyme adds another sugar (galactose) to the H antigen
- Type AB: Both enzymes are present; both sugars get added
- Type O: No enzyme works, so the H antigen stays unmodified
The gene for this enzyme sits on chromosome 9. A and B alleles are codominant; O is recessive.
The Rh (Rhesus) System
The second major system. It revolves mainly around one antigen called D (RhD).
- Rh-positive (Rh+): You carry the D antigen on your red cells (~85% of people)
- Rh-negative (Rh-): You do not carry it (~15% of people)
Unlike ABO, you don't automatically have anti-D antibodies. You only produce them after exposure to Rh+ blood (via transfusion or pregnancy).
Your full blood type is written as a combination: A+, B-, O+, AB-, etc.
Why Blood Matching Matters in Transfusions
What Happens in an ABO Mismatch?
If you receive the wrong ABO blood type, your preexisting antibodies immediately attack the foreign red cells. This is called an acute hemolytic transfusion reaction and it is life-threatening:
- Antibodies bind to the transfused red cells
- The complement system is activated, blowing up the cells (intravascular hemolysis)
- Released hemoglobin floods the kidneys, causing acute kidney failure
- Massive release of cytokines (TNF, IL-1) triggers high fever and shock
- Clotting factors get consumed faster than they're made, leading to disseminated intravascular coagulation (DIC) - the patient can paradoxically bleed to death while blood is clotting everywhere
- Cellular and Molecular Immunology, p. 1156-1157
Delayed Reactions (Minor Antigens)
Mismatches in smaller blood group systems (like Kell, Duffy, Kidd) cause slower reactions: the transfused red cells are gradually destroyed, leading to anemia and jaundice days to weeks later.
Cross-Matching Before Transfusion
Before any transfusion, the lab performs:
- ABO + Rh typing of both donor and recipient
- Cross-match test: Mix the recipient's serum with donor cells to check for hidden reactions
- Full cross-match: ~45 minutes
- Urgent "type-specific" blood (ABO/Rh matched only): ready in 10-15 minutes
- True emergency: O- blood for females, O+ for males
Two healthcare staff must verify the patient's details against the blood bag label before administration to prevent fatal errors.
- Bailey and Love's Short Practice of Surgery, p. 1826-1833
Rh in Pregnancy (Hemolytic Disease of the Newborn)
This is a special and important scenario:
- An Rh- mother carries an Rh+ baby
- Some fetal blood cells leak into the mother's circulation during delivery
- Her immune system makes anti-D antibodies (she is now "sensitized")
- In a second Rh+ pregnancy, these antibodies cross the placenta and attack the baby's red cells
- This causes erythroblastosis fetalis - severe hemolytic anemia in the baby, possibly fatal (hydrops fetalis)
Prevention: Give the mother RhoGAM (anti-D immunoglobulin) during and after each Rh+ pregnancy. It destroys fetal red cells before the mother's immune system can respond, preventing sensitization.
- Histology: A Text and Atlas, p. 683
Summary at a Glance
| Concept | Key Point |
|---|---|
| Blood group | Determined by antigens on red cell surface |
| ABO system | Most important for transfusion safety |
| O blood type | Universal donor (no A/B antigens) |
| AB blood type | Universal recipient (no antibodies) |
| Rh system | D antigen; Rh- people can make anti-D antibodies |
| ABO mismatch | Life-threatening hemolysis, kidney failure, DIC |
| Cross-match | Must be done before every transfusion |
| Rh in pregnancy | Risk of hemolytic disease of newborn; prevent with RhoGAM |
What are other blood grouping system
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Excellent - I now have thorough textbook data on all the major systems. Here is a clear, organized explanation.
Other Blood Group Systems (Beyond ABO and Rh)
There are 45 recognized red blood cell (RBC) blood group systems in total, classified by the International Society of Blood Transfusion (ISBT). Of these, five are routinely tested in clinical practice - Rh, Kell, Duffy, Kidd, and MNS - because testing all five achieves about 95% transfusion compatibility.
