Draw the diagram of paravertebral space and labelled the structure and discuss anesthesiolical implications
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Searching PubMed
thoracic paravertebral block analgesia
Loading Image
Finding Sources
Generating Image
Here is a comprehensive discussion of the paravertebral space and its anesthesiological implications.
Paravertebral Space - Anatomy & Anesthesiological Implications
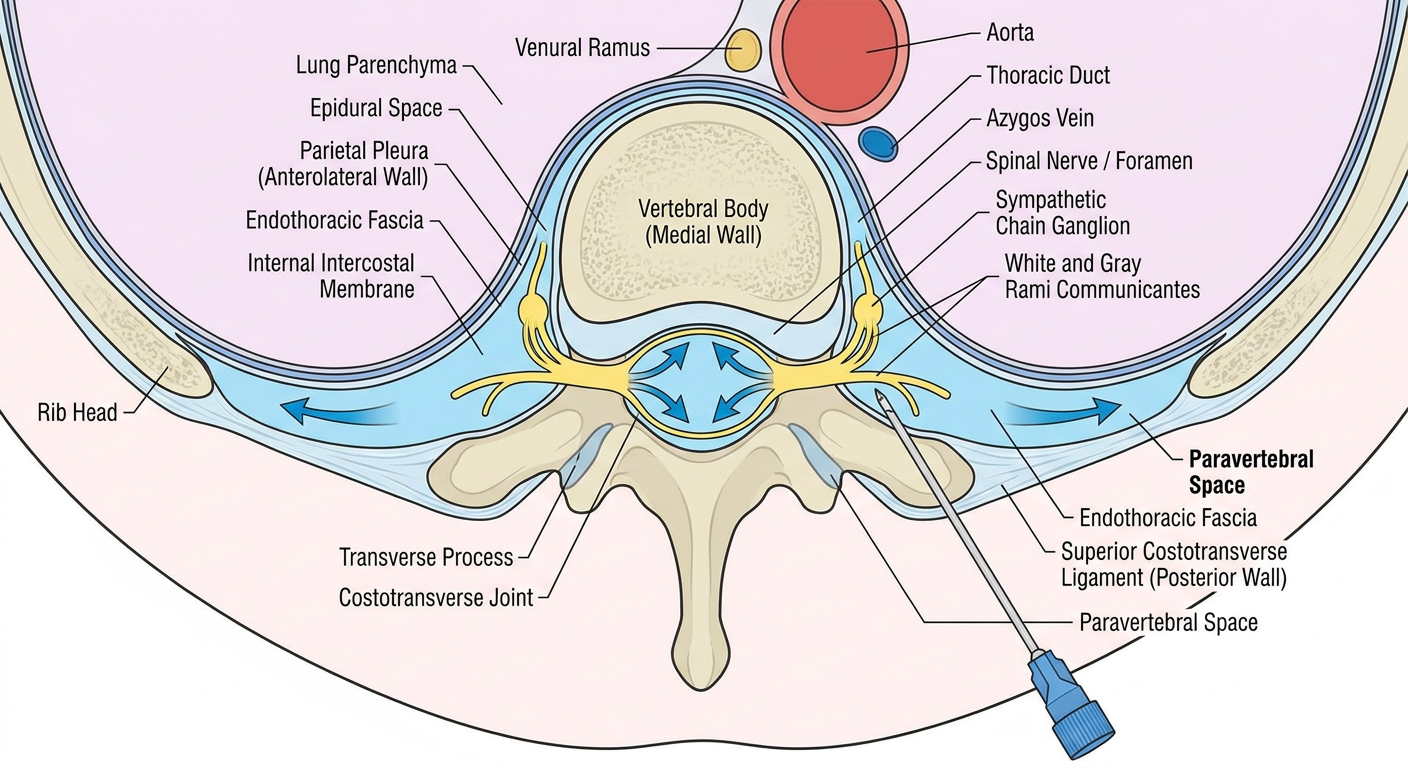
Generated Labeled Diagram
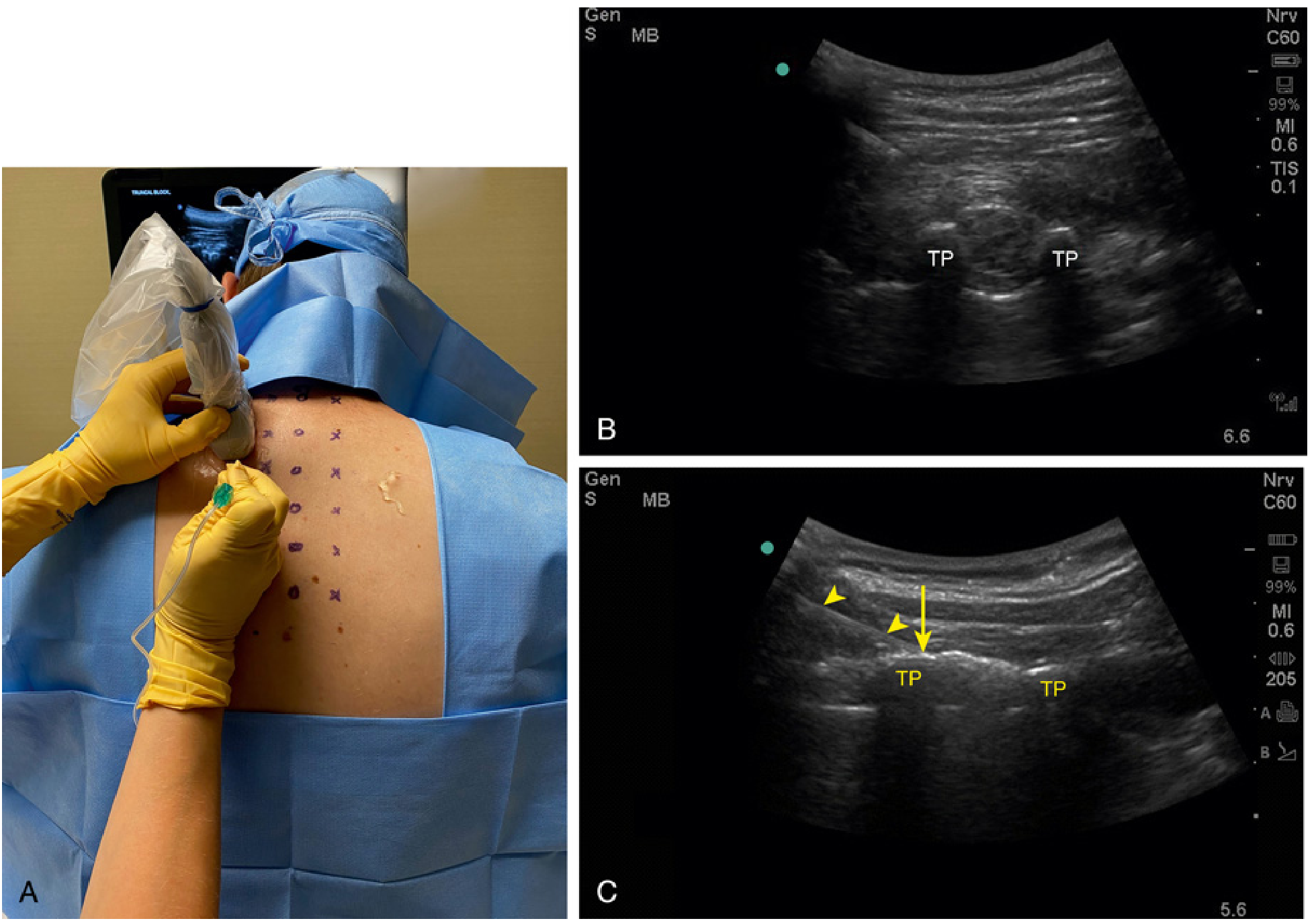
Textbook Ultrasound & Anatomical Images
Ultrasound-guided paravertebral block (Miller's Anesthesia, 10e, Fig. 42.19) - showing the parasagittal approach, transverse processes (TP), superior costotransverse ligament, and the "smile sign" of local anesthetic depressing the parietal pleura:
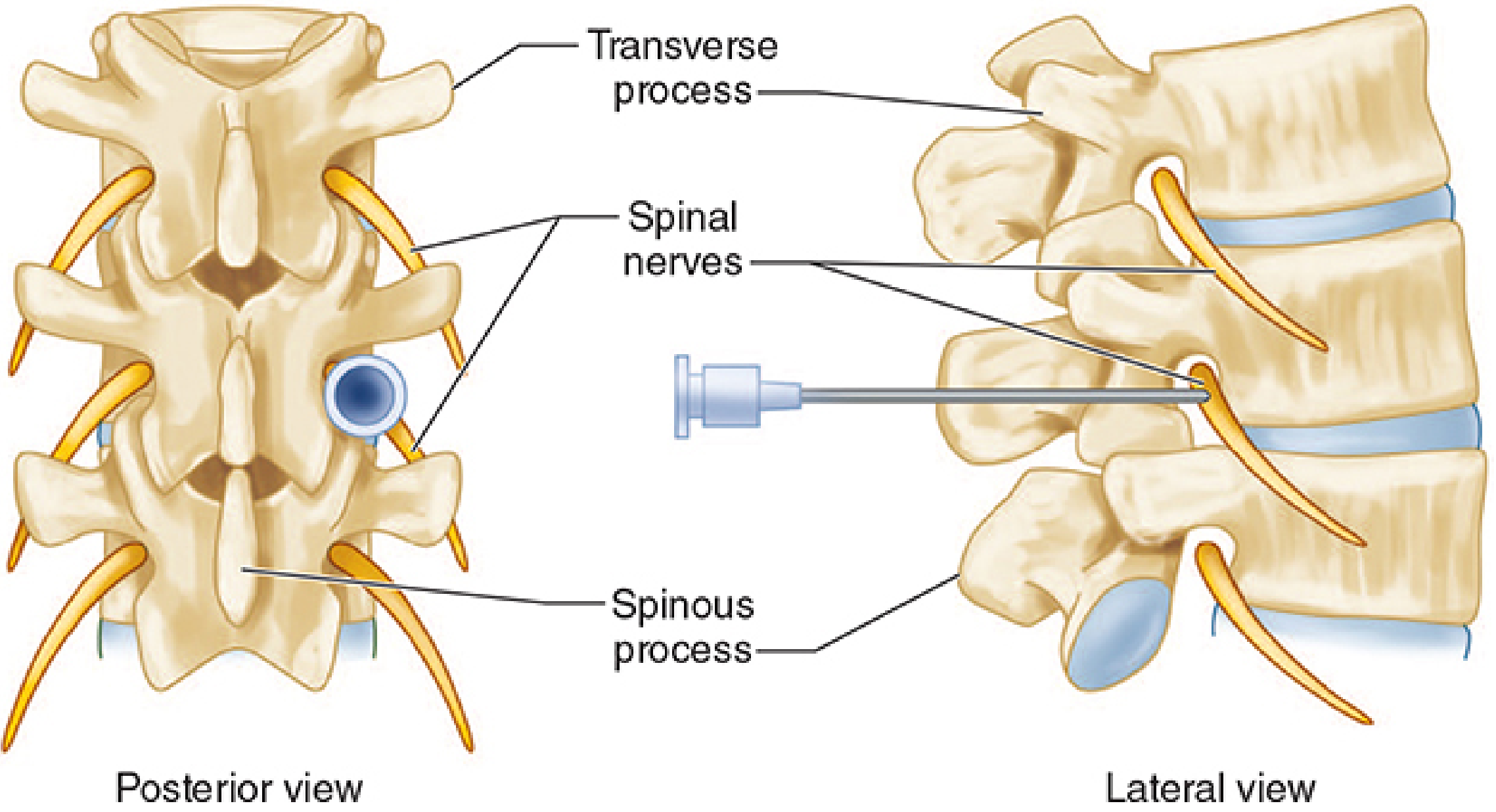
Lumbar paravertebral nerve block - posterior and lateral views (Morgan & Mikhail's, 7e, Fig. 47-14):
1. Anatomy of the Paravertebral Space
The paravertebral space (PVS) is a bilateral, wedge-shaped potential space located on either side of the vertebral column, extending along the entire length of the spine. Its shape makes it ideal for segmental deposition of local anesthetic.
Boundaries (Thoracic Region)
| Wall | Structure |
|---|---|
| Medial | Vertebral body, intervertebral disc, intervertebral foramen, spinous processes |
| Anterolateral | Parietal pleura (in thorax); endothoracic fascia lines this surface |
| Posterior | Superior costotransverse ligament; approximately 2.5 cm from tip of spinous process, often in a slightly caudad orientation |
| Lateral | Posterior intercostal membrane (where space transitions into the intercostal space) |
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, p. 2912
- Miller's Anesthesia, 10e, p. 6254
Key Structures Within the Paravertebral Space
- Spinal nerve - exits the intervertebral foramen within the PVS; quickly divides into:
- Ventral ramus - motor and sensory to the anterior thoracic wall
- Dorsal ramus - sensory to paravertebral muscles and back skin
- Sympathetic chain ganglion - lies close to somatic nerves; coincidental sympathetic block is routinely achieved
- White rami communicantes - preganglionic sympathetic efferents from T1-L2 entering the chain
- Gray rami communicantes - postganglionic fibers returning to the spinal nerve at all levels
- Intercostal nerve (continuation of ventral ramus) at the lateral border
- Endothoracic fascia - lines the inner chest wall, separating it from the parietal pleura
Contiguity with Adjacent Spaces
The PVS does not exist in isolation. It is directly contiguous with:
- The epidural space medially (through the intervertebral foramen) - explaining epidural spread with large volumes
- The intercostal space laterally - explaining dermatomal spread
- The contralateral paravertebral space through the prevertebral fascia - explaining bilateral effects with large volumes
This anatomical continuity is both clinically useful and a source of complications.
2. Anesthesiological Implications
A. Mechanism of Block
A single-level injection of local anesthetic into the PVS anesthetizes:
- The somatic nerve at that level (ventral + dorsal rami)
- The sympathetic chain at that level
- Often 2-3 adjacent dermatomal segments (due to cephalocaudad spread within the PVS)
The resulting block is unilateral somatosensory, motor, and sympathetic - in contrast to epidural which is bilateral.
B. Clinical Indications
| Region | Surgery / Condition |
|---|---|
| Breast | Mastectomy, axillary dissection (T2-T6) |
| Thorax | Thoracotomy, VATS, rib fractures, chest trauma |
| Abdomen | Ventral hernia repair (T7-T11), exploratory laparotomy |
| Inguinal | Herniorrhaphy (T9-T11) |
| Acute pain | Herpes zoster, proximal rib fractures |
| Chronic pain | Thoracic spine-origin pain, post-thoracotomy pain syndrome |
| Hip surgery | Thoracolumbar paravertebral (postoperative analgesia) |
The thoracic PVB is particularly valuable in upper thoracic segments where the scapula physically blocks intercostal nerve access. - Morgan & Mikhail's, 7e, p. 2054
C. Advantages Over Other Techniques
| Feature | PVB | Epidural | Intercostal |
|---|---|---|---|
| Bilateral block | No (usually) | Yes | No |
| Sympathetic block | Unilateral | Bilateral | Minimal |
| Hemodynamic instability | Less | More | Minimal |
| Urinary retention | Rare | Common | No |
| Opioid-sparing | Yes | Yes | Partial |
| Anticoagulation risk | Lower | Higher | Lower |
| Single-injection multi-level coverage | Yes | N/A | No (each level) |
A single-injection PVB for surgical anesthesia has been shown to surpass general anesthesia for postoperative pain relief, incidence of vomiting, and pain on mobilization. - Barash, 9e, p. 2980
The PVB provides anesthesia for breast and cardiothoracic surgery comparable to thoracic epidural, but with fewer complications from central neuraxial blockade. - Miller's, 10e, p. 6254
D. Technique
Landmark/loss-of-resistance technique:
- Patient seated or prone
- Mark 2.5 cm lateral to the superior border of the target spinous process
- Insert needle perpendicular to the skin until the transverse process is contacted (~3-5 cm depth)
- Walk the needle caudally off the inferior edge of the transverse process
- Advance 1-2 cm further, feeling a "pop" as the superior costotransverse ligament is pierced
- Inject 5 mL local anesthetic per level
Ultrasound-guided technique (preferred):
- Parasagittal probe orientation (preferred over transverse approach for better pleural visualization)
- Identify transverse processes of two adjacent levels, the superior costotransverse ligament, and parietal pleura
- In-plane needle approach, caudal-to-cranial trajectory
- Target: just deep to the superior costotransverse ligament
- Endpoint: "smile sign" - local anesthetic depresses the parietal pleura anteriorly, confirming correct injection
Volumes: 15-20 mL per level for single-injection; 5 mL per level for catheter-based multilevel blocks - Miller's, 10e, p. 6255-6256
E. Complications and Risks
| Complication | Notes |
|---|---|
| Pneumothorax | Most feared; actual incidence with US-guidance is low and similar to the operation itself; usually managed conservatively |
| Hypotension | From sympathetic block; significant concern with bilateral blocks |
| Inadvertent epidural/intrathecal injection | Via medial spread through intervertebral foramen; can cause high spinal |
| Vascular injection / LAST | PVS is vascular; total dose must be calculated carefully, especially for bilateral or multilevel blocks |
| Dural puncture | Transverse (medial) needle placement approach - higher risk |
| Spinal cord injury | Infraforaminal approaches carry risk |
| Block failure | 6-10% depending on operator experience |
| Respiratory decompensation | In patients with severe pulmonary disease who rely on intercostal muscles; bilateral block is relatively contraindicated |
| Paresthesia | Inadvertent nerve contact during placement |
- Miller's, 10e, p. 6256-6257; Barash, 9e, p. 2980-2982
F. Local Anesthetic Choices
- Ropivacaine 0.5% or bupivacaine 0.25-0.5% - most commonly used for prolonged postoperative analgesia
- Single injection provides 12-18 hours of analgesia
- Catheter technique extends duration for thoracotomy, post-thoracotomy pain syndrome
- Epinephrine reduces systemic absorption but must be used cautiously given proximity to major vessels
G. Special Considerations
Compared to Erector Spinae Plane (ESP) Block:
The ESP block is gaining popularity as a safer alternative - it is more superficial, remote from the lung, and easier to perform. However, its exact mechanism is debated and the level of evidence for equivalence is still accumulating. The PVB remains the gold standard for true paravertebral neural blockade.
Continuous catheter use:
For post-thoracotomy analgesia, a catheter placed into the PVS and secured provides superior pain management when compared to on-demand systemic opioids. Epidural equivalence has been demonstrated in multiple trials.
Pediatrics:
Continuous PVB has been described for post-thoracotomy analgesia in children and is an accepted technique in pediatric thoracic surgery.
3. Recent Evidence (2024-2026)
Three recent high-level systematic reviews confirm the continued relevance of PVB:
- A 2024 network meta-analysis (PMID 39621976) assessed regional analgesia after thoracic surgery, directly comparing PVB against epidural and newer fascial plane blocks.
- A 2025 Bayesian network meta-analysis (PMID 39740311) compared regional anesthesia modalities in blunt thoracic trauma, confirming PVB efficacy for rib fractures.
- The 2026 PROSPECT guidelines (PMID 41521792) for post-thoracotomy pain management (published in Anaesthesia) provide the most current procedure-specific recommendations on selecting between PVB, epidural, and ESP blocks.
Summary
The paravertebral space is a wedge-shaped anatomical corridor that gives the anesthesiologist direct access to the spinal nerve (both rami), the sympathetic chain, and the rami communicantes - all in a single injection. Its contiguity with the epidural and intercostal spaces explains both the spread of analgesia and the complications. When performed under ultrasound guidance, PVB is a safe, effective alternative to thoracic epidural for unilateral thoracic, breast, and upper abdominal surgery, offering equivalent analgesia with significantly fewer hemodynamic and neuraxial side effects.
This is a shared conversation. Sign in to Orris to start your own chat.