Abg
Reading File
Searching the Web
ABG arterial blood gas interpretation 2025 clinical guide
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, textbook-grounded guide to ABG interpretation:
Arterial Blood Gas (ABG) - Complete Interpretation Guide
Normal Reference Values
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaO2 | 80 - 100 mmHg |
| PaCO2 | 35 - 45 mmHg |
| HCO3- | 22 - 26 mEq/L |
| SaO2 | 95 - 100% |
| Base excess | -2 to +2 |
5-Step Systematic Interpretation
Step 1 - Assess the pH
- < 7.35 = Acidemia
- > 7.45 = Alkalemia
- 7.35 - 7.45 = Normal (may still have a compensated disorder)
Step 2 - Identify the primary disorder
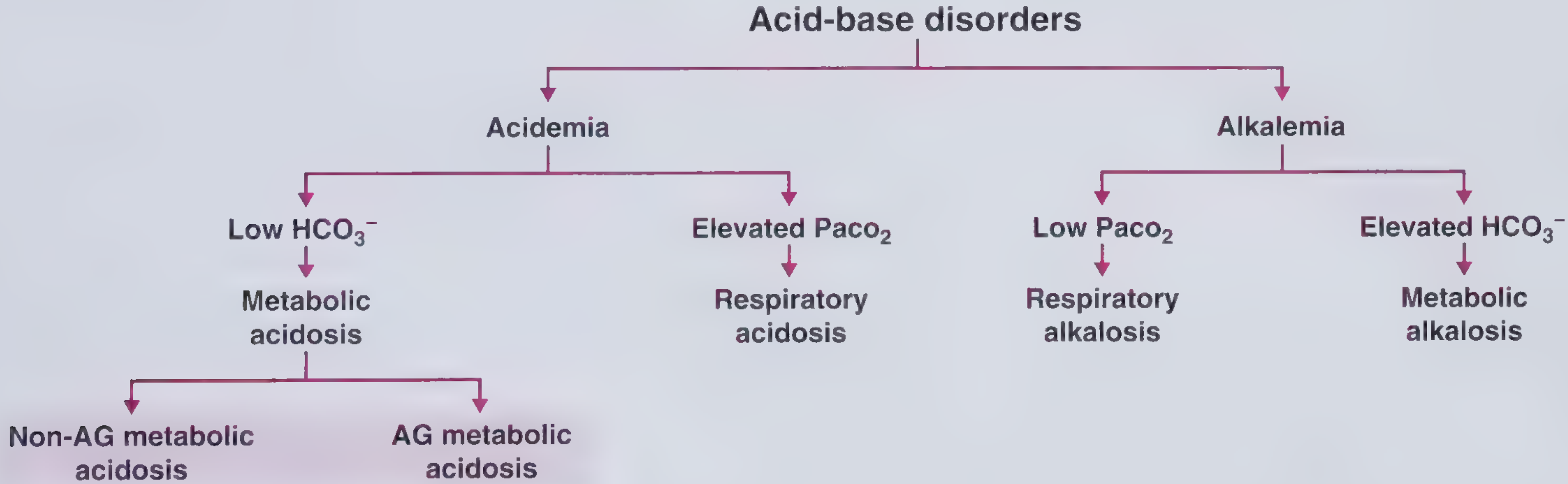
| pH | PaCO2 | HCO3- | Disorder |
|---|---|---|---|
| < 7.35 | > 45 | Normal | Respiratory acidosis |
| < 7.35 | Normal | < 22 | Metabolic acidosis |
| > 7.45 | < 35 | Normal | Respiratory alkalosis |
| > 7.45 | Normal | > 26 | Metabolic alkalosis |
Step 3 - Assess compensation (expected values)
Use the formulas from Henry's Clinical Diagnosis and Management by Laboratory Methods to check if compensation is appropriate:
| Primary Disorder | Compensation Formula |
|---|---|
| Metabolic acidosis | Expected PaCO2 = ΔHCo3- × 1.2 ± 2 (Winter's formula) |
| Metabolic alkalosis | Expected ΔPCO2 = ΔHCO3- × 0.7 ± 5 |
| Acute respiratory acidosis | Expected ΔHCO3- = ΔPaCO2 × 0.07 ± 1.5 |
| Chronic respiratory acidosis | Expected ΔHCO3- = ΔPaCO2 × 0.4 ± 3 |
| Acute respiratory alkalosis | Expected ΔHCO3- = ΔPaCO2 × 0.2 ± 2.5 |
| Chronic respiratory alkalosis | Expected ΔHCO3- = ΔPaCO2 × 0.5 ± 2.5 |
- If compensation is less than expected → mixed disorder (second acidosis present)
- If compensation is greater than expected → second alkalosis present
Step 4 - Calculate the Anion Gap (if metabolic acidosis)
AG = Na+ - (Cl- + HCO3-)
Normal AG: < 12 mEq/L
Correct for hypoalbuminemia: Add 2.5 mEq/L to calculated AG for every 1 g/dL drop in albumin below normal.
