Young syndrome
Reading File
Finding Sources
Searching PubMed
Young syndrome azoospermia sinusitis
Searching the Web
Young syndrome clinical features pathophysiology management 2024
Reading File
Reading File
Reading File
I now have thorough information from multiple textbooks. Here is the full answer:
Young Syndrome
Definition
Young syndrome is a rare condition described in the 1970s characterized by a classic clinical triad:
- Chronic sinusitis
- Bronchiectasis
- Obstructive azoospermia (with normal spermatogenesis)
It is seen exclusively in males, because the definition includes azoospermia.
Etiology and Pathophysiology
The exact cause is unknown. Two main hypotheses exist:
- Mercury poisoning - The incidence of Young syndrome has declined dramatically since the 1970s, coinciding with the ban on mercurous chloride (calomel), which was used in teething powders and anthelmintics. This temporal relationship strongly supports mercury exposure as a key etiologic factor.
- Abnormal ciliary function or mucus quality - Ciliary beat frequency and ultrastructural anatomy are generally normal (unlike primary ciliary dyskinesia/Kartagener syndrome), but mucociliary clearance is prolonged nearly threefold compared to controls. In at least one case, ~13% of epididymal cilia showed microtubular disarrangement (malformation of radial spokes and dynein arms). Abnormally thick, viscous secretions are produced.
Some older cases diagnosed as Young syndrome may actually have been undetected cystic fibrosis (CF) or CFTR mutations - with more comprehensive CFTR testing now available, this overlap is being clarified.
Comparison with Similar Conditions
| Feature | Young Syndrome | Cystic Fibrosis | Kartagener / PCD |
|---|---|---|---|
| Bronchiectasis | Yes | Yes | Yes |
| Sinusitis | Yes | Yes | Yes |
| Azoospermia | Obstructive (epididymal) | Obstructive (absent vas deferens) | Yes (immotile sperm) |
| Site of obstruction | Distal epididymis | Congenital absence of vas deferens | Sperm flagellar dysfunction |
| Spermatogenesis | Normal | Normal | Normal |
| Sweat chloride | Normal | Elevated | Normal |
| GI symptoms | Absent | Present (pancreatic insufficiency) | Absent |
| Cilia ultrastructure | Normal (mostly) | Normal | Abnormal (absent dynein arms) |
| Situs inversus | No | No | ~50% |
| Genetics | Unknown | CFTR mutations | Autosomal recessive |
Clinical Presentation
- Recurrent sinopulmonary infections beginning in childhood or early adulthood
- Chronic productive cough
- Bronchiectasis on imaging
- Male infertility (presenting complaint in many cases)
- Normal testicular size and normal serum FSH (indicating intact spermatogenesis)
- Palpable vas deferens and epididymides bilaterally (unlike CF/CBAVD)
- Mild respiratory symptoms compared to CF; no GI involvement
Diagnosis
Young syndrome is a clinical/exclusionary diagnosis. There is no specific laboratory test. The diagnosis requires:
- Recurrent sinopulmonary infections (sinusitis, bronchiectasis)
- Persistent azoospermia with normal spermatogenesis (confirmed by testicular biopsy or normal FSH/testicular size)
- Obstruction at the epididymis on examination
- Exclusion of CF (normal sweat chloride, no CFTR mutations)
- Exclusion of immotile cilia syndrome / PCD (normal ciliary ultrastructure on EM, normal sperm motility in other contexts)
Classification
Young syndrome is classified under CF variants in respiratory medicine, alongside classic CF and alpha-1-antitrypsin deficiency, as a cause of bronchiectasis. In urology, it is listed under posttesticular, congenital, reproductive tract obstruction as a cause of male infertility.
Management
There is no cure. Treatment is symptomatic and individualized, drawing heavily from CF management protocols:
- Antibiotics for acute bacterial sinopulmonary infections
- Inhaled bronchodilators (e.g., albuterol) and hypertonic saline to loosen airway secretions
- Airway clearance physiotherapy
- Surgical reconstruction (vasoepididymostomy) for fertility - however, success rates are lower than for other obstructive conditions
- Assisted reproduction - surgical sperm retrieval (e.g., MESA, TESE) combined with ICSI can achieve fatherhood
Key Points to Remember
- Triad: sinusitis + bronchiectasis + obstructive azoospermia
- Normal sweat test and pancreatic function (unlike CF)
- Normal ciliary ultrastructure (unlike Kartagener syndrome)
- Obstruction is at the epididymis, not the vas deferens
- Declining incidence since mercury-containing teething powders were banned
- Men with this triad should be tested for CFTR mutations before a definitive Young syndrome label is applied
Sources: Smith and Tanagho's General Urology, 19th Ed.; Murray & Nadel's Textbook of Respiratory Medicine; The Washington Manual of Medical Therapeutics; Histology: A Text and Atlas (Pawlina); Medical Physiology (Boron & Boulpaep)
Give me the list of ciliary dyskinesia syndrome where you will have situs inversus asplenia
Finding Sources
Finding Sources
Searching the Web
ciliary dyskinesia situs inversus asplenia heterotaxy right isomerism syndrome list
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
I now have enough to give a thorough, precise answer. Let me compile this clearly.