- Harrison's Principles of Internal Medicine 22e, p. 945
Quick Overview Table
| ISBT No. | System | Key Antigens | Clinical Significance |
|---|---|---|---|
| 2 | MNS | M, N, S, s, U | M & N - usually insignificant; S, s, U - can cause hemolysis & HDFN |
| 6 | Kell | K, k, Kp^a^, Kp^b^ | Significant - causes delayed hemolysis & HDFN |
| 7 | Lewis | Le^a^, Le^b^ | Usually insignificant; rare hemolysis from anti-Le^a^ |
| 8 | Duffy | Fy^a^, Fy^b^ | Significant - HDFN; Duffy-negative protects against malaria |
| 9 | Kidd | Jk^a^, Jk^b^ | Highly significant - causes sneaky delayed hemolytic reactions |
1. MNS System (ISBT No. 2)
- Antigens are on glycophorin A and B proteins on the red cell surface.
- M and N antigens: Usually naturally occurring IgM antibodies; generally considered clinically harmless unless reactive at body temperature (37°C).
- S, s, and U antigens: These are the dangerous ones - anti-S, anti-s, and anti-U antibodies are clinically significant and can cause both hemolytic transfusion reactions and hemolytic disease of the fetus and newborn (HDFN).
- The rare U-negative phenotype occurs almost exclusively in people of African descent and can cause severe HDFN.
2. Kell System (ISBT No. 6)
Discovered in 1946 when anti-K antibodies were found in a mother whose baby had HDFN.
- K antigen is present in only ~9% of the population (low frequency), while its partner k antigen is in 99.8%.
- Antibodies (anti-K, anti-k) are IgG type, formed after exposure to foreign blood or during pregnancy.
- Clinically important - causes moderate to severe delayed hemolytic transfusion reactions and HDFN.
- Unique feature in pregnancy: Anti-K suppresses fetal red cell production in the bone marrow (erythropoiesis), so fetal anemia is due to lack of production rather than just destruction. This makes it different from other HDFN-causing antibodies.
- The McLeod phenotype (absent Kell expression) is associated with McLeod syndrome - a rare condition causing blood, heart, and nerve/muscle problems.
- Tietz Textbook of Laboratory Medicine, p. 3711
3. Lewis System (ISBT No. 7)
Described in 1946. The Lewis system is unique because Lewis antigens are NOT made directly on red blood cells - they are made in plasma and then absorbed passively onto the RBC surface.
- Two main antigens: Le^a^ and Le^b^, formed by two enzymes (Lewis enzyme and Secretor enzyme).
- Lewis phenotypes:
| Phenotype | Le^a^ | Le^b^ |
|---|---|---|
| Le(a-b+) | Trace | +++ (most common) |
| Le(a+b-) | + | None |
| Le(a+b+) | ++ | ++ (transient, in babies) |
| Le(a-b-) | None | None (seen in pregnancy) |
- Anti-Le^a^ and anti-Le^b^ are IgM antibodies, reactive at room temperature - generally NOT clinically significant for transfusion reactions or HDFN. Rare hemolysis from anti-Le^a^ has been reported.
- During pregnancy, Lewis antigens disappear from the red cell surface (diluted in expanded plasma, absorbed onto lipoproteins), so pregnant women often type as Le(a-b-).
- Tietz Textbook of Laboratory Medicine, p. 3879-3905
4. Duffy System (ISBT No. 8)
Described in 1950, discovered in a multiply-transfused hemophilia patient.
- Key antigens: Fy^a^ and Fy^b^, sitting on a protein called ACKR1 (formerly DARC).
- IgG antibodies; clinically significant for transfusion reactions and HDFN.
Special biological role - Malaria resistance
The ACKR1/DARC protein is the entry receptor that Plasmodium vivax (malaria parasite) uses to invade red blood cells. Many people of West African and Middle Eastern descent carry a genetic mutation that silences Fy^b^ expression on red cells (while it stays expressed on other tissues). Result: Fy(a-b-) individuals are naturally resistant to P. vivax malaria - this explains why P. vivax malaria is rare in West Africa.
- Tietz Textbook of Laboratory Medicine, p. 3712; Robbins Pathology
5. Kidd System (ISBT No. 9)
Described in 1951 - first found in the mother of a newborn with HDFN.
- Key antigens: Jk^a^ and Jk^b^, on the SLC14A1 urea transporter protein.
- IgG antibodies; clinically significant.
The "sneaky" blood group
Kidd antibodies are notorious because:
- They wane over time - can drop to undetectable levels on routine testing.
- If a patient was sensitized in the past but their antibody level has dropped, they may appear compatible at cross-match.
- On re-exposure to incompatible blood, the immune system mounts a rapid anamnestic (memory) response - anti-Kidd antibodies can reappear within 24-48 hours, causing a brisk delayed hemolytic transfusion reaction.
- This is why a thorough antibody history is essential, even if current tests are negative.
- Tietz Textbook of Laboratory Medicine, p. 3712-3713
Other Notable Systems (Less Commonly Tested)
| System | Key Fact |
|---|---|
| P1PK | Anti-P1 usually insignificant; rare anti-P (Tj^r^) causes severe reactions |
| Lutheran | Lutheran antigens on red cells and kidney; anti-Lu^b^ can cause mild HDFN |
| Chido/Rodgers | Antigens from complement proteins (C4a, C4b) absorbed onto RBCs; usually insignificant |
| I system | Anti-I common in cold agglutinin disease; associated with Mycoplasma pneumoniae infection |
| Diego | Clinically significant in South American and East Asian populations |
Why Do These Systems Matter?
- Multi-transfused patients (e.g., sickle cell disease, thalassemia) can develop antibodies to multiple blood group systems over time, making it very hard to find compatible blood.
- Pregnant women - minor group antibodies can cross the placenta and cause HDFN.
- Transplantation - some antigens are expressed on organ endothelium, not just red cells (e.g., ABO, Kell).
- Extended matching (beyond ABO/Rh) for Kell, Duffy, Kidd, and MNS is now standard practice for chronically transfused patients.
Combine both of them write a complete answer
Here is the complete, combined answer on Blood Groups and Transfusions:
Blood Groups and Transfusions - Complete Guide
What is a Blood Group?
Your blood group is determined by antigens (marker molecules) on the surface of your red blood cells. Think of them as identity tags. Your immune system also carries antibodies in the blood plasma that attack any antigens it does not recognize as "self."
There are 45 recognized blood group systems in total. The two most important are the ABO and Rh (Rhesus) systems, but five systems (Rh, Kell, Duffy, Kidd, and MNS) are routinely tested in clinical practice - testing all five achieves about 95% transfusion compatibility.
PART 1: THE ABO SYSTEM
Discovered by Landsteiner in 1900, the ABO system is the single most important blood group for safe transfusions.
The 4 Blood Types
| Blood Type | Antigen on RBCs | Antibodies in Plasma | Universal Role |
|---|---|---|---|
| A | A antigen | Anti-B | - |
| B | B antigen | Anti-A | - |
| AB | A and B antigens | None | Universal Recipient |
| O | Neither A nor B | Anti-A and Anti-B | Universal Donor |
- Group AB - no antibodies against A or B, so it can safely receive blood from anyone.
- Group O - no A or B antigens on cells, so nobody's antibodies will attack it.
How the Antigens Form (Simple Chemistry)
All humans start with the same basic sugar chain on their red blood cells - the H antigen (the bare surface).
- Type A: An enzyme adds one extra sugar (N-acetylgalactosamine) to the H antigen
- Type B: A different enzyme adds another sugar (galactose) to the H antigen
- Type AB: Both enzymes are present; both sugars are added
- Type O: No enzyme works - the H antigen stays unmodified
The gene sits on chromosome 9. A and B alleles are codominant; O is recessive. So six genotypes exist (OO, AA, AO, BB, BO, AB) but produce only four phenotypes (O, A, B, AB).
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, p. 681
PART 2: THE Rh (RHESUS) SYSTEM
The second major system. It revolves mainly around one antigen called the D antigen (RhD).
- Rh-positive (Rh+): You carry the D antigen (~85% of people)
- Rh-negative (Rh-): You do not carry it (~15% of people)
Unlike ABO, you do NOT automatically have anti-D antibodies. You only produce them after exposure to Rh+ blood (via transfusion or pregnancy).
Your full blood type combines both systems: A+, B-, O+, AB-, etc.
The Rh system also contains nearly 56 antigens total (not just D). The most immunogenic are D, C, c, E, and e.
Rh in Pregnancy - Hemolytic Disease of the Newborn (HDFN)
This is a critical clinical scenario:
- An Rh- mother carries an Rh+ baby
- Fetal red cells leak into the mother's circulation during delivery (or miscarriage)
- Her immune system makes anti-D antibodies - she is now "sensitized"
- Usually no problem in the first pregnancy (not enough antibodies)
- In a second Rh+ pregnancy, the antibodies cross the placenta and attack the baby's red cells
- This causes erythroblastosis fetalis - severe hemolytic anemia in the baby, possibly fatal (hydrops fetalis)
Prevention: Give the mother RhoGAM (anti-D immunoglobulin) during and after each Rh+ pregnancy. It destroys fetal red cells in the mother's circulation before her immune system can respond, preventing sensitization entirely.
- Histology: A Text and Atlas, p. 683
PART 3: TRANSFUSIONS
What Happens in an ABO Mismatch?
If you receive the wrong ABO blood type, your preexisting antibodies immediately attack the foreign red cells. This is called an acute hemolytic transfusion reaction and it is life-threatening:
- Antibodies bind to the transfused red cells
- The complement system is activated, exploding the cells (intravascular hemolysis)
- Released hemoglobin floods the kidneys - causing acute kidney failure (renal tubular necrosis)
- Massive cytokine release (TNF, IL-1) triggers high fever and shock
- Clotting factors get consumed faster than they are made - disseminated intravascular coagulation (DIC) develops
- Paradoxically, the patient can bleed to death while blood clots everywhere
- Cellular and Molecular Immunology, p. 1156-1157
Delayed Hemolytic Reactions (Minor Antigens)
Mismatches in smaller blood group systems cause slower reactions. The transfused red cells are gradually destroyed over days to weeks, leading to:
- Worsening anemia
- Jaundice (liver overwhelmed with hemoglobin-derived pigments)
Types of Transfusion Reactions (Summary)
| Type | Cause | Features |
|---|---|---|
| Acute hemolytic | ABO incompatibility | Immediate; fever, shock, DIC, kidney failure - life-threatening |
| Delayed hemolytic | Minor antigen incompatibility | Days to weeks; anemia, jaundice |
| Febrile non-hemolytic | White blood cells in donor blood (graft-vs-host) | Fever, chills, rigors - stop transfusion; rare with leukodepleted blood |
| Allergic | Plasma proteins in donor blood | Urticaria, rarely anaphylaxis |
Cross-Matching Before Transfusion
Before any transfusion, the lab performs:
- ABO + Rh typing of both donor and recipient
- Antibody screen: Look for unexpected antibodies in the recipient
- Cross-match: Mix recipient serum with donor red cells to confirm compatibility
| Urgency | Blood Provided | Time Required |
|---|---|---|
| Full cross-match | ABO+Rh+antibody matched | ~45 minutes |
| Urgent "type-specific" | ABO and Rh matched only | 10-15 minutes |
| True emergency | O- (females) or O+ (males) | Immediate |
Two healthcare staff must always verify the patient's details against the blood bag label before administration - most fatal ABO incompatibility reactions result from patient identification errors, not lab mistakes.
- Bailey and Love's Short Practice of Surgery 28e, p. 1826-1833
PART 4: OTHER BLOOD GROUP SYSTEMS
Beyond ABO and Rh, 43 more systems exist. The five most clinically important ones are below.
1. MNS System (ISBT No. 2)
- Antigens sit on glycophorin A and B proteins on the red cell surface.
- M and N antigens: Usually IgM antibodies reactive only at cold temperatures - generally clinically harmless.
- S, s, and U antigens: These are dangerous - anti-S, anti-s, and anti-U cause hemolytic transfusion reactions and HDFN.
- The U-negative phenotype is rare and occurs almost exclusively in people of African descent - finding compatible blood for these patients is very difficult.
2. Kell System (ISBT No. 6)
Discovered in 1946 through a case of HDFN.
- K antigen: Only ~9% of people carry it (low frequency); its partner k is in 99.8%.
- Antibodies (anti-K, anti-k) are IgG, formed after exposure to foreign blood.
- Causes moderate to severe delayed hemolytic reactions and HDFN.
Unique feature in pregnancy: Anti-K works differently from other HDFN-causing antibodies - it suppresses fetal bone marrow production of red cells rather than just destroying them. Fetal anemia is therefore from lack of production, not just hemolysis.
McLeod phenotype: Absence of Kell protein on red cells. Associated with McLeod syndrome - a rare disorder with combined blood, heart, and nerve/muscle abnormalities.
- Tietz Textbook of Laboratory Medicine, p. 3711
3. Lewis System (ISBT No. 7)
Unique because Lewis antigens are not made on red blood cells - they are made in plasma and passively absorbed onto the RBC surface.
- Two main antigens: Le^a^ and Le^b^, formed by two enzymes (Lewis enzyme from the FUT3 gene; Secretor enzyme from the FUT2 gene).
| Phenotype | Le^a^ | Le^b^ |
|---|---|---|
| Le(a-b+) | Trace | +++ (most common type) |
| Le(a+b-) | + | None |
| Le(a+b+) | ++ | ++ (transient in babies) |
| Le(a-b-) | None | None (seen in pregnancy) |
-
Antibodies are IgM, react at room temperature - generally NOT clinically significant for transfusion or HDFN.
-
During pregnancy, Lewis antigens temporarily disappear from the red cell surface - the mother often types as Le(a-b-).
-
Tietz Textbook of Laboratory Medicine, p. 3879-3905
4. Duffy System (ISBT No. 8)
Discovered in 1950 in a multiply-transfused hemophilia patient.
- Key antigens: Fy^a^ and Fy^b^, on the ACKR1 protein (formerly called DARC).
- IgG antibodies; clinically significant for transfusion reactions and HDFN.
Special biological role - Malaria resistance:
The ACKR1/DARC protein is the entry receptor that Plasmodium vivax uses to invade red blood cells. Many people of West African and Middle Eastern descent carry a mutation silencing Fy^b^ on red cells. Result: Fy(a-b-) individuals are naturally resistant to P. vivax malaria. This is why P. vivax malaria is rare in West Africa.
- Tietz Textbook of Laboratory Medicine, p. 3712; Robbins Pathology
5. Kidd System (ISBT No. 9)
Discovered in 1951 - first found in the mother of a newborn with HDFN.
- Key antigens: Jk^a^ and Jk^b^, on the SLC14A1 urea transporter protein.
- IgG antibodies; clinically significant.
The "sneaky" blood group - notorious for delayed reactions:
- Anti-Kidd antibodies wane over time - they drop to undetectable levels on routine testing
- A patient sensitized years ago may appear compatible at cross-match
- On re-exposure to incompatible blood, immune memory kicks in - anti-Kidd reappears within 24-48 hours
- The resulting delayed hemolytic transfusion reaction can be severe and brisk
- This is why a thorough antibody history is essential even when current tests are negative
- Tietz Textbook of Laboratory Medicine, p. 3712-3713
6. Other Notable Systems
| System | Key Clinical Fact |
|---|---|
| P1PK | Rare anti-P (Tj^r^) causes severe reactions |
| Lutheran | Anti-Lu^b^ can cause mild HDFN |
| I system | Anti-I common in cold agglutinin disease; linked to Mycoplasma pneumoniae infection |
| Diego | Clinically significant in South American and East Asian populations |
| Chido/Rodgers | Derived from complement proteins (C4a, C4b); usually insignificant |
PART 5: WHY ALL THIS MATTERS CLINICALLY
| Clinical Scenario | Relevance |
|---|---|
| Emergency transfusion | Give O- to females of childbearing age, O+ to males |
| Sickle cell / thalassemia | Chronic transfusions cause antibody buildup across multiple systems - extended matching needed |
| Pregnant women | Minor group antibodies (Kell, Duffy, Kidd) cross placenta and cause HDFN |
| Transplantation | ABO and some antigens expressed on organ endothelium - matching essential |
| Repeated transfusions | Antibody screen must be repeated with every admission; Kidd antibodies can disappear then resurge |
The bottom line: ABO and Rh are the first line of matching. Kell, Duffy, Kidd, and MNS are the next tier that prevents the majority of remaining transfusion reactions. For chronically transfused patients, extended phenotype matching across all five major systems is now the standard of care.
This is a shared conversation. Sign in to Orris to start your own chat.