Explain the complete histology of urinary system and prostate
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer. Let me compile it.
Complete Histology of the Urinary System and Prostate
Sources: Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Pawlina/Ross); Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease
PART 1: THE KIDNEY
Overview and Gross Organization
Each kidney is a flattened bean-shaped structure (~10 cm long). Its cut surface reveals two distinct regions:
- Cortex - reddish-brown outer region containing renal corpuscles and convoluted tubules
- Medulla - lighter inner region containing straight tubules (loops of Henle) and collecting ducts arranged into renal pyramids. The apex of each pyramid forms the renal papilla, which opens at an area cribrosa into a minor calyx.
The medullary rays are groups of straight tubules that radiate from the base of each pyramid into the cortex, dividing the cortex into the cortical labyrinth (contains renal corpuscles and convoluted tubules) and medullary rays (contain proximal straight tubules, distal straight tubules, and cortical collecting ducts).
The Nephron - Functional Unit
There are approximately 2 million nephrons per kidney. Each nephron consists of:
- Renal corpuscle
- Proximal tubule (convoluted + straight)
- Thin segment (loop of Henle)
- Distal tubule (straight + convoluted)
- Connecting tubule → collecting duct
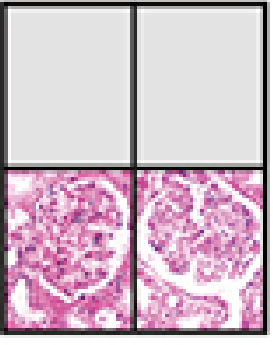
Renal Corpuscle
The renal corpuscle appears as a spherical structure at low power. It contains:
Glomerulus - a tuft of 10-20 capillary loops enclosed by Bowman capsule.
Bowman Capsule - has two layers:
- Parietal layer - simple squamous epithelium lining the outer wall; continuous with the proximal tubule at the urinary pole
- Visceral layer - composed of podocytes (modified epithelial cells) whose processes wrap around glomerular capillaries; their nuclei are large and pale-staining compared to endothelial/mesangial nuclei
Urinary space - the crescent-shaped space between parietal and visceral layers into which the filtrate collects
Two poles:
- Vascular pole - where the afferent arteriole enters and efferent arteriole exits; the juxtaglomerular (JG) apparatus sits here
- Urinary pole - where the urinary space is continuous with the proximal convoluted tubule lumen; epithelium transitions from squamous to cuboidal/columnar with brush border
Three cell types within the glomerulus:
| Cell Type | Location | Function |
|---|---|---|
| Fenestrated endothelial cells | Capillary lumen | Filtration (pores ~70 nm) |
| Podocytes (visceral epithelium) | Outer surface of capillaries | Primary filtration barrier; foot processes with slit diaphragms |
| Mesangial cells | Between capillary loops | Structural support; phagocytosis; contractility |
Glomerular filtration barrier (from lumen to urinary space):
- Fenestrated endothelium
- Glomerular basement membrane (GBM) - type IV collagen + laminin + heparan sulfate
- Podocyte foot processes with slit diaphragms (nephrin protein)
Juxtaglomerular Apparatus (JGA)
Located at the vascular pole, the JGA is a homeostatic sensor comprising:
- Juxtaglomerular (JG) cells - modified smooth muscle cells in the afferent arteriole wall; contain secretory granules loaded with renin; they are the renin-secreting cells
- Macula densa - a cluster of densely-packed cells in the distal convoluted tubule where it returns to lie adjacent to its own glomerulus; nuclei appear crowded and apical cytoplasm is reduced; monitors NaCl concentration in tubular fluid
- Extraglomerular mesangial cells (lacis cells) - fill the angle between afferent and efferent arterioles
Proximal Convoluted Tubule (PCT)
The most prominent tubule in the cortical labyrinth.