Ciliary Dyskinesia Syndromes with Situs Inversus / Asplenia
First, an important conceptual clarification is needed here, because situs inversus and asplenia are actually two different laterality outcomes, and they belong to distinct ends of the ciliary dyskinesia spectrum.
The Underlying Mechanism
Nodal cilia (located on the ventral surface of the primitive node in the embryo) use a 9+0 microtubule pattern and establish left-right body asymmetry during early development. When these cilia are dysfunctional:
- The L-R signal is randomized → producing situs inversus (mirror image) in ~50% of cases
- The L-R signal is absent or chaotic → producing situs ambiguus / heterotaxy, which is when asplenia appears
The Syndromes
1. Kartagener Syndrome (Classic)
- Part of Primary Ciliary Dyskinesia (PCD)
- Triad: Situs inversus totalis + bronchiectasis + chronic sinusitis
- Spleen is present and normal (just on the wrong side, mirrored)
- ~50% of PCD patients develop situs inversus totalis (random chance from dysfunctional nodal cilia)
- Absent dynein arms on electron microscopy
- No asplenia
2. Heterotaxy Syndrome (Situs Ambiguus) - Right Isomerism = Asplenia Syndrome
- Also known as Ivemark syndrome (Ivemark sequence)
- Results from failure to establish the L-R axis (bilateral right-sidedness)
- Features:
- Asplenia (or hypoplastic spleen) - because the spleen is a left-sided organ; bilateral right-sidedness means no spleen develops
- Bilateral right-sided (trilobed) lungs and eparterial bronchi
- Complex congenital heart defects (single ventricle, AV canal, anomalous pulmonary venous return, transposition)
- Liver midline or right-sided
- Intestinal malrotation
- Dextrocardia (but NOT situs inversus totalis - incomplete/ambiguous)
- ~9-12% of PCD patients develop heterotaxy/situs ambiguus
- The spleen absence predisposes to fulminant infections by encapsulated bacteria (Streptococcus pneumoniae, Haemophilus, Neisseria)
3. Heterotaxy Syndrome - Left Isomerism = Polysplenia Syndrome
- Bilateral left-sidedness
- Polysplenia (multiple small spleens, may be functionally inadequate)
- Bilateral bilobed lungs
- IVC interruption with azygos continuation
- Complex heart defects (less severe than right isomerism)
- No asplenia
Summary Table
| Syndrome | Laterality | Spleen | Lungs | Key Cilia Defect |
|---|---|---|---|---|
| Kartagener syndrome (PCD) | Situs inversus totalis | Normal, mirrored | Mirrored | Absent dynein arms; randomized L-R axis |
| Right isomerism / Ivemark / Asplenia syndrome | Situs ambiguus | Absent (asplenia) | Bilateral trilobed | Nodal cilia fail to establish L-R axis |
| Left isomerism / Polysplenia syndrome | Situs ambiguus | Multiple small spleens | Bilateral bilobed | Nodal cilia fail to establish L-R axis |
| Young syndrome | Normal | Normal | Bronchiectasis only | Radial spoke + dynein arm malformation (no laterality defect) |
Key Takeaway
The specific ciliary dyskinesia syndrome with situs inversus + asplenia is:
Ivemark syndrome (Right Isomerism / Asplenia Heterotaxy) - a form of PCD/heterotaxy where nodal cilia fail to generate directional flow, resulting in bilateral right-sidedness, absence of the spleen, complex heart defects, and ambiguous organ positioning.
Classic Kartagener syndrome has situs inversus but the spleen is intact. The asplenia combination specifically points to right isomerism / Ivemark syndrome.
Sources: Langman's Medical Embryology; Harrison's Principles of Internal Medicine 22E; The Developing Human (Moore & Persaud); Histology: A Text and Atlas (Pawlina); Emery's Elements of Medical Genetics; Grainger & Allison's Diagnostic Radiology
Give me treatment of Kawasaki disease
Reading File
Finding Sources
Searching PubMed
"Kawasaki disease" treatment IVIG aspirin
Searching the Web
Kawasaki disease treatment guidelines 2024 IVIG aspirin corticosteroids
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive data from textbooks and the 2024 AHA update. Here is the full treatment guide:
Treatment of Kawasaki Disease
The primary goal of treatment is to reduce coronary artery inflammation and prevent coronary artery aneurysms (CAA), which occur in 20-25% of untreated children. Treatment must be initiated within the first 10 days of fever whenever possible.
1. Acute Phase Treatment (All Patients)
A. IVIG (Intravenous Immunoglobulin) - FIRST-LINE
- Dose: 2 g/kg as a single infusion over 10-12 hours
- Timing: Must be given within the first 10 days of illness (ideally days 5-9)
- Reduces coronary artery dilation risk from ~20-25% down to <3%
- Reduces incidence of coronary artery aneurysms fivefold vs aspirin alone
- Can still be given after day 10 if ESR/CRP remain elevated with persistent fever
- Treatment with IVIG + aspirin reduces CAA prevalence from ~25% (aspirin alone) to ~5%
B. Aspirin - GIVEN ALONGSIDE IVIG
Two dosing strategies exist (both acceptable - no superiority proven):
| Phase | US Standard Dose | Alternative (Many Centers) |
|---|---|---|
| Acute (febrile) | High dose: 80-100 mg/kg/day in 4 divided doses | Moderate dose: 30-50 mg/kg/day |
| Duration of high/moderate dose | Until 48-72 hours after defervescence | Until afebrile |
| Maintenance (subacute/convalescent) | Low dose: 3-5 mg/kg/day as single daily dose | Same |
| Duration of low dose | 6-8 weeks, or until platelet count and ESR normalize (if no CAA) | Indefinitely if CAA persists |
Note: Ibuprofen antagonizes the antiplatelet effect of aspirin and should be avoided. Use acetaminophen for fever instead.
2. High-Risk Patients - Adjunctive Therapy (2024 AHA Update)
Patients at high risk for IVIG resistance or CAA development should receive intensified primary therapy alongside IVIG + aspirin:
High-risk criteria include:
- Age ≤ 6 months
- Baseline coronary artery z-score ≥ 2.5 on echocardiogram
Adjunctive Options:
| Agent | Dose | Notes |
|---|---|---|
| Corticosteroids (methylprednisolone/prednisolone) | IV methylprednisolone 2 mg/kg/day | First-line adjunct for high-risk; reduces CAA z-score significantly; shown to suppress monocyte-mediated inflammation more than IVIG alone |
| Infliximab (anti-TNF-α) | 10 mg/kg IV over 2 hours | Alternative to steroids; screen for Hepatitis B and TB first; evidence from KIDCARE trial |
| Anakinra (IL-1 receptor antagonist) | Limited data | Emerging option; recent 2026 systematic review supports use in selected refractory cases |
| Cyclosporine | Limited data | Option for highly refractory cases |
The 2024 AHA statement notes that which specific adjunct is chosen matters less than ensuring one is used in high-risk patients, as both corticosteroids and infliximab reduce CAA progression compared to IVIG alone.
3. IVIG Resistance (Refractory Kawasaki Disease)
Defined as: persistence or recrudescence of fever ≥36 hours after completion of initial IVIG infusion (affects ~10% of patients)
Step-wise approach:
- Second dose of IVIG - 2 g/kg (first-line re-treatment)
- Corticosteroids - IV methylprednisolone if second IVIG fails
- Infliximab - 5-10 mg/kg IV (from KIDCARE trial data)
- Non-glucocorticoid immunosuppressives (cyclosporine, anakinra) - for persistent fever despite above
4. Antithrombotic / Long-Term Therapy by Coronary Artery Status
| Risk Level | Coronary Status | Long-Term Therapy | Follow-Up |
|---|---|---|---|
| I | No coronary changes | None beyond 6-8 weeks | Cardiovascular risk counseling every 5 years |
| II | Transient ectasia, resolved by 8 weeks | None beyond 6-8 weeks | Cardiovascular risk counseling every 3-5 years |
| III | Small-medium solitary aneurysm | Aspirin 3-5 mg/kg/day until aneurysm resolves | Annual echo + ECG |
| IV | Large (>6 mm) or multiple aneurysms, no obstruction | Aspirin 3-5 mg/kg/day + warfarin or LMWH for giant aneurysms | Echo/ECG every 6 months; cardiac cath at 6-12 months |
| V | Coronary artery obstruction | Aspirin + warfarin/LMWH + beta-blockers (reduce myocardial work) | Echo/ECG every 6 months; cardiac cath; guided stress testing |
5. Echocardiographic Follow-Up (All Patients)
- At diagnosis (baseline)
- At 2 weeks
- At 6-8 weeks
- At 12 months (optional if normal)
- More frequent if CAA or elevated z-scores present
A higher baseline coronary artery z-score is strongly associated with worse cardiac outcomes.