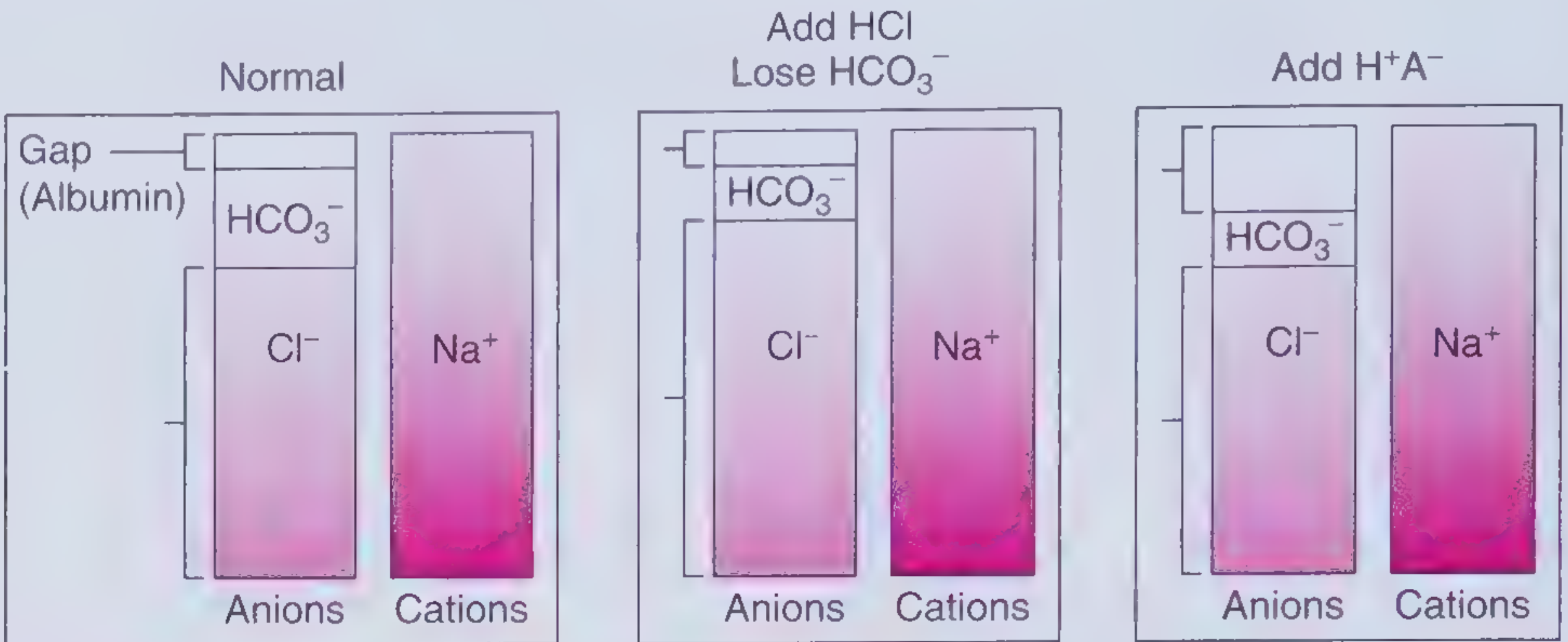
High AG metabolic acidosis (MUDPILES):
- Methanol, Uremia, Diabetic ketoacidosis, Propylene glycol, Isoniazid/Iron, Lactic acidosis, Ethanol, Salicylates
Normal AG (hyperchloremic) metabolic acidosis (HARDUPS):
- Hyperalimentation, Addison's disease, Renal tubular acidosis, Diarrhea, Ureteral diversion, Pancreatic fistula, Saline infusion
Step 5 - Assess oxygenation
- PaO2 < 80 mmHg = Hypoxemia
- Calculate A-a gradient = PAO2 - PaO2
- PAO2 = (FiO2 × 713) - (PaCO2 / 0.8)
- Normal A-a gradient: ~4 mmHg (age-adjusted: Age/4 + 4)
- Widened A-a gradient suggests V/Q mismatch, diffusion impairment, or shunt
- Normal A-a gradient with hypoxia suggests pure hypoventilation
Quick Summary of Disorders
| Disorder | pH | PaCO2 | HCO3- | Common Causes |
|---|---|---|---|---|
| Respiratory acidosis | ↓ | ↑ | ↑ (compensated) | COPD, hypoventilation, sedation |
| Respiratory alkalosis | ↑ | ↓ | ↓ (compensated) | Anxiety, PE, pain, hypoxia |
| Metabolic acidosis | ↓ | ↓ (compensated) | ↓ | DKA, lactic acidosis, renal failure |
| Metabolic alkalosis | ↑ | ↑ (compensated) | ↑ | Vomiting, diuretics, excess alkali |
Key Clinical Pearls
- Arterial blood is the gold standard - venous pH correlates closely (±0.05 units) but venous PO2 cannot assess oxygenation - Tintinalli's Emergency Medicine
- Pulse oximetry cannot detect hypercarbia, especially in patients on supplemental O2. A patient can have significant CO2 retention with a normal SpO2 - Murray & Nadel's Respiratory Medicine
- Compensation is most effective in respiratory alkalosis (pH often normalizes), then respiratory acidosis, then metabolic acidosis. It is least effective in metabolic alkalosis - Henry's Clinical Diagnosis
- Mixed disorders are common in the ICU. Always check if compensation matches the formula; deviation signals a second disorder.
This is a shared conversation. Sign in to Orris to start your own chat.