Estrogen cycle?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks plus a detailed diagram. Let me compile the full answer.
The Estrogen Cycle (Menstrual Cycle)
The menstrual cycle is a coordinated interplay between hypothalamic, pituitary, and ovarian hormones that drives monthly changes in the ovary and uterus. In a standard 28-day cycle, it is divided into an ovarian cycle (follicular + luteal phases) and a uterine cycle (menstrual + proliferative + secretory phases).
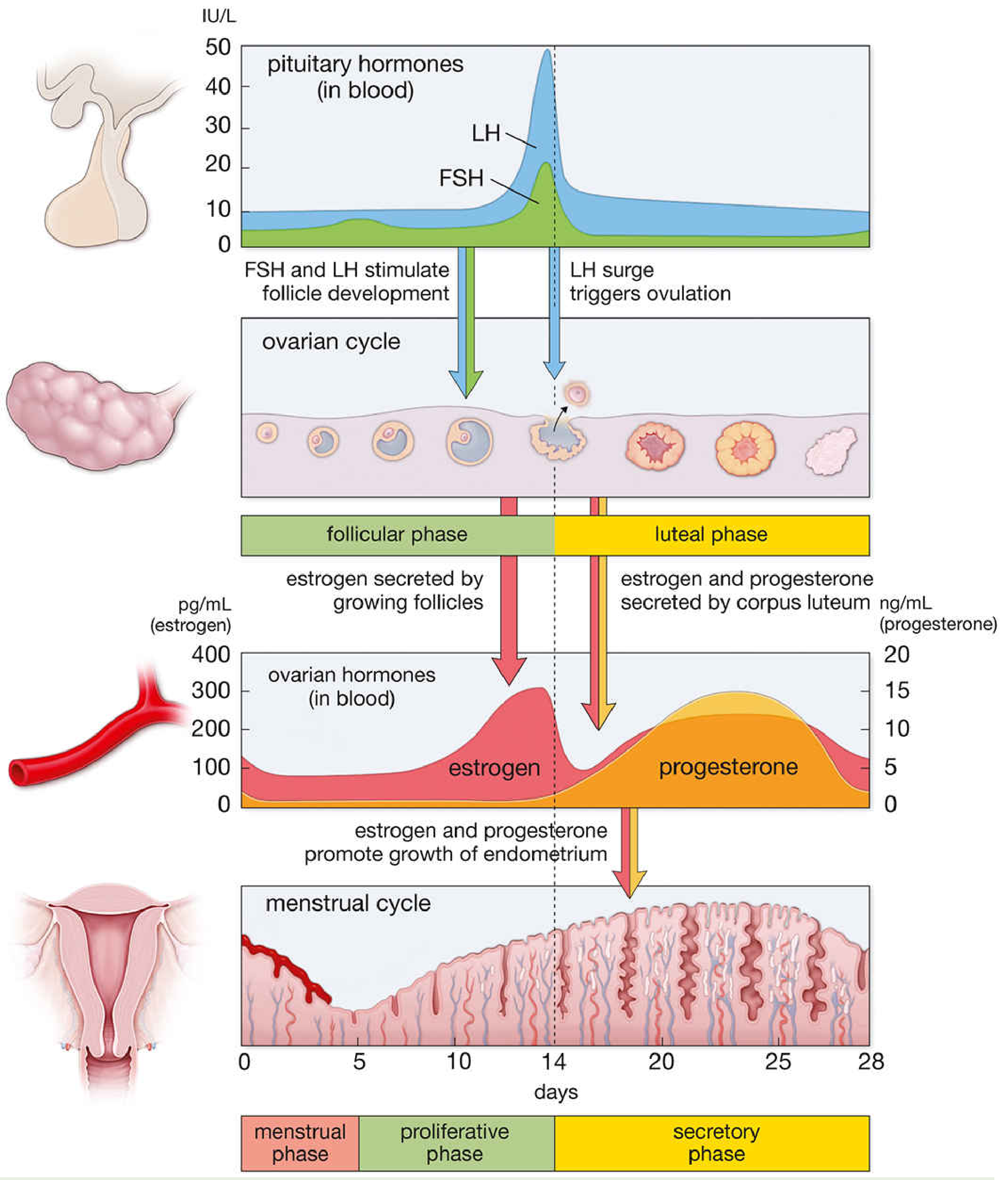
Overview of the 28-Day Cycle
| Day | Phase | Dominant Hormone | Key Event |
|---|---|---|---|
| 1-5 | Menstrual | Low E + P | Endometrial shedding |
| 1-13 | Follicular (ovarian) / Proliferative (uterine) | Rising Estrogen | Follicle growth, endometrial rebuilding |
| ~14 | Ovulation | Estrogen peak → LH surge | Oocyte released |
| 15-28 | Luteal (ovarian) / Secretory (uterine) | Progesterone + Estrogen | Corpus luteum, endometrial secretory prep |
Phase-by-Phase Breakdown
1. Menstrual Phase (Days 1-5)
- At the end of the previous luteal phase, corpus luteum degenerates and estradiol + progesterone levels fall sharply.
