Chronic heart failure
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"heart failure" AND management
Searching the Web
chronic heart failure overview pathophysiology management 2024
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the material I need for a thorough medical student-level overview. Let me compose the full answer.
Chronic Heart Failure (CHF) - Medical Student Overview
1. Definition
Heart failure is a clinical syndrome in which the heart cannot pump blood at a rate sufficient to meet the metabolic demands of tissues, or can do so only at an elevated filling pressure. It is not a diagnosis in itself but the end result of many cardiac (and non-cardiac) diseases.
2. Classification
By Ejection Fraction (EF)
| Type | EF | Key Feature |
|---|---|---|
| HFrEF (systolic HF) | <40% | Reduced contractility; responds to inotropes & neurohormonal blockers |
| HFmrEF (mildly reduced) | 40-49% | Intermediate; emerging evidence for treatment |
| HFpEF (diastolic HF) | ≥50% | Stiff, non-compliant ventricle; reduced filling |
By Side
- Left-sided HF: Pulmonary congestion - dyspnoea, orthopnoea, PND, pulmonary oedema
- Right-sided HF: Systemic venous congestion - peripheral oedema, raised JVP, hepatomegaly, ascites
High-Output HF (rare)
Demands exceed even increased cardiac output - causes include hyperthyroidism, beriberi (thiamine deficiency), severe anaemia, arteriovenous fistulae. Does not respond to standard HF drugs; treat the underlying cause.
3. Aetiology
Common causes:
- Ischaemic heart disease / myocardial infarction (most common in developed world)
- Hypertension (leads to LV hypertrophy → diastolic dysfunction)
- Valvular heart disease (aortic stenosis, mitral regurgitation)
- Dilated cardiomyopathy (idiopathic, alcoholic, viral myocarditis)
- Diabetes mellitus
- Congenital heart disease
4. Pathophysiology
The hemodynamic model of CHF has been replaced by the neurohormonal / LV remodelling model.
A. Trigger → LV Remodelling
Any injury (MI, hypertension, etc.) causes LV stretching and dilation with progressive reduction in LV function. This remodelling process activates neurohormonal cascades.
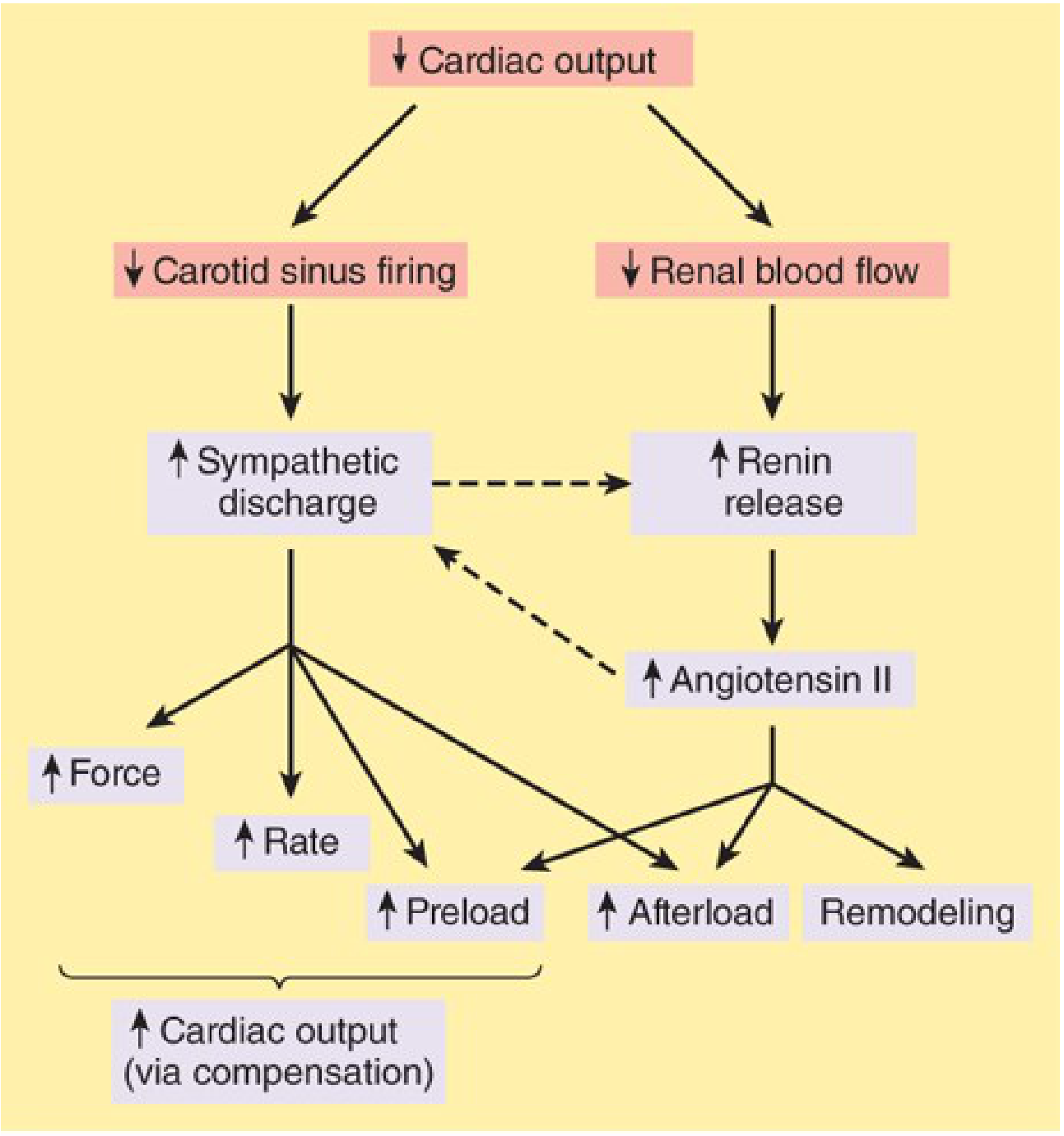
B. Compensatory Neurohormonal Responses
Two major systems are activated:
1. Sympathetic Nervous System (SNS):
- Baroreceptors reset at lower sensitivity → increased sympathetic outflow
- Short-term benefit: increased HR, contractility, venous tone, preload
- Long-term harm: tachycardia, beta-receptor downregulation, catecholamine-mediated myocyte apoptosis, LVH, arrhythmias
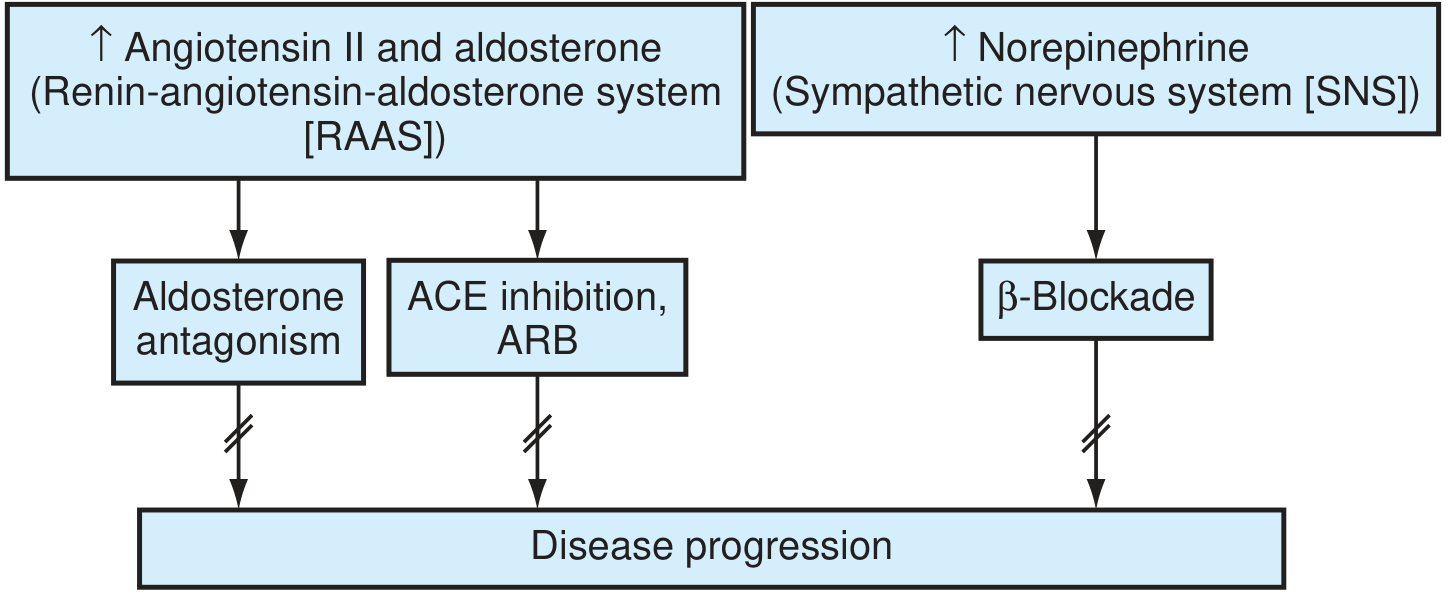
2. Renin-Angiotensin-Aldosterone System (RAAS):
- Reduced renal blood flow → renin release → Angiotensin II
- Angiotensin II: vasoconstriction (↑ afterload), aldosterone release (Na+/water retention → ↑ preload), myocyte apoptosis, ventricular fibrosis
- Aldosterone "escapes" ACE inhibition over time → need for direct aldosterone blockade
Other mediators: Endothelin-1 (potent vasoconstrictor), pro-inflammatory cytokines, MMPs (promoting fibrosis), altered calcium handling, glycolysis replacing fatty acid oxidation.