6. Other Considerations
- Influenza vaccine: All children ≥6 months should receive inactivated (not live) influenza vaccine before discharge (and family members) - mandatory while on aspirin therapy to reduce Reye syndrome risk
- Live vaccines (MMR, varicella): Defer for 11 months after IVIG (may blunt immune response)
- Incomplete Kawasaki disease: Treat with IVIG promptly at diagnosis - do NOT delay until day 10
Sources: The Harriet Lane Handbook 23rd Ed. (Johns Hopkins); Rosen's Emergency Medicine; Fitzpatrick's Dermatology; AHA 2024 Scientific Statement Update on Kawasaki Disease; ACR/Vasculitis Foundation 2021 Guidelines; UC Davis Health Protocol December 2024
Generate this in form of image
Generating Image
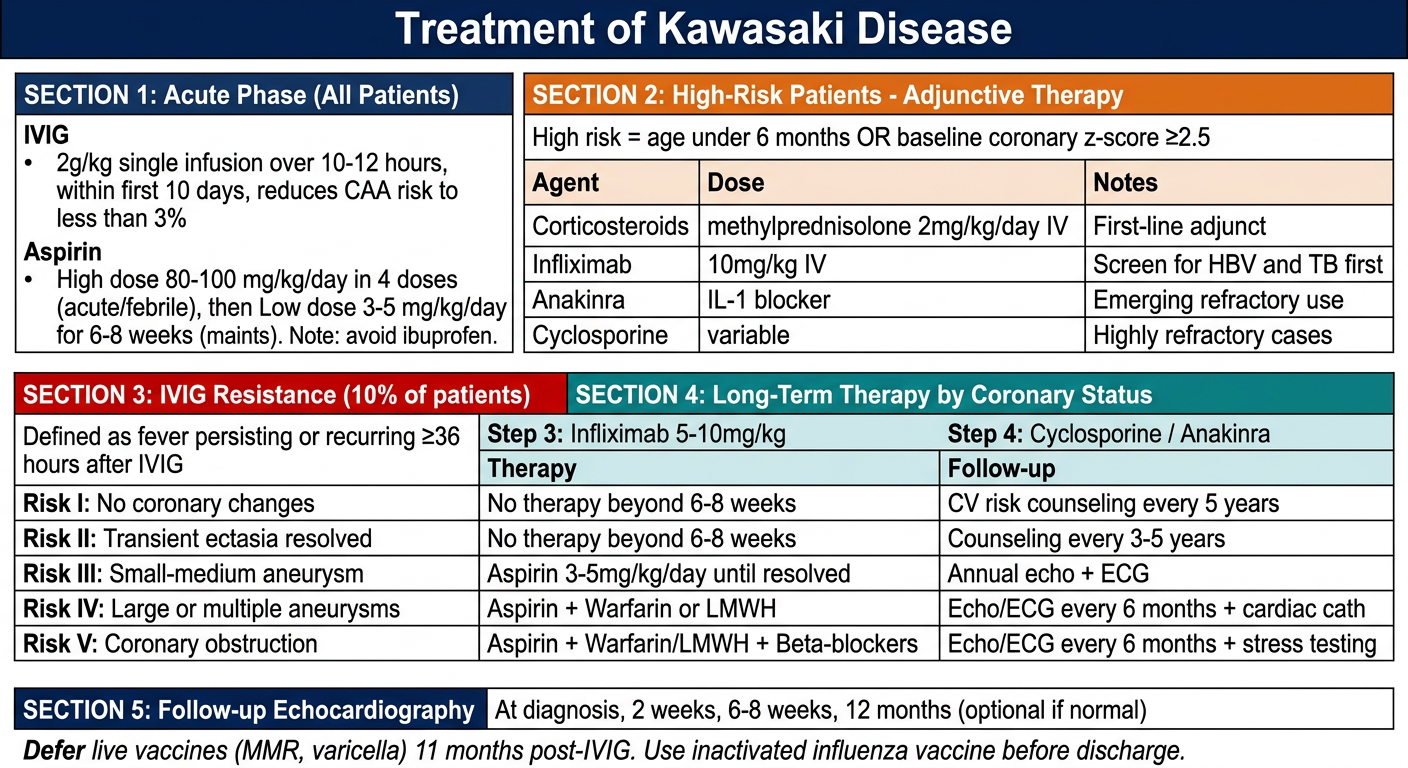
Here is the full Kawasaki Disease treatment summary as a clinical reference image, covering all five sections: acute management, high-risk adjunctive therapy, IVIG resistance protocol, long-term coronary risk stratification, and echocardiographic follow-up. Let me know if you'd like any section expanded or reformatted.
This is a shared conversation. Sign in to Orris to start your own chat.