- Withdrawal of hormonal support causes vascular and glandular breakdown of the endometrium, leading to menstrual bleeding (day 1 = start of the cycle).
- After menstruation, only a thin layer of stromal cells and remnant glands remain on most of the uterine surface.
(Medical Physiology, p. 1639)
2. Follicular Phase / Proliferative Phase (Days 1-13)
In the ovary:
- With corpus luteum demise, FSH rises and recruits a cohort of growing follicles. Each secretes increasing amounts of estrogen as they grow.
- Rising estrogen initially suppresses FSH (negative feedback) and inhibin B also suppresses FSH, so only the dominant follicle survives.
- Late in the follicular phase, LH shows a biphasic response - initially suppressed by rising estradiol, then dramatically stimulated (positive feedback switch).
- Average follicular phase length: 10-14 days (this is what varies most between women and drives cycle-length differences).
In the uterus:
- Estrogen from the growing follicles drives endometrial proliferation - thickness increases from ~0.5 mm to ~5 mm.
- Estrogen receptor (ER) levels in the endometrium peak during this phase, then decline after ovulation.
- Estradiol also stimulates growth factors (IGFs, TGFs, EGF) to promote endometrial maturation, and induces progesterone receptor (PR) synthesis to prepare for the luteal phase.
(Berek & Novak's Gynecology, p. 280-281; Medical Physiology, p. 1639)
3. Ovulation (~Day 14)
- The mid-cycle LH surge (triggered by the positive feedback of peak estradiol) is the proximate cause of ovulation, which occurs 24-36 hours after the surge.
- Just before ovulation, FSH-induced LH receptors appear on granulosa cells; these, with LH stimulation, trigger progesterone secretion - responsible for the FSH mid-cycle surge.
- Estrogen levels briefly dip just after ovulation.
(Berek & Novak's Gynecology, p. 281)
4. Luteal Phase / Secretory Phase (Days 15-28)
In the ovary:
- The ruptured follicle transforms into the corpus luteum, which secretes both progesterone and estrogen (a second, smaller estrogen peak in mid-luteal phase around day 20-21).
- Inhibin A is co-secreted by the corpus luteum.
- Progesterone, estrogen, and inhibin A act centrally to suppress gonadotropins and new follicular growth.
- If no pregnancy occurs, the corpus luteum degenerates (~day 26-28), hormones fall, and the next cycle begins. If pregnancy occurs, hCG from the trophoblast rescues the corpus luteum until ~week 9 of gestation.
In the uterus (secretory phase):
- Progesterone dominates and actively opposes estrogen action by: (1) inhibiting ER expression, (2) stimulating 17β-HSD to convert estradiol to the weaker estrone, and (3) stimulating sulfotransferase to inactivate estrogens.
- This halts proliferation and switches the endometrium to a secretory mode.
- Endometrial glands become tortuous and engorged; vascularization increases; glycogen accumulates; thickness reaches 5-6 mm. Peak secretory activity occurs around day 20-21.
- Beginning ~9-10 days post-ovulation, stromal cells undergo predecidualization - forming rounded decidual cells with a collagen-rich matrix (laminin, fibronectin, type IV collagen), creating the zona compacta.
(Medical Physiology, p. 1640-1641; Berek & Novak's Gynecology, p. 281)
Estrogen Levels Throughout the Cycle
| Timing | Estrogen Level |
|---|---|
| Early follicular (day 1-5) | Low (~50 pg/mL) |
| Late follicular (day 12-13) | First peak (~300-400 pg/mL) - triggers LH surge |
| Early luteal (day 15-17) | Brief dip |
| Mid-luteal (day 20-22) | Second smaller peak (~150-200 pg/mL) from corpus luteum |
| Late luteal (day 26-28) | Falls sharply → menstruation |
Key Feedback Mechanisms
| Signal | Effect |
|---|---|
| Low estrogen (early follicular) | Stimulates FSH release (negative feedback removed) |
| Rising estrogen (mid-follicular) | Suppresses FSH (negative feedback) |
| Peak estrogen pre-ovulation | Triggers LH surge (positive feedback) |
| Progesterone + estrogen (luteal) | Suppresses LH and FSH (negative feedback), prevents new follicular recruitment |
Clinical Correlates
- Variability in cycle length is almost entirely due to variation in the follicular phase (10-14 days); the luteal phase is nearly constant at ~14 days.
- Anovulatory cycles (common post-menarche and perimenopause) lack the LH surge and corpus luteum, so progesterone is absent - leading to unopposed estrogen stimulation of the endometrium.
- Oral contraceptives (estrogen + progestin combinations) suppress the LH/FSH surge by negative feedback, preventing follicular development and ovulation.
- Lactation suppresses GnRH and FSH/LH via high prolactin, causing amenorrhea.
(Costanzo Physiology 7th Ed., p. 483-484; Berek & Novak's Gynecology, p. 281)
How does clomiphene acts?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Comprehensive data retrieved from three pharmacology references. Here is the full answer:
How Clomiphene Works
Drug Class & Chemistry
Clomiphene citrate is a non-steroidal triphenylethylene compound - structurally related to diethylstilbestrol. It exists as two isomers with opposite activities:
| Isomer | Name | Activity |
|---|---|---|
| cis-clomiphene | Zuclomiphene | Weak estrogen agonist |
| trans-clomiphene | Enclomiphene | Potent estrogen antagonist |
The drug binds to both ERα and ERβ. It is well absorbed orally, has a half-life of 5-7 days, undergoes enterohepatic circulation, distributes to adipose tissue, and is excreted primarily in urine.
(Katzung's Basic and Clinical Pharmacology, 16th Ed.)
Mechanism of Action
The core mechanism is competitive blockade of estrogen receptors in the hypothalamus and pituitary:
- Normally, circulating estradiol exerts negative feedback on the hypothalamus and anterior pituitary, suppressing GnRH, LH, and FSH release.
- Clomiphene occupies hypothalamic ERs and blocks estradiol's negative feedback signal.
- The hypothalamus/pituitary "perceives" estrogen levels as low, even when they are not.
- In response, GnRH pulse frequency increases → anterior pituitary releases more FSH and LH.
- Elevated FSH drives follicular recruitment and development in the ovary.
- Growing follicles produce estradiol, which eventually triggers the LH surge and ovulation.
"Clomiphene probably blocks the feedback inhibitory influence of estrogens on the hypothalamus, causing a surge of gonadotropins, which leads to ovulation." - Katzung's Basic and Clinical Pharmacology, 16th Ed.
The ER-ligand conformation produced by clomiphene is distinct from estradiol's - it recruits different coactivators and corepressors at gene promoters, which explains its tissue-selective partial agonist/antagonist profile (tissue context determines whether coactivators or corepressors dominate).
(Goodman & Gilman's Pharmacological Basis of Therapeutics)
Clinical Use & Dosing Regimen
- Indication: Anovulatory infertility - most commonly polycystic ovary syndrome (PCOS), oligomenorrhea, or amenorrhea. Not useful in ovarian or pituitary failure.
- Dose: 50 mg/day orally for 5 consecutive days, starting days 2-5 of the cycle (or after progesterone-induced withdrawal bleed).
- Can be escalated to 100 mg/day (FDA-approved max) or even 150-200 mg/day if no response.
- Results: Ovulation is induced in ~75% of treated women, but successful pregnancy occurs in only 40-50% of those who ovulate.
Why Pregnancy Rate Lags Behind Ovulation Rate
Clomiphene's anti-estrogenic effect is not limited to the hypothalamus - it also acts on the endometrium and cervical mucus:
- Endometrium: reduced estrogen action leads to a thinner, less receptive lining - suboptimal for implantation.
- Cervical mucus: becomes thicker and hostile to sperm penetration.
This explains the gap between ovulation induction success (~75%) and actual pregnancy rates (~40-50%).
(Goodman & Gilman's Pharmacological Basis of Therapeutics)
Clomiphene vs. Letrozole (Key Comparison)
Because of the endometrial and cervical mucus side effects, letrozole (an aromatase inhibitor) is now preferred over clomiphene in PCOS:
- Letrozole works by reducing estrogen biosynthesis directly → more FSH without prolonged ER blockade.
- Associated with higher pregnancy and live birth rates in PCOS (Legro et al., 2014).
- Fewer estrogen-deprivation side effects, and possibly fewer multifetal pregnancies.
(Goodman & Gilman's Pharmacological Basis of Therapeutics)
Adverse Effects
| Effect | Notes |
|---|---|
| Hot flushes | Most common - resembles menopause, resolves on stopping |
| Ovarian enlargement | Expected; can be marked - monitor carefully |
| Visual disturbances | Prolonged afterimages; caution with driving |
| Multiple pregnancy | ~10% incidence (twins most common) |
| Mood changes, headache, nausea | Mostly from ovulatory hormonal shifts |
| Ovarian hyperstimulation | Rare but possible |
| Long-term use (>1 year) | Possible increased risk of low-grade ovarian cancer (evidence not conclusive) |
(Katzung's Basic and Clinical Pharmacology, 16th Ed.)
Summary Diagram of Action
Low estrogen feedback sensed (ER blocked by clomiphene)
↓
Hypothalamus → ↑ GnRH pulses
↓
Anterior pituitary → ↑ FSH + LH
↓
Ovary → Follicle recruitment & growth → ↑ Estradiol
↓
LH surge → Ovulation
Is It blocks receptors in both site hypothalamus and pituitary land ?
Finding Sources
Finding Sources
Finding Sources
The textbook confirms it clearly. Here is the precise answer:
Clomiphene: Hypothalamus AND Pituitary - Both Sites
Yes, clomiphene acts at both sites, and Berek & Novak's Gynecology states this explicitly:
"Clomiphene citrate is an estrogen antagonist at the hypothalamus and pituitary that promotes gonadotropin release."
However, there is a distinction in emphasis between the two sites:
1. Hypothalamus (Primary/Dominant Site)
- Clomiphene binds and occupies hypothalamic estrogen receptors for prolonged periods (recall its long half-life of 5-7 days).
- This blocks the normal ovarian-hypothalamic estrogen negative feedback loop.
- Result: increased GnRH pulsatility from the hypothalamus.
"Clomiphene citrate is thought to bind and block estrogen receptors in the hypothalamus for prolonged periods, thereby decreasing the normal ovarian-hypothalamic estrogen feedback loop. This blockade increases GnRH pulsatility..." - Berek & Novak's Gynecology
2. Anterior Pituitary (Secondary Site)
- Clomiphene also blocks ERs directly at the pituitary gonadotrophs.
- Estrogen normally acts on the pituitary to suppress FSH and LH release (independent of hypothalamic GnRH).
- By blocking this direct pituitary suppression, clomiphene allows increased secretion of FSH and LH in response to both the elevated GnRH and the removal of direct estrogen inhibition at the pituitary level.
Net Effect: Two-Level Disinhibition
Clomiphene blocks ER at HYPOTHALAMUS
↓
↑ GnRH pulsatility
↓
Anterior pituitary → ↑ FSH + LH
↑
Clomiphene ALSO blocks ER at PITUITARY (direct disinhibition)
Both actions converge to produce a surge in FSH and LH, driving follicular development and ovulation.
Why the Hypothalamus Gets More Emphasis
Most sources emphasize the hypothalamus because:
- It is the upstream regulator - increasing GnRH pulse frequency amplifies the entire downstream axis.
- Estrogen's negative feedback at the hypothalamus is quantitatively more important in humans than its direct pituitary effect.
- The prolonged ER occupancy at the hypothalamus (due to clomiphene's long half-life) is what drives the sustained gonadotropin rise.
So in short: both sites are blocked, but the hypothalamic effect is the dominant driver of the clinical response. (Berek & Novak's Gynecology)
This is a shared conversation. Sign in to Orris to start your own chat.