C. The Vicious Cycle
↓ CO → neurohormonal activation → ↑ afterload → ↓ EF → ↓ CO further. This self-perpetuating spiral drives disease progression.
D. Renal Response
Reduced cardiac output → reduced renal perfusion → oliguria/anuria. The kidneys retain Na+ and water, increasing blood volume. A moderate increase in fluid is initially compensatory (Frank-Starling mechanism), but excessive retention causes oedema and pulmonary congestion.
5. Clinical Features
| Symptom/Sign | Mechanism |
|---|---|
| Dyspnoea (on exertion, then rest) | Pulmonary venous congestion |
| Orthopnoea, PND | Redistribution of fluid when supine |
| Fatigue, exercise intolerance | ↓ Cardiac output to muscles |
| Tachycardia | SNS activation |
| Bilateral pitting oedema | Na+ and water retention, venous hypertension |
| Raised JVP | Right heart congestion |
| Crackles (basal) | Pulmonary oedema |
| S3 gallop | Rapid ventricular filling |
| Cardiomegaly | LV remodelling |
| Hepatomegaly / ascites | Right heart failure |
6. Classification Systems
NYHA Functional Class
| Class | Description |
|---|---|
| I | No limitation; ordinary activity causes no symptoms |
| II | Slight limitation; comfortable at rest, symptoms on moderate exertion |
| III | Marked limitation; comfortable at rest, symptoms on minimal exertion |
| IV | Symptoms at rest; unable to carry out any activity |
ACC/AHA Staging (complements NYHA)
| Stage | Description |
|---|---|
| A | At risk (hypertension, diabetes, IHD) - no structural disease, no symptoms |
| B | Structural heart disease, asymptomatic (≈ NYHA I) |
| C | Structural heart disease + current or prior symptoms (≈ NYHA II-III) |
| D | Refractory HF at rest, requiring advanced interventions (≈ NYHA IV) |
7. Investigations
- ECG: LVH, ischaemic changes, arrhythmias, bundle branch block
- Chest X-ray: Cardiomegaly, Kerley B lines, upper lobe venous diversion, pulmonary oedema (bat-wing appearance)
- Echocardiogram: Confirms and classifies HF; assesses EF, wall motion, valves - key investigation
- BNP / NT-proBNP: Elevated in HF; excellent for diagnosis and monitoring; elevated due to myocyte stretch
- Bloods: FBC (anaemia), U&E (renal impairment, electrolytes), LFTs, TFTs (hypothyroidism), HbA1c, iron studies, lipids
- Coronary angiography: If ischaemic aetiology suspected
- Cardiac MRI: Cardiomyopathy characterisation, viability
8. Management
Principles
- Treat the underlying cause (revascularisation, valve surgery, rate control)
- Remove precipitating factors (infection, arrhythmia, medication non-compliance, fluid excess)
- Neurohormonal blockade to slow remodelling and reduce mortality (HFrEF)
- Symptom relief with diuretics
- Device therapy where appropriate
Drug Treatment for HFrEF ("Four Pillars")
| Pillar | Drug Class | Examples | Benefit |
|---|---|---|---|
| 1 | ACE inhibitor (or ARB if intolerant) | Enalapril, ramipril, losartan | ↓ Mortality, ↓ afterload, slows remodelling |
| 2 | Beta-blocker | Bisoprolol, carvedilol, metoprolol | ↓ Mortality, ↓ HR, ↑ EF over time |
| 3 | Mineralocorticoid receptor antagonist (MRA) | Spironolactone, eplerenone | ↓ Mortality & morbidity, anti-fibrotic |
| 4 | SGLT2 inhibitor | Dapagliflozin, empagliflozin | ↓ HF hospitalisations, natriuresis, metabolic benefits |
ARNI (sacubitril/valsartan - Entresto): Replaces ACE inhibitor/ARB; superior mortality benefit in HFrEF. Combines neprilysin inhibition (↑ natriuretic peptides) with AT1 blockade.
