Volume of distribution and 3 compartment model
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough explanation of both topics, drawn from Barash's Clinical Anesthesia, Miller's Anesthesia, and Katzung's Basic and Clinical Pharmacology.
Volume of Distribution (Vd)
Definition
The volume of distribution is an apparent (hypothetical) volume that relates the total amount of drug in the body to the drug concentration measured in plasma (or blood):
Vd = Amount of drug in body / Plasma concentration
It is called "apparent" because it does not correspond to any real anatomical space. It is simply a mathematical construct that tells you how extensively a drug distributes into tissues relative to plasma.
- If Vd is small (e.g., ~0.04 L/kg = ~2.8 L): the drug is confined mostly to plasma (e.g., large protein molecules like antibodies).
- If Vd equals total body water (~0.6 L/kg = ~42 L): the drug distributes evenly throughout the body (e.g., ethanol).
- If Vd is very large (e.g., hundreds of liters): the drug has much higher concentrations in peripheral tissues than in plasma - it is being "pulled out" of the plasma into tissues (e.g., digoxin ~500 L, chloroquine ~200-800 L/kg).
Physical Body Compartments vs. Vd
| Compartment | Volume (L/kg) | Example Drugs |
|---|---|---|
| Plasma | 0.04 | Large proteins, antibodies |
| Extracellular water | 0.2 | Gentamicin |
| Total body water | 0.6 | Ethanol |
| Fat | 0.2-0.35 | Diazepam |
| Bone | 0.07 | Lead, fluoride |
Clinical Importance of Vd
- Loading dose calculation:
Loading Dose = Vd × Target Concentration- A higher Vd means a larger loading dose is needed to "fill up" the compartments and reach the target plasma concentration.
- Predicting drug behavior: Lipophilic drugs have large Vd; hydrophilic drugs have small Vd.
- Dosing adjustments: Pathological states (heart failure, obesity, edema, burns, hypoalbuminemia) alter Vd and may require dose changes.
Note: Vd cannot tell you the concentration of drug in any specific tissue - it only summarizes the overall distribution behavior. - Barash's Clinical Anesthesia, p. 747
Compartmental Pharmacokinetic Models
Compartmental models describe the body as a series of interconnected "boxes" (compartments). These are mathematical constructs - they do not map directly onto real organs or tissues.
One-Compartment Model
The simplest model. The entire body behaves as a single well-mixed tank. After IV administration:
- Drug instantly and evenly distributes throughout one volume (Vd).
- Elimination follows first-order kinetics:
C(t) = C₀ × e^(-kt) - Plasma concentration declines as a single exponential curve.
Two-Compartment Model
After IV injection, plasma concentration shows two phases (biexponential decline):
Cp(t) = Ae^(-αt) + Be^(-βt)- α phase (distribution phase): Rapid initial fall in plasma concentration as drug rapidly distributes from the central compartment (V₁ - blood/plasma) into the peripheral/shallow compartment (V₂ - well-perfused tissues like muscle, viscera).
- β phase (elimination phase): Slower decline as drug is eliminated from the central compartment while the peripheral compartment re-equilibrates.