- Epithelium: simple cuboidal to low columnar
- Brush border (microvilli): prominent, stains deeply eosinophilic - the defining feature; gives a "fuzzy" luminal border; greatly increases absorptive surface area
- Lumen: appears small and irregular (star-shaped cross-section) due to the thick brush border
- Cytoplasm: intensely eosinophilic; abundant mitochondria (basolateral infoldings interdigitate with mitochondria for active Na⁺-K⁺-ATPase-driven transport)
- Nucleus: large, round, centrally placed; only 2-3 nuclei visible per tubule cross-section
- Function: reabsorbs ~65% of filtered Na⁺, water, glucose, amino acids, HCO₃⁻, phosphate; secretes organic acids, drugs, toxins
Loop of Henle
The U-shaped portion connecting the proximal and distal tubules. Contains:
Proximal straight tubule (thick descending limb) - resembles PCT; found in medullary rays and outer medulla; has brush border
Thin segment - located in the medulla and tips of pyramids; simple squamous epithelium; nuclei bulge into lumen; very thin walls; no brush border; passively permeable to water (descending) and ions (ascending)
Distal straight tubule (thick ascending limb) - simple cuboidal; no brush border; lumen appears wider (more open) than PCT; actively impermeable to water but pumps NaCl out (generates medullary hyperosmolarity)
Distal Convoluted Tubule (DCT)
- Epithelium: simple cuboidal
- No brush border - lumen appears more open than PCT
- Smaller cells with less cytoplasm; more nuclei visible per cross-section than PCT
- Basolateral membrane: highly infolded with mitochondria (active ion transport)
- Function: regulated reabsorption of Na⁺ (aldosterone-sensitive), Ca²⁺ (PTH-sensitive), Mg²⁺
Collecting Duct
Receives urine from multiple nephrons via connecting tubules.
Two cell types:
- Principal (light) cells: pale, few organelles; respond to ADH (aquaporin-2 insertion → water reabsorption) and aldosterone (Na⁺ reabsorption)
- Intercalated (dark) cells: rich in mitochondria; stain darker; regulate acid-base balance (H⁺ secretion, HCO₃⁻ reabsorption)
The collecting duct grows larger in diameter as it courses through the medulla. The papillary ducts of Bellini (the largest collecting ducts) open at the area cribrosa at the tip of the renal papilla. They are lined by tall columnar epithelium.
Renal Interstitium and Blood Supply
The peritubular capillary network supplies the cortex. The vasa recta are hairpin-looped capillaries that supply the medulla and participate in the counter-current exchange mechanism maintaining medullary hypertonicity.
PART 2: EXCRETORY PASSAGES
General Plan
All excretory passages (except urethra) share a common wall structure:
| Layer | Composition |
|---|---|
| Mucosa | Transitional epithelium (urothelium) + lamina propria |
| Muscularis | Smooth muscle bundles with connective tissue |
| Adventitia (or serosa) | Fibrous/adipose tissue with vessels and nerves |
Transitional Epithelium (Urothelium)
This is the defining epithelium of the urinary tract. It is a stratified epithelium uniquely designed to accommodate stretch and provide an impermeable barrier.
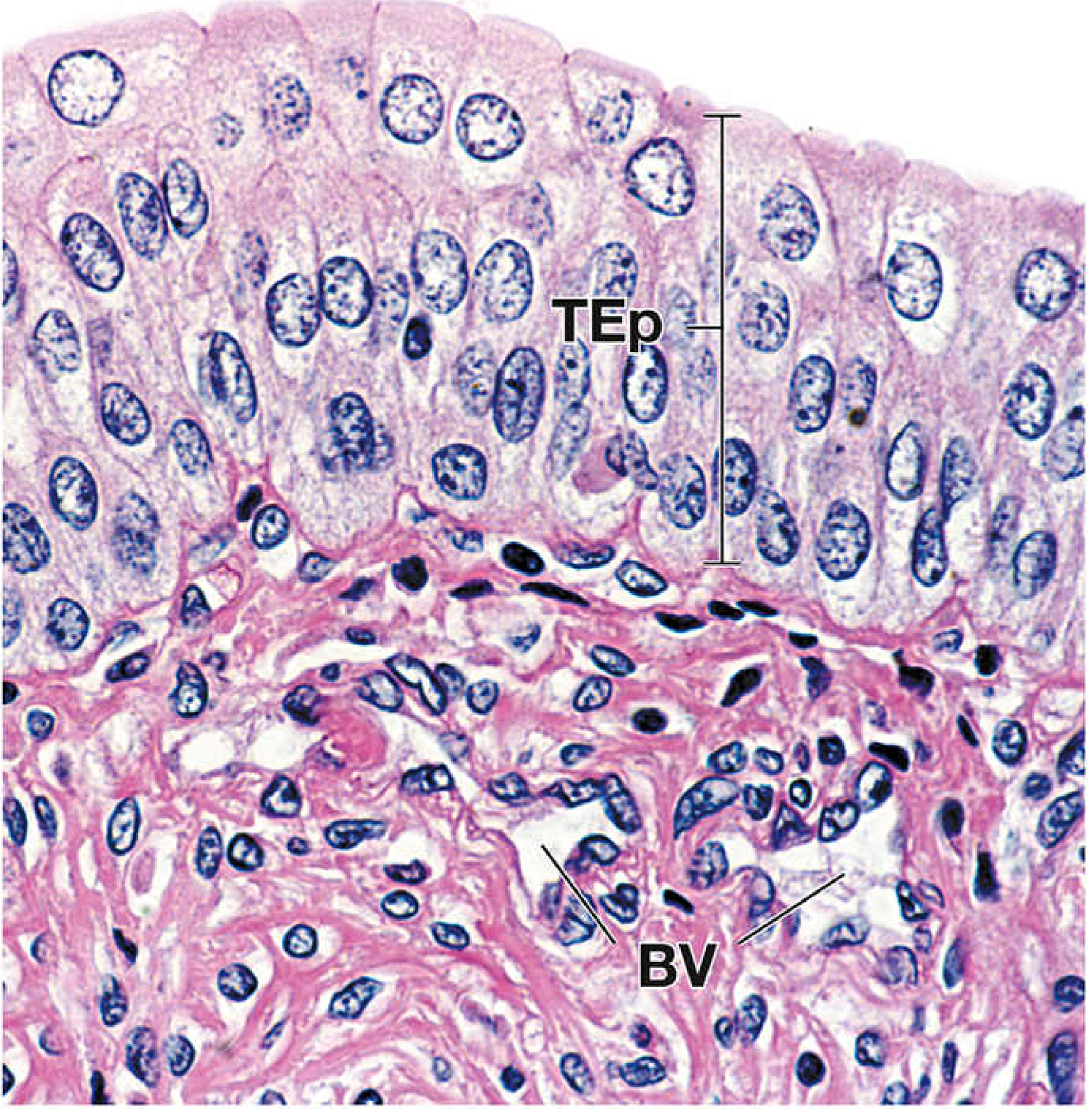
Three layers:
- Basal cells - small, round/polygonal; minimal cytoplasm; resting on the basement membrane
- Intermediate (umbrella precursor) cells - medium-sized; 2-3 layers thick
- Superficial (umbrella/dome) cells - the hallmark - very large, dome-shaped; often binucleate; have a thick, rigid asymmetric unit membrane (AUM) on their apical surface
Ultrastructure of superficial cells:
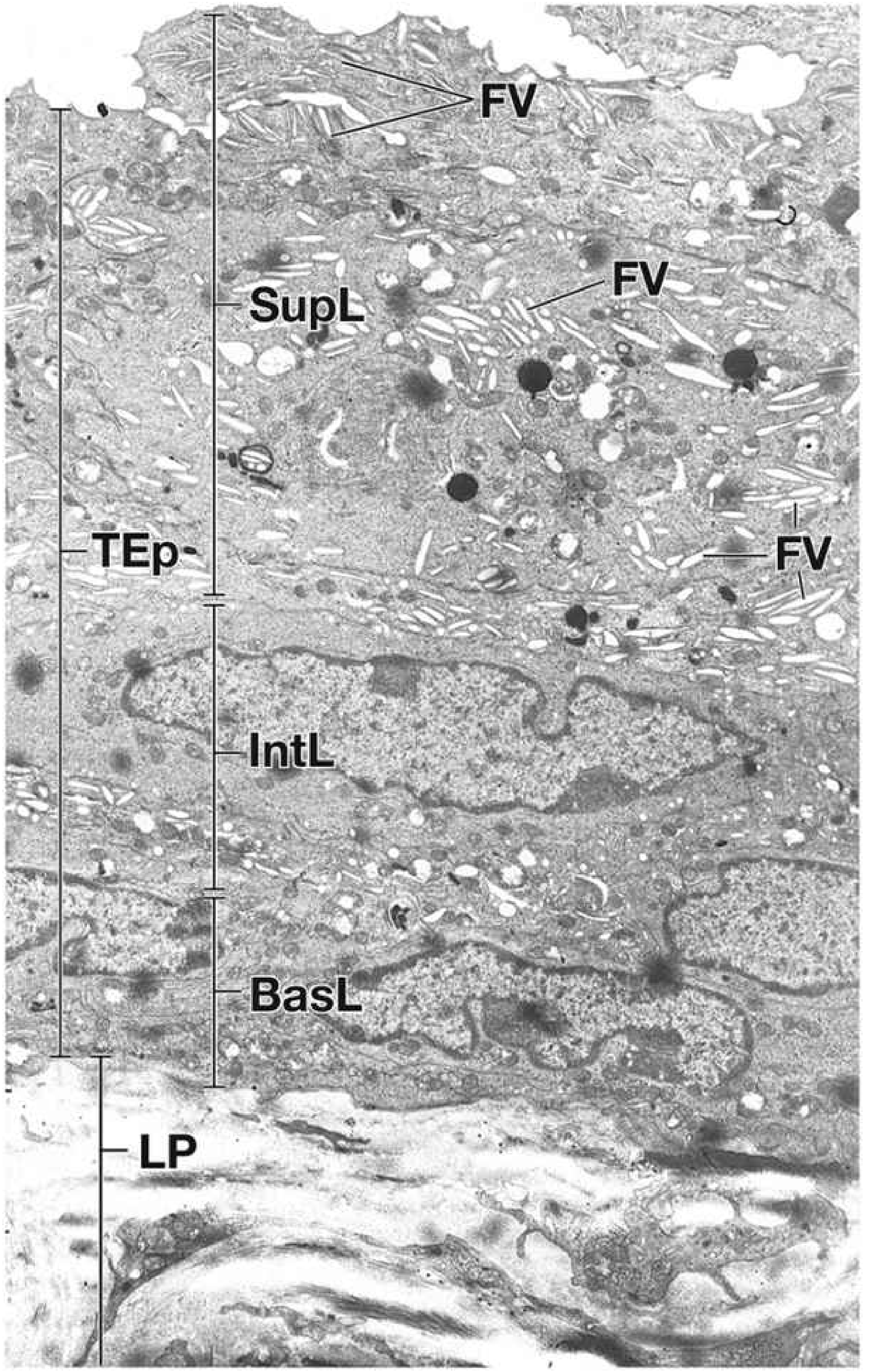
The cytoplasm of umbrella cells contains fusiform vesicles (FV) - membrane-bounded discoid organelles that represent invaginated excess apical membrane. When the bladder fills and the epithelium stretches, these vesicles fuse with the apical membrane to increase surface area. When the bladder empties, the membrane is re-internalized as fusiform vesicles. The apical membrane is composed of uroplakin proteins that form rigid hexagonal plaques.
Thickness variation:
- Relaxed/empty bladder: 4-6+ cell layers visible
- Distended bladder: as few as 2-3 layers (cells spread out, not actually lost)
Renal Calyces and Renal Pelvis
- Epithelium: transitional (2-3 cell layers in minor calyces, thicker in pelvis)
- Lamina propria: fibroelastic connective tissue
- Muscularis: thin smooth muscle, inner longitudinal and outer circular layers
- Adventitia: merges with perinephric fat
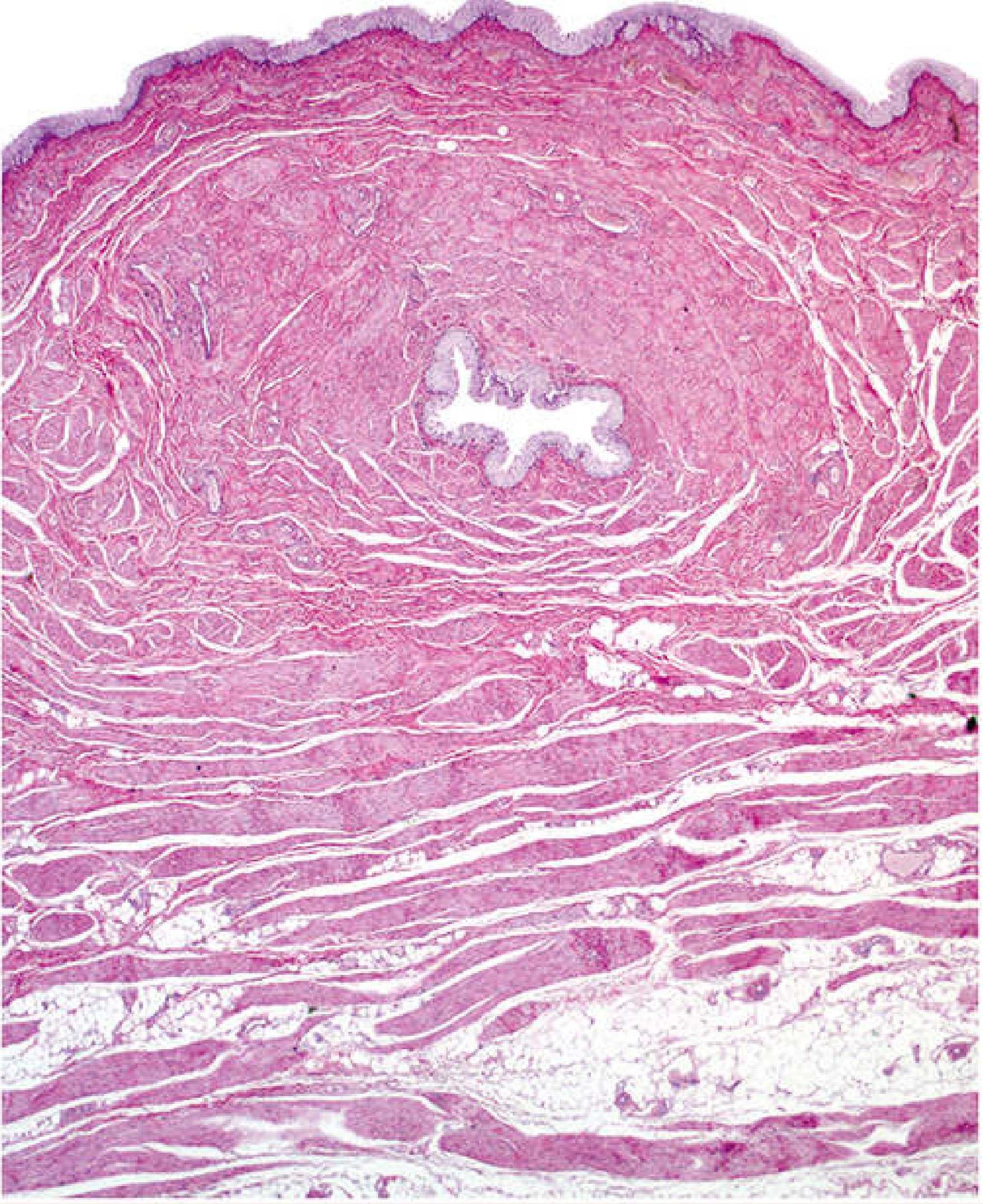
Ureter
- Length: ~24-34 cm
- Mucosa: transitional epithelium (4-5 cells thick when relaxed); underlying lamina propria has dense fibroelastic connective tissue; no muscularis mucosae; wall folds create a star-shaped lumen in cross-section when empty
- Muscularis:
- Upper 2/3: two layers - inner longitudinal and outer circular (note: opposite of gut arrangement)
- Lower 1/3: three layers - inner longitudinal + middle circular + outer longitudinal
- Adventitia: retroperitoneal adipose tissue with vessels and nerves
- The oblique passage through the bladder wall creates a valve effect preventing vesicoureteral reflux
Urinary Bladder
A highly distensible reservoir in the pelvis.
- Mucosa: transitional epithelium (up to 6-10 cell layers when contracted; 2-3 when distended); prominent mucosal folds when empty; lamina propria is highly vascular with loose fibroelastic connective tissue
- Trigone region: embryologically derived from the mesonephric ducts; lacks mucosal folds; no muscularis mucosae or submucosa; smooth and flat at all times
- Muscularis (Detrusor muscle): three poorly-defined interdigitating layers of smooth muscle (inner longitudinal, middle circular, outer longitudinal); bundles are interlaced rather than forming pure sheets; contraction empties the bladder
- Internal urethral sphincter: ring of smooth muscle at the bladder neck (involuntary)
- Serosa (superior surface) or Adventitia (inferior/lateral surfaces)
Urethra
Female urethra (~4 cm):
- Upper half (internal): transitional epithelium continuous with the bladder
- Lower half: pseudostratified or stratified columnar epithelium → stratified squamous epithelium at the external meatus
- Muscularis: inner longitudinal smooth muscle + outer circular smooth muscle; the external urethral sphincter is skeletal muscle (voluntary)
- Paraurethral (Skene's) glands: small mucous glands opening near the external meatus
Male urethra (~20 cm; three regions):
| Segment | Length | Epithelium | Notes |
|---|---|---|---|
| Prostatic urethra | ~3 cm | Transitional (urothelium) | Passes through prostate; verumontanum here |
| Membranous urethra | ~1-2 cm | Stratified/pseudostratified columnar | Pierces the external urethral sphincter (skeletal muscle) |
| Penile (spongy) urethra | ~15 cm | Pseudostratified columnar → stratified squamous at navicular fossa | Traverses corpus spongiosum; Littre's glands (mucous) open here |
PART 3: THE PROSTATE
Anatomy and Zones
The prostate is a retroperitoneal organ (~20 g in adults) that surrounds the proximal urethra just below the bladder neck. It lacks a true capsule but is surrounded by a fibromuscular pseudocapsule.
Four zones (clinically important):
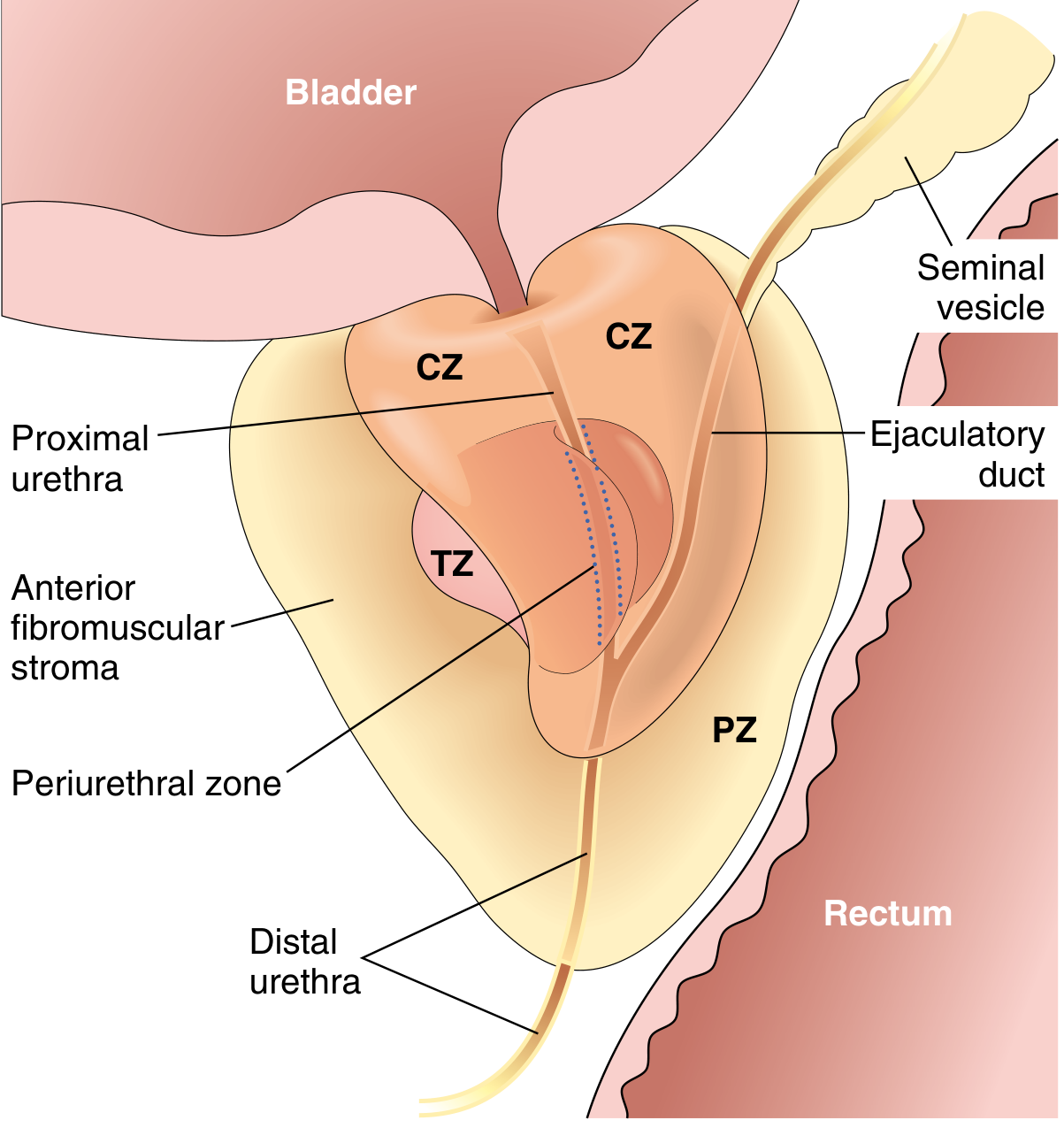
| Zone | Volume | Clinical Relevance |
|---|---|---|
| Peripheral zone (PZ) | ~70% | 70-80% of carcinomas arise here; palpable on DRE |
| Central zone (CZ) | ~25% | Surrounds ejaculatory ducts; less commonly involved |
| Transition zone (TZ) | ~5% (enlarges with age) | Site of benign prostatic hyperplasia (BPH) |
| Periurethral zone | Small | Mucosal glands adjacent to urethra |
The anterior fibromuscular stroma occupies the anterior surface and contains no glandular tissue.
Histological Structure of Normal Prostate
The prostate contains compound tubuloalveolar glands arranged in three concentric groups:
- Mucosal glands - innermost, small, adjacent to urethra
- Submucosal glands - middle layer
- Main (peripheral) glands - outermost; largest; drain into the posterior urethra via excretory ducts
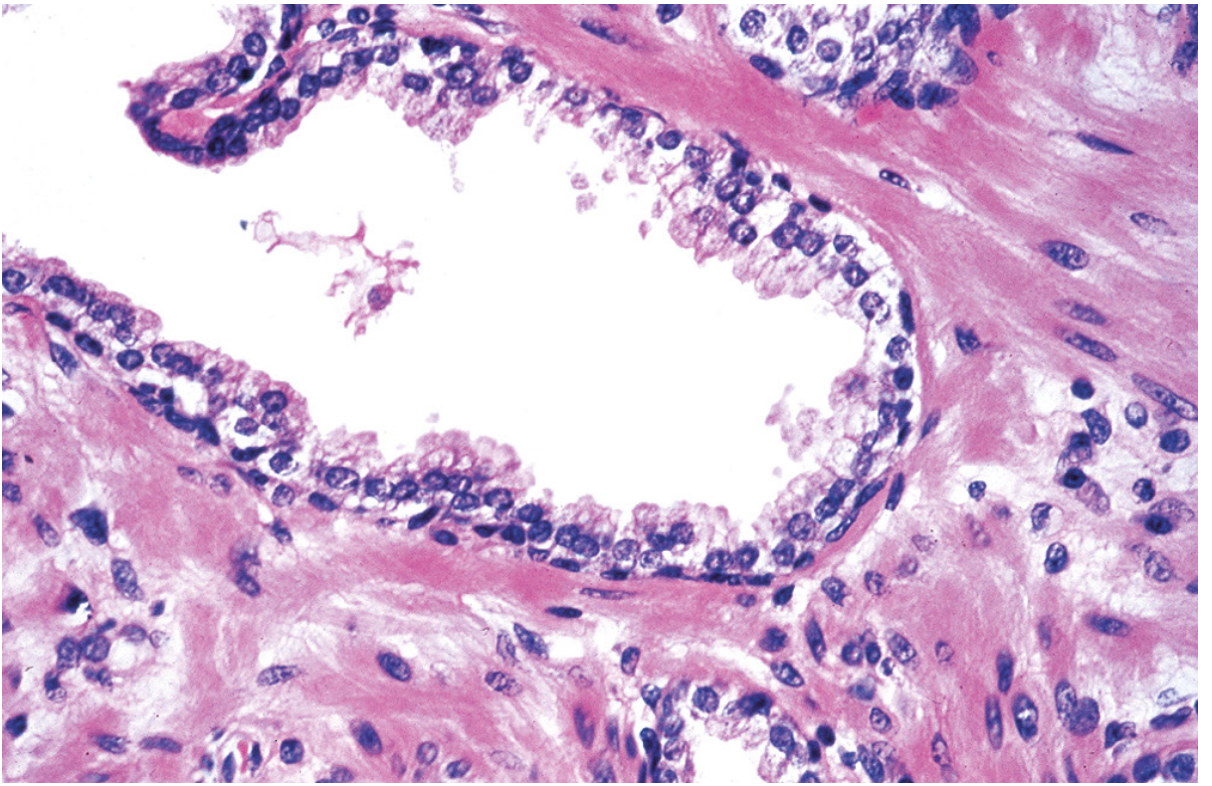
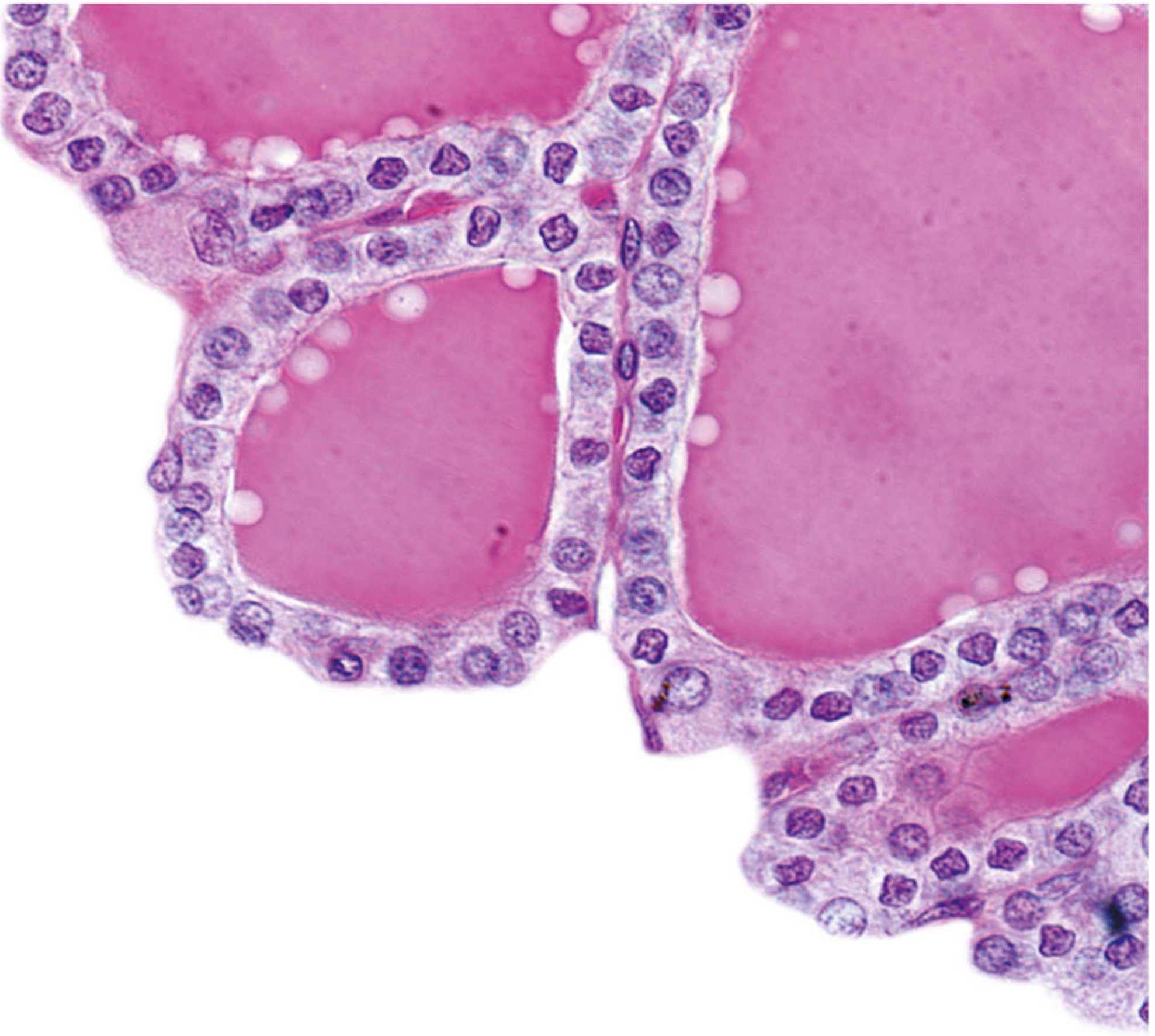
Glandular epithelium - the defining two-cell architecture:
| Layer | Cell Type | Characteristics |
|---|---|---|
| Basal layer | Low cuboidal cells | CK5/CK14-positive; p63-positive; do not secrete; serve as reserve/stem cells |
| Luminal/Secretory layer | Tall columnar cells | PSA-positive; produce prostatic secretions; small apical papillary infoldings into lumen; pale-staining cytoplasm |
Corpora amylacea: rounded, laminated, eosinophilic bodies seen within glandular lumina (especially in older men); represent inspissated secretions; concentric rings of glycoprotein; increase with age; clinically insignificant but a histological landmark.
Luminal content: pale, eosinophilic secretion within gland lumina; small lipid droplets.
Prostatic Stroma
The stroma between glands is abundant and contains:
- Smooth muscle (fibromuscular stroma) - contracts during ejaculation to expel secretions
- Dense fibrous connective tissue - collagen bundles
- Blood vessels, lymphatics, nerves
The ratio of stroma to epithelium is roughly 2:1 in the normal gland.
Hormonal Dependence
Testicular androgens (primarily DHT, converted from testosterone by 5α-reductase within prostatic cells) are essential for growth and maintenance of prostatic epithelium. Castration leads to widespread apoptosis of secretory cells and prostatic atrophy. This is the basis for androgen deprivation therapy in prostate cancer.
Summary Comparison Table
| Structure | Epithelium | Key Histological Feature |
|---|---|---|
| Glomerulus | Podocytes (visceral); squamous (parietal) | Filtration slits; podocyte foot processes |
| PCT | Simple cuboidal, brush border | Prominent microvilli; eosinophilic; narrow lumen |
| Thin limb (Henle) | Simple squamous | Thin walls; nuclei bulge into lumen |
| DCT | Simple cuboidal, no brush border | Open lumen; macula densa at JGA |
| Collecting duct | Simple cuboidal (principal + intercalated) | Two cell types; responds to ADH/aldosterone |
| Calyces/Pelvis/Ureter/Bladder | Transitional (urothelium) | Dome-shaped umbrella cells; fusiform vesicles; binucleate |
| Prostatic urethra | Transitional | Continuous with bladder |
| Penile urethra | Pseudostratified columnar | Littre's glands; squamous at meatus |
| Prostate | Two-cell layer (basal + columnar secretory) | Corpora amylacea; fibromuscular stroma; PSA-producing |
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Pawlina), pp. 1926-1968
- Robbins & Kumar Basic Pathology, 10e, p. 3466-3468
- Robbins, Cotran & Kumar Pathologic Basis of Disease, 10e, p. 1614-1618
Explain the complete histology of lips, cheeks, palate, whole teeth, whole teeth, gums, oropharynx, tubular digestive tract and enteric nervous system
This is a shared conversation. Sign in to Orris to start your own chat.