Diuretics (symptomatic relief):
- Loop diuretics (furosemide) - first-line for oedema
- Thiazides - only in very mild failure
- Cause secondary K+ loss → supplement or add MRA/ACEi
Ivabradine: If-channel blocker; reduces HR without affecting contractility; used if HR >70 bpm on max beta-blocker.
Digoxin: Indicated when HF + atrial fibrillation; can reduce symptoms in sinus rhythm when other drugs insufficient; narrow therapeutic index.
Vasodilators (hydralazine + isosorbide dinitrate): Used in patients intolerant of RAAS blockers; particularly recommended in Black patients (BiDil).
Calcium Channel Blockers
Avoid in HFrEF - negative inotropic effect worsens failure. Can be used in HFpEF for rate control and BP reduction.
HFpEF Treatment
Fewer proven mortality-reducing drugs. Focus on:
- Symptom relief: diuretics (cautiously)
- BP control, rate control
- SGLT2 inhibitors and MRAs reduce HF hospitalisations
- ARNI (sacubitril/valsartan) may reduce symptoms
Device Therapy
| Device | Indication |
|---|---|
| ICD (implantable cardioverter-defibrillator) | EF ≤35%, NYHA II-III, on optimal medical therapy - reduces sudden cardiac death |
| CRT (cardiac resynchronisation therapy) | EF ≤35%, LBBB (QRS ≥150ms) - resynchronises ventricular contraction |
| LVAD (left ventricular assist device) | Stage D refractory HF; bridge to transplant or destination therapy |
| Heart transplant | End-stage HF, no contraindications |
Non-pharmacological
- Salt restriction (<2g Na+/day)
- Fluid restriction in severe HF
- Daily weight monitoring (>2kg gain in 2 days = seek review)
- Cardiac rehabilitation / exercise - proven to improve outcomes and quality of life
- Smoking cessation, alcohol reduction (alcoholic cardiomyopathy is reversible)
- Vaccination (influenza, pneumococcal)
9. Complications
- Sudden cardiac death (ventricular arrhythmias) - most common cause of death
- Atrial fibrillation (very common comorbidity; worsens HF)
- Renal failure (cardiorenal syndrome)
- Thromboembolic disease (AF, mural thrombus)
- Hepatic congestion ("cardiac cirrhosis" in severe RHF)
- Cachexia (cardiac cachexia - poor prognosis)
- Depression and poor quality of life
10. Prognosis
- 5-year mortality ~50% (worse than many cancers)
- BNP/NT-proBNP, NYHA class, EF, and renal function are key prognostic markers
- Mortality significantly reduced with the four-pillar pharmacotherapy (ACEi/ARNI + beta-blocker + MRA + SGLT2i)
Recent Evidence (2024-2026)
- SGLT2 inhibitors continue to show benefit even in hospitalised patients: a 2025 meta-analysis (PMID 40884036) including the DAPA-ACT HF-TIMI 68 trial confirmed SGLT2i benefits in patients hospitalised for HF, reinforcing early initiation
- Exercise-based cardiac rehabilitation: A 2024 systematic review/network meta-analysis (PMID 39732888) confirmed that cardiac rehabilitation modes improve outcomes in CHF - supporting its routine recommendation
Key Sources:
- Katzung's Basic and Clinical Pharmacology, 16e (Management of CHF, Pathophysiology)
- Guyton and Hall Textbook of Medical Physiology (Chronic Stage of HF, Treatment)
- Textbook of Family Medicine, 9e (Pathophysiology, ACC/AHA Classification, Evaluation)
- NICE guideline NG106 - Chronic heart failure in adults: diagnosis and management
This is a shared conversation. Sign in to Orris to start your own chat.