case based mcqs on renal physiology 1st yr mbbs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have enough information from Guyton & Hall, Costanzo, and other physiology textbooks to create high-quality case-based MCQs. Let me compose them now.
Case-Based MCQs: Renal Physiology (1st Year MBBS)
Based on Guyton & Hall Textbook of Medical Physiology, Costanzo Physiology, and Ganong's Review
CASE 1 - Glomerular Filtration Forces
A 30-year-old man is brought to the ER after a road traffic accident with massive haemorrhage. His blood pressure drops to 70/40 mm Hg. A urinary catheter shows near-absent urine output.
Q1. Which primary change in Starling forces is responsible for the decreased GFR in this patient?
A) Increased Bowman capsule hydrostatic pressure
B) Increased plasma oncotic pressure
C) Decreased glomerular capillary hydrostatic pressure
D) Increased glomerular filtration coefficient (Kf)
Answer: C
Explanation: GFR = Kf × (P_G - P_B - π_G + π_B). In haemorrhagic shock, systemic hypotension reduces glomerular capillary hydrostatic pressure (P_G, normally ~60 mm Hg), the primary driving force for filtration. This directly reduces the net filtration pressure and hence GFR. The net filtration pressure under normal conditions = 60 - 18 - 32 = +10 mm Hg; even a small fall in P_G dramatically cuts this. (Guyton & Hall, p.328)
CASE 2 - Renal Clearance and Tubular Handling
In a physiology lab experiment, a student measures the following in a volunteer: urine flow = 1 mL/min, urine creatinine = 140 mg/dL, plasma creatinine = 1 mg/dL.
Q2. What is the creatinine clearance, and what does it primarily estimate?
A) 70 mL/min - effective renal plasma flow
B) 125 mL/min - effective renal plasma flow
C) 140 mL/min - GFR
D) 100 mL/min - tubular secretory capacity
Answer: C
Explanation: Clearance = (U × V) / P = (140 mg/dL × 1 mL/min) / 1 mg/dL = 140 mL/min. Creatinine clearance slightly overestimates GFR (vs. inulin clearance of ~125 mL/min) because a small amount of creatinine is tubularly secreted. Since creatinine clearance > inulin clearance (125 mL/min), creatinine must be secreted by the tubules. (Guyton & Hall, p.369)
CASE 3 - Tubular Reabsorption: Glucose and Tm
A 45-year-old woman with poorly controlled type 2 diabetes has a plasma glucose of 400 mg/dL. Urinalysis shows glycosuria (glucose in urine). Her GFR is 125 mL/min.
Q3. Why does glucose appear in the urine in this patient?
A) Glucose is normally secreted into tubules; its secretion has increased
B) The filtered glucose load exceeds the tubular transport maximum (Tm)
C) GFR is so high that glucose cannot be reabsorbed
D) Aldosterone inhibits glucose reabsorption at high concentrations
Answer: B
Explanation: Filtered glucose load = GFR × plasma glucose = 125 mL/min × 4 mg/mL = 500 mg/min. The renal Tm for glucose is approximately 375 mg/min (in most people). When filtered load exceeds Tm, the excess glucose cannot be reabsorbed and spills into urine. Normally, plasma glucose of ~1 g/L leads to a filtered load of ~180 g/day, which is entirely reabsorbed. Glycosuria begins when plasma glucose exceeds ~180 mg/dL (the "renal threshold"). (Guyton & Hall, p.362)
CASE 4 - Renin-Angiotensin-Aldosterone System (RAAS)
A 65-year-old hypertensive woman is found to have 90% stenosis of her right renal artery on angiography. Her plasma renin activity is markedly elevated, and renin levels in the right renal vein are much higher than in the left. She is started on an ACE inhibitor.
Q4. What is the mechanism by which renal artery stenosis leads to hypertension in this patient?
A) Direct mechanical compression increases renal venous pressure
B) Decreased renal perfusion triggers RAAS → angiotensin II-mediated vasoconstriction + aldosterone-mediated Na+ retention
C) Increased urine output due to pressure natriuresis
D) Left kidney hyperfiltration directly raises systemic blood pressure
Answer: B
Explanation: Stenosis reduces perfusion pressure to the right kidney. Juxtaglomerular cells sense low pressure and secrete renin → converts angiotensinogen to angiotensin I → ACE converts it to angiotensin II. Ang II: (1) vasoconstricts arterioles, raising TPR and mean arterial pressure; (2) stimulates adrenal cortex to release aldosterone → increases Na+ reabsorption in collecting duct → expands ECF/blood volume → raises diastolic BP. ACE inