Anatomy of uterus and its ligament. Placement of uterus in pelvic floor ( explanation and include single diagram for each aspect view)
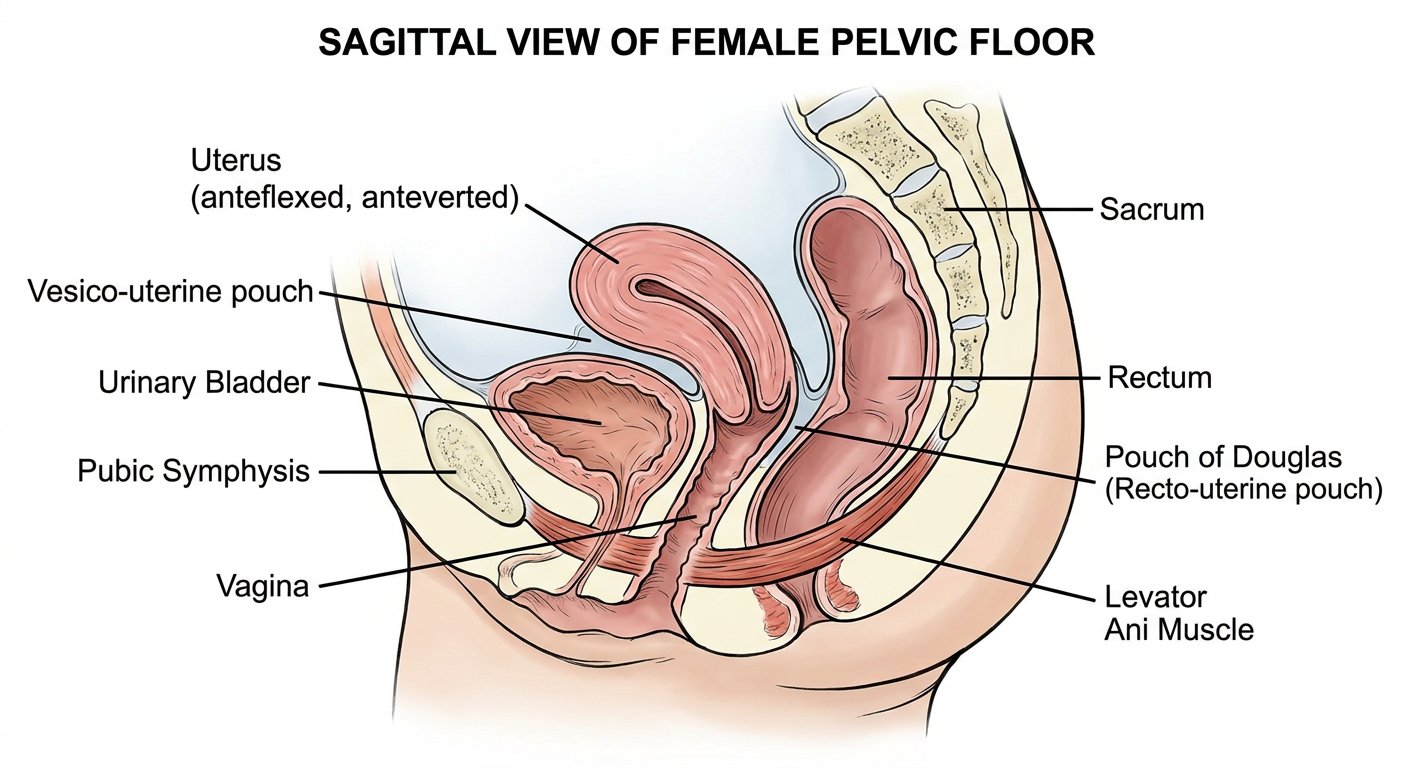
Anatomical diagram of the uterus in the female pelvic floor, sagittal (side) view cross-section showing: uterus in anteflexed anteverted position between the urinary bladder anteriorly and rectum posteriorly, vagina below, pubic symphysis in front, sacrum behind, levator ani muscle of pelvic floor below the uterus, pouch of Douglas (recto-uterine pouch) between uterus and rectum, vesico-uterine pouch between bladder and uterus. All structures clearly labeled with annotation lines. Medical textbook style, clean white background.
Anatomy of the Uterus, Its Ligaments, and Placement in the Pelvic Floor
Part 1 - Anatomy of the Uterus
Regions of the Uterus (Anterior View)
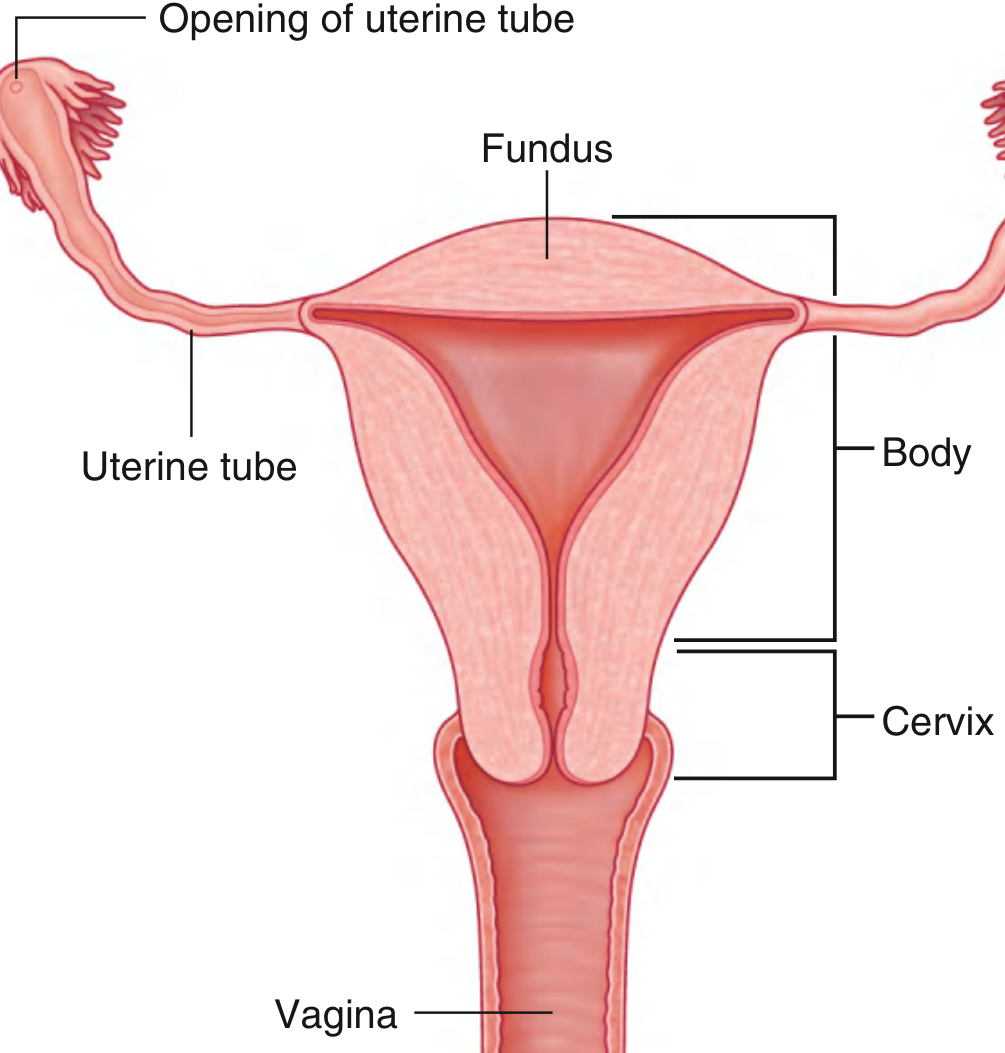
| Part | Description |
|---|---|
| Fundus | The rounded dome-shaped superior end, above the openings of the uterine tubes |
| Body (Corpus) | Main middle portion, flattened anteroposteriorly; houses the triangular endometrial cavity |
| Isthmus (Lower Uterine Segment) | The constricted junction between body and cervix; clinically important in cesarean section |
| Uterine Cornua | Funnel-shaped lateral angles of the body where the fallopian tubes insert |
| Cervix | The lower cylindrical portion, ~3 cm long, divided into supravaginal and vaginal (portio vaginalis) parts |
Layers of the Uterine Wall
| Layer | Structure | Detail |
|---|---|---|
| Perimetrium (Serosa) | Outer peritoneal covering | Covers most of the corpus and posterior cervix |
| Myometrium | Middle smooth muscle layer | 1.5-2.5 cm thick; interlacing smooth muscle bundles; outer fibers continuous with round ligament and fallopian tube |
| Endometrium (Mucosa) | Inner mucous membrane | Columnar gland-forming epithelium with specialized stroma; undergoes cyclic changes; shed as menstruation |
- Berek & Novak's Gynecology, p. 179
Cervix
- Exocervix (portio vaginalis): Convex surface protruding into the vagina; covered by stratified squamous epithelium; the external os opens into the endocervical canal
- Endocervical canal: ~2-3 cm long; lined by mucus-secreting columnar epithelium; opens superiorly into the endometrial cavity at the internal os
- Squamocolumnar junction (Transformation Zone): The dynamic interface between squamous and columnar epithelium - the most vulnerable site for squamous neoplasia
- Composition: Deep stroma is fibrous connective tissue with a small amount of smooth muscle in a circular arrangement
Part 2 - Ligaments of the Uterus
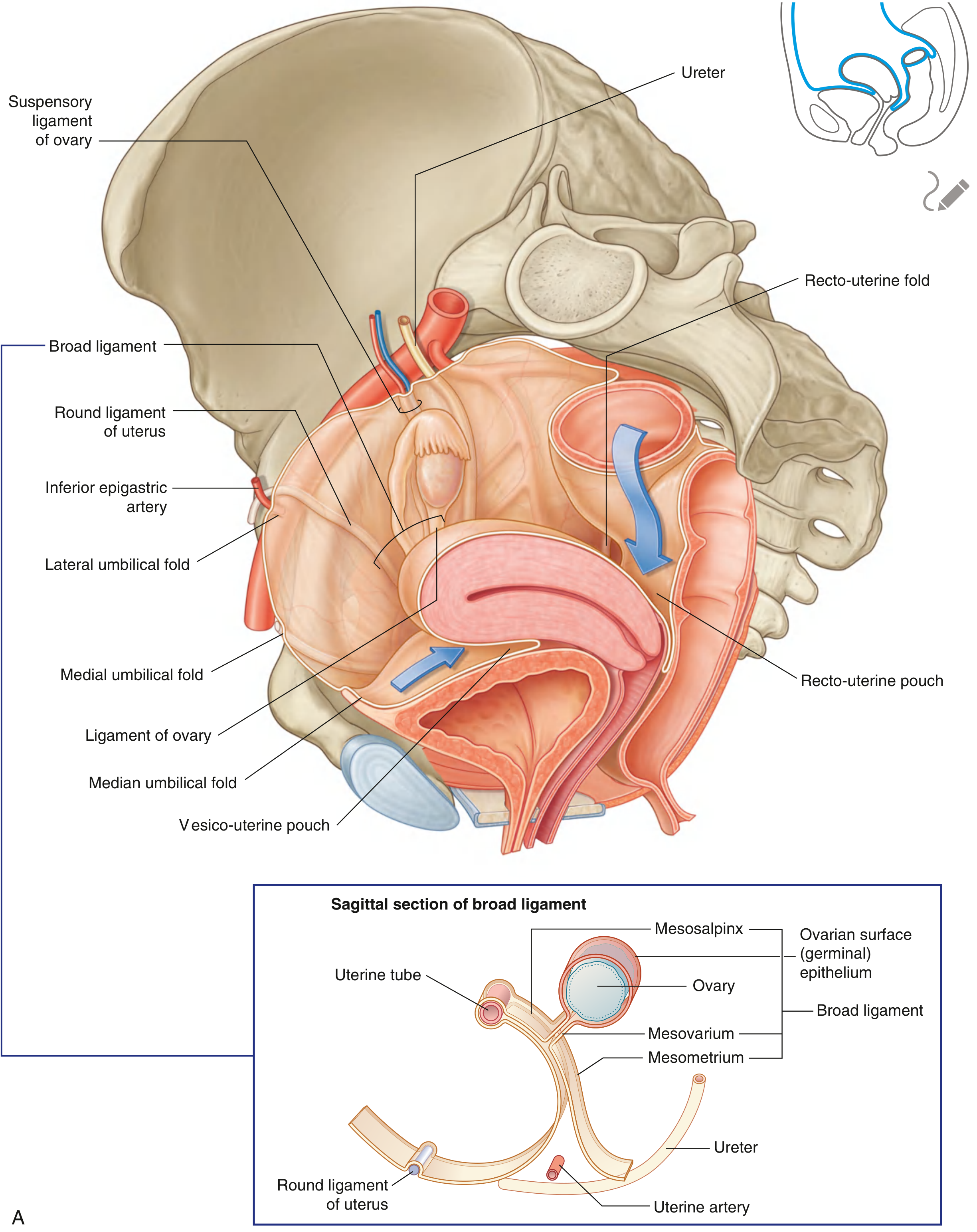
Uterus with Broad Ligament and Adnexa (Posterior View)
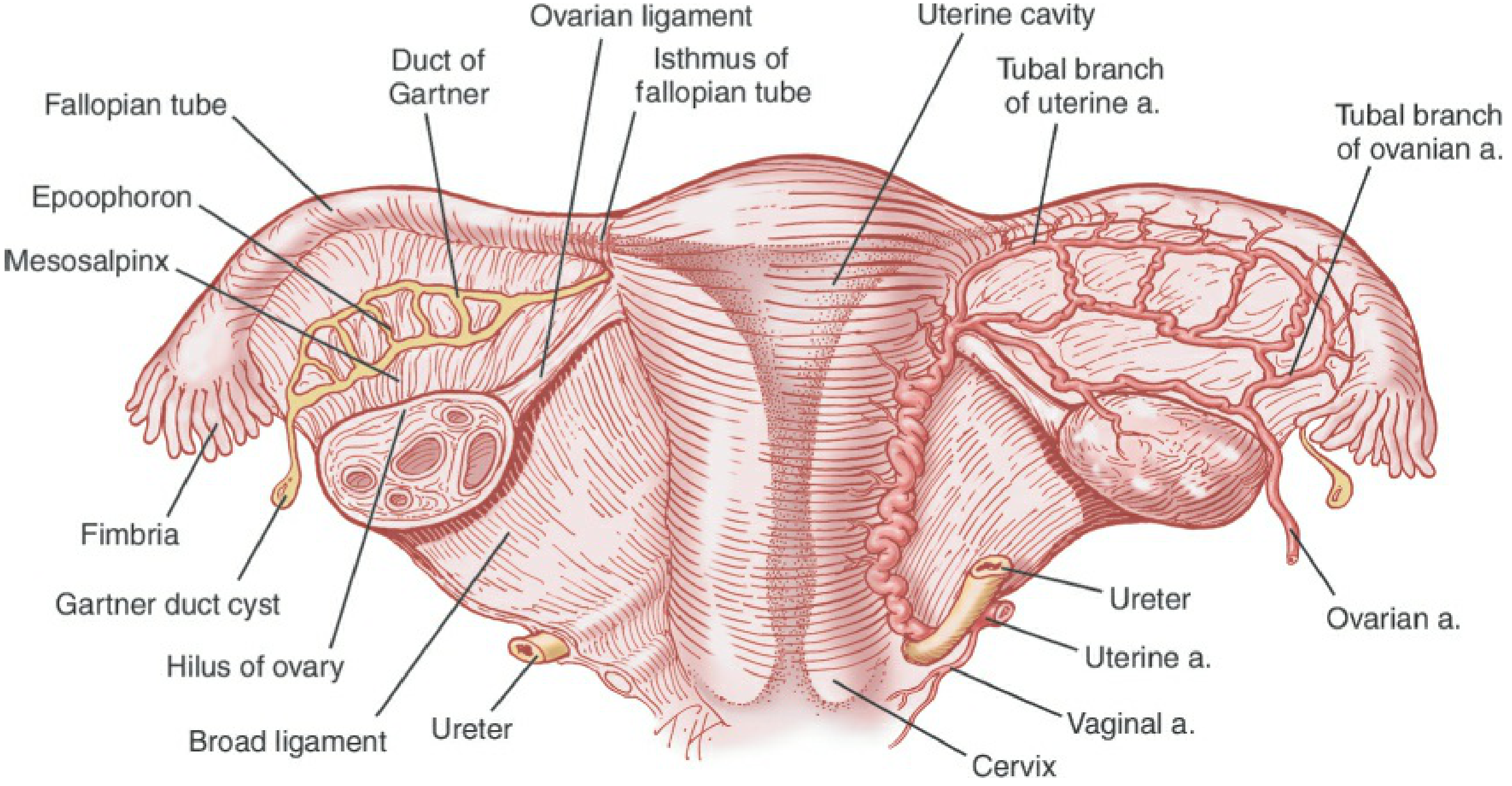
A. Peritoneal Folds (Broad Ligament Complex)
| Part | Location | Contents |
|---|---|---|
| Mesometrium | Largest part; from lateral pelvic wall to the body of uterus | Uterine artery, uterine veins, ureter at its base |
| Mesosalpinx | Most superior free margin | Encloses the uterine (fallopian) tube |
| Mesovarium | Posterior extension | Attaches to the ovary; peritoneum is continuous with the ovarian surface epithelium |
- Gray's Anatomy for Students, pp. 560-561
B. Fascial Condensations (True Supporting Ligaments)
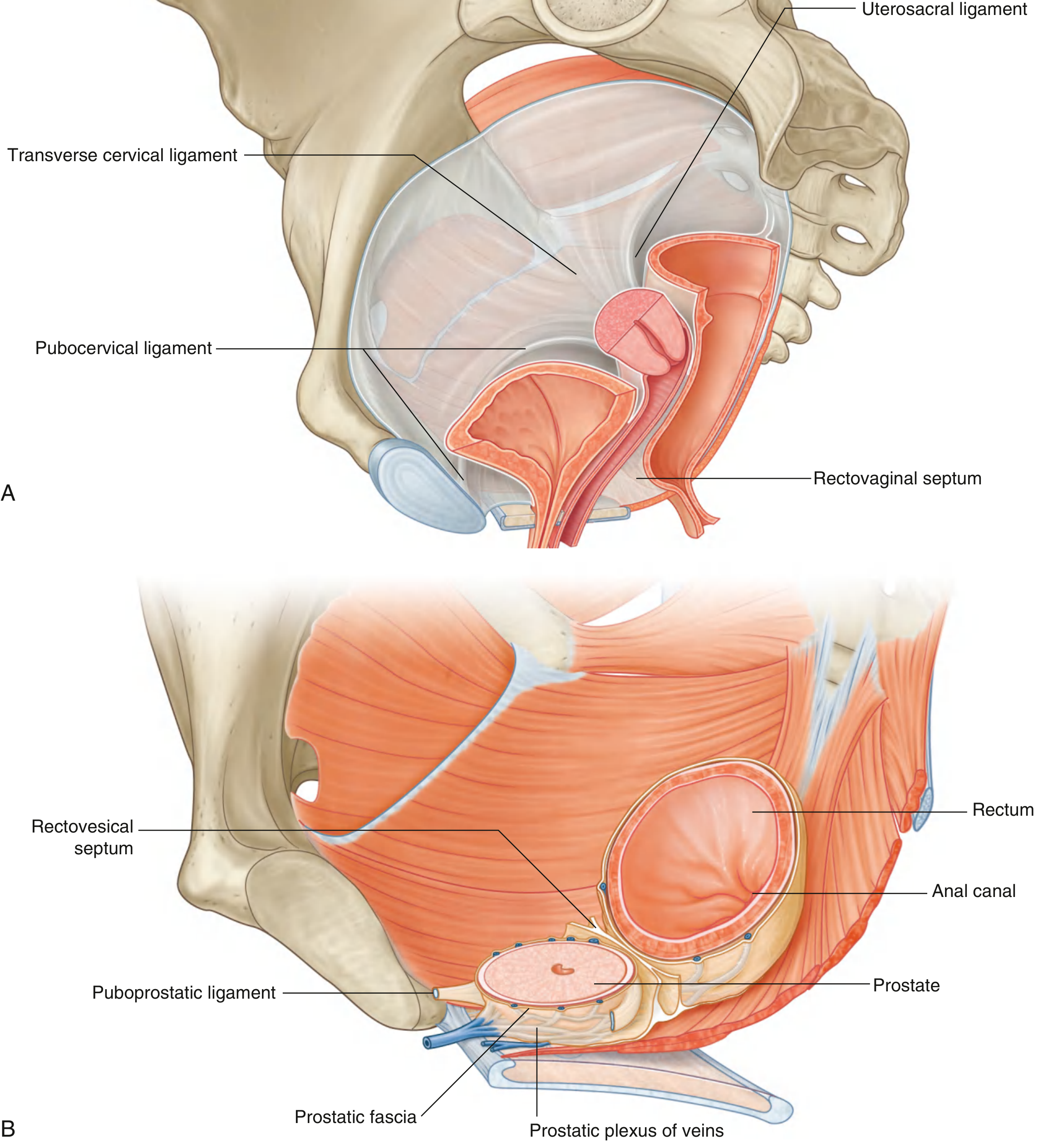
| Ligament | Origin | Insertion | Function |
|---|---|---|---|
| Transverse Cervical (Cardinal) Ligament - Mackenrodt's ligament | Cervix and vaginal vault | Lateral pelvic wall | Most important support; primary resistance against uterine prolapse |
| Uterosacral Ligament | Posterior cervix | Posterolateral pelvic wall / sacrum (S2-S4) | Pulls cervix posteriorly; maintains anteverted position; contains sympathetic nerve fibers |
| Pubocervical Ligament | Anterior cervix | Posterior surface of pubic symphysis | Supports anterior cervix and base of bladder |
The recto-uterine folds of peritoneum overlie the uterosacral ligaments and form the lateral margins of the pouch of Douglas.
- Gray's Anatomy for Students, pp. 558-559
Part 3 - Placement of the Uterus in the Pelvic Floor
Sagittal View - Uterus in the Pelvis
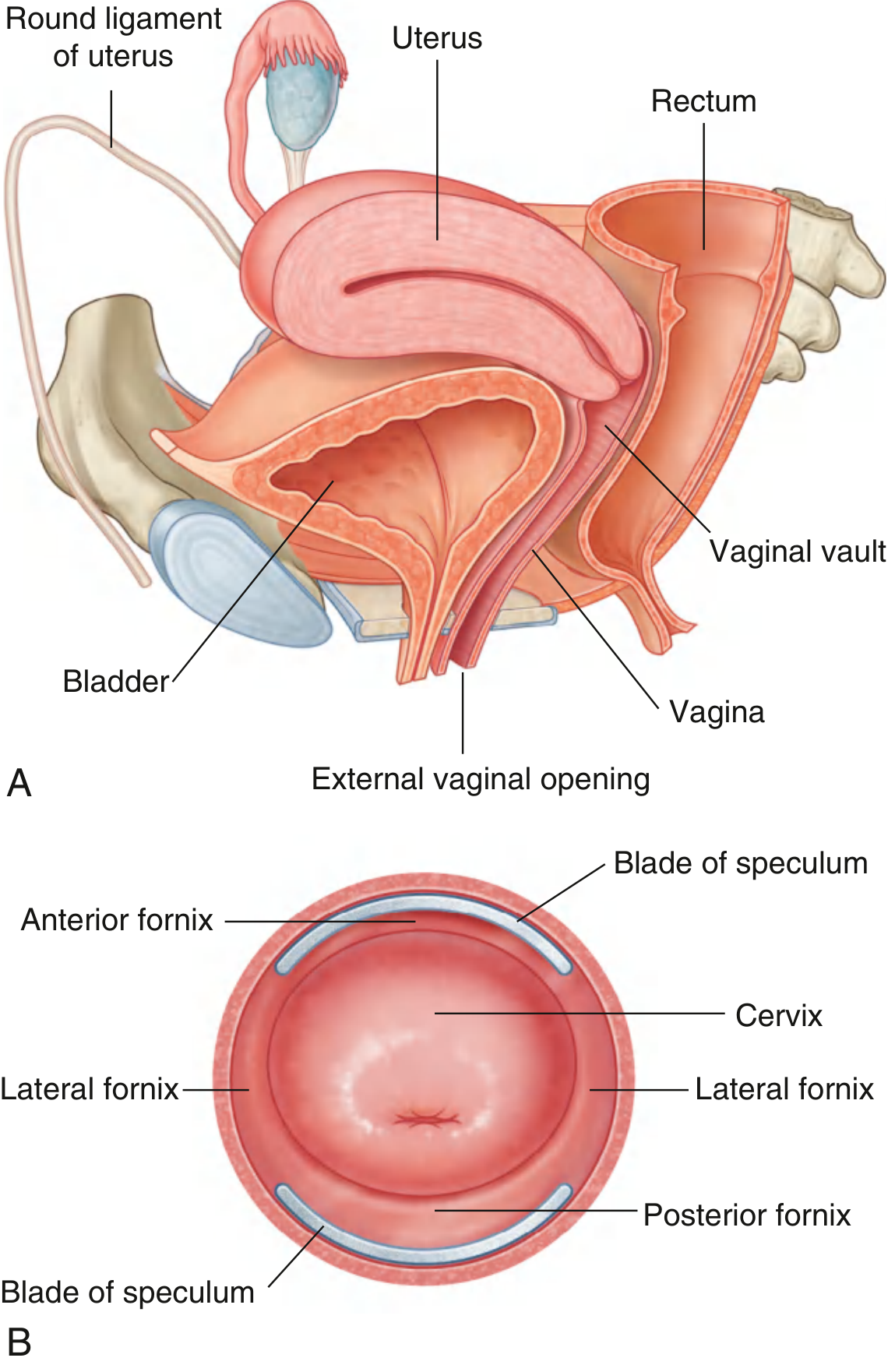
Position and Orientation
- Version = the angle between the long axis of the uterus and the vagina. Normally the uterus is anteverted (tilts forward over the bladder, at ~90° to the vagina)
- Flexion = the angle between the long axis of the uterine corpus and the cervix. Normally the corpus is anteflexed (bends forward on itself, creating an angle of ~170°)
| Structural Relationship | Detail |
|---|---|
| Anterior | Urinary bladder (vesico-uterine pouch separates them) |
| Posterior | Rectum (recto-uterine pouch / Pouch of Douglas lies between) |
| Below | Levator ani muscle (pelvic diaphragm); vagina connects cervix to perineum |
| Lateral | Broad ligaments, ureters, uterine vessels |
| Above | Free peritoneal cavity; fallopian tubes project laterally to the ovaries |
Peritoneal Pouches Around the Uterus
Pelvic Floor Support - Diagram
Supports of the Uterus - Summary
- Pelvic diaphragm (Levator ani + coccygeus) - the muscular floor; provides the primary support platform for all pelvic viscera
- Cardinal (transverse cervical) ligaments - the most important fascial anchors; prevent lateral and downward displacement
- Uterosacral ligaments - pull the cervix posteriorly and superiorly, maintaining anteversion
- Round ligaments - contribute to anteverted position (but are relatively weak supports)
- Pubocervical ligaments - support the anterior cervix and base of bladder
- Perineal body + perineal membrane - further inferior support
Quick Clinical Pearls
- The ureter passes 1.5 cm lateral to the cervix, under the uterine artery at the base of the broad ligament - it must be identified during hysterectomy to avoid iatrogenic injury
- The Pouch of Douglas is the preferred site for drainage of pelvic abscesses or sampling of pelvic fluid (culdocentesis)
- Uterosacral nerve ablation (used in treatment of central pelvic pain/dysmenorrhea) targets the sympathetic fibers running within these ligaments
- Variations in uterine position (retroversion, retroflexion) are generally normal variants unless fixed by adhesions (e.g., endometriosis)
Supports of the uterus - diagram
Detailed medical anatomy diagram showing all supports of the uterus, coronal and sagittal combined view. Show the uterus in the center with clearly labeled supporting structures: 1) Cardinal ligament (Mackenrodt's ligament) - extending laterally from cervix to pelvic sidewall, 2) Uterosacral ligaments - extending posteriorly from cervix to sacrum, 3) Pubocervical ligaments - extending anteriorly from cervix to pubic symphysis, 4) Round ligaments - extending from uterine cornua through inguinal canal to labia majora, 5) Broad ligament - peritoneal folds on each side, 6) Levator ani muscle (pelvic diaphragm) - muscular floor below, 7) Perineal body - inferior support. Include the bladder anteriorly and rectum posteriorly for orientation. Use color coding: red for fascial ligaments, blue for peritoneal folds, green for muscles. All structures clearly labeled with leader lines. Medical textbook illustration style, clean white background, highly detailed and accurate.
Create a clinical presentation on uterine prolapse and pelvic floor dysfunction