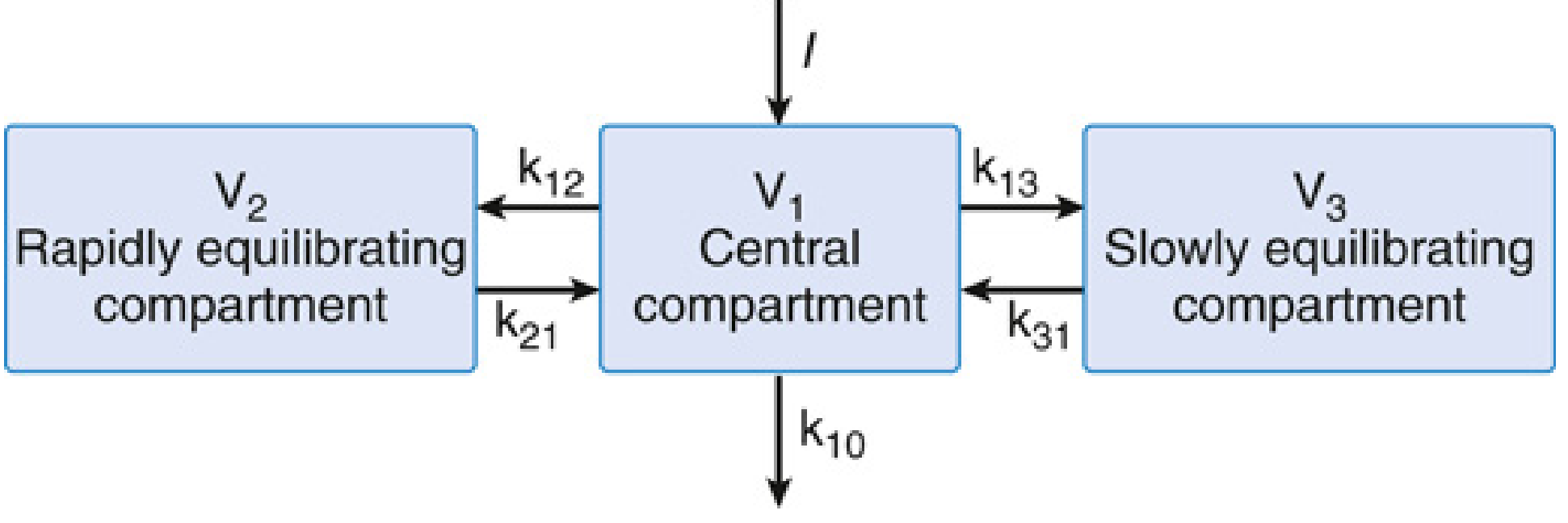
Three-Compartment Model
Many drugs (especially lipophilic anesthetics, opioids) show three distinct phases after IV injection - a triphasic concentration-time curve:
Cp(t) = Ae^(-αt) + Be^(-βt) + Ge^(-γt)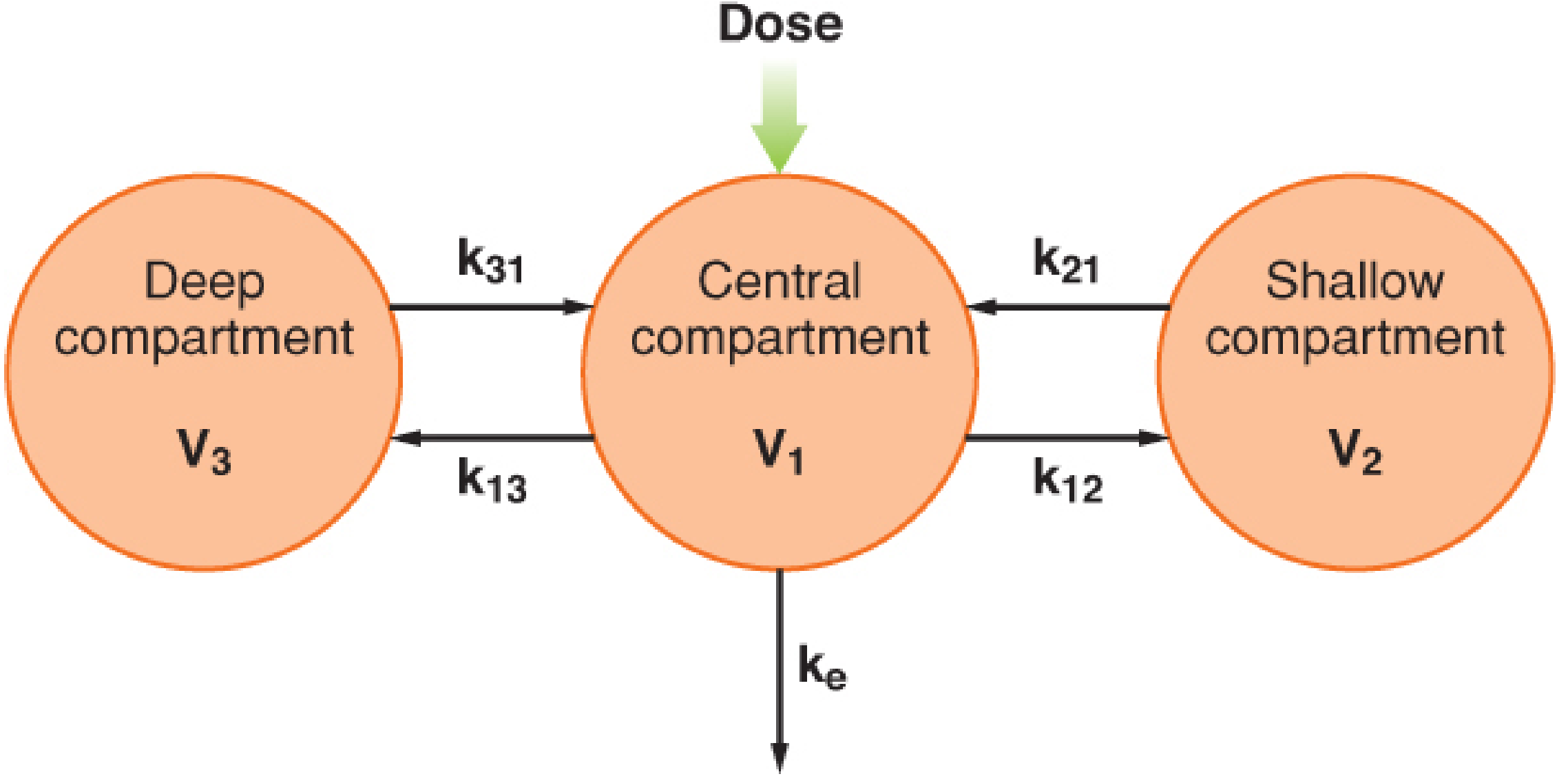
Structure
| Compartment | Volume | Physiological Correlate | Equilibration |
|---|---|---|---|
| Central (V₁) | Smallest | Blood, highly perfused organs (liver, lung, kidneys) | Instantaneous |
| Shallow peripheral (V₂) | Intermediate | Muscle, skin, lean tissues | Rapid (minutes) |
| Deep peripheral (V₃) | Largest | Fat, bone, poorly perfused tissues | Slow (hours) |
Rate Constants
- k₁₂ / k₂₁: Transfer between central (V₁) and shallow peripheral (V₂)
- k₁₃ / k₃₁: Transfer between central (V₁) and deep peripheral (V₃)
- ke (or k₁₀): Irreversible elimination from the central compartment only
The Three Phases Explained
- α phase (rapid distribution): Drug rapidly moves from plasma into the shallow peripheral compartment. Steep, fast initial drop in plasma concentration.
- β phase (slow distribution): Drug slowly moves into the deep peripheral compartment (e.g., fat). Plasma levels continue to fall, but more gradually.
- γ phase (terminal elimination): Drug re-enters the central compartment from peripheral compartments and is eliminated. This is the true half-life.
Steady-State Volume of Distribution
In the three-compartment model:
Vss = V₁ + V₂ + V₃
All three compartmental volumes add up to give the steady-state volume of distribution.
Clinical Examples of Three-Compartment Drugs
- Fentanyl, sufentanil, alfentanil - classic three-compartment opioids; their prolonged effect after infusion ("context-sensitive half-time") is largely explained by drug re-emerging from the deep compartment.
- Propofol - three-compartment kinetics; rapid awakening after bolus is due to redistribution, not elimination.
- Thiopental - highly lipophilic; recovery from a single induction dose is driven by redistribution into muscle and fat (V₂ and V₃).
Key Takeaway: Why It Matters Clinically
| Feature | Clinical Implication |
|---|---|
| Large V₃ (fat) | Drug accumulates with prolonged infusion; slow release causes extended effect after stopping |
| Rapid k₁₂/k₂₁ | Fast onset and offset for short procedures |
| Slow k₁₃/k₃₁ | Context-sensitive half-time increases with infusion duration |
| Vss = V₁ + V₂ + V₃ | Loading dose must account for all compartments |
Sources: - Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, pp. 746-758 - Miller's Anesthesia, 10e, pp. 1698-1720 - Katzung's Basic and Clinical Pharmacology, 16e, pp. 77-78
This is a shared conversation. Sign in to Orris to start your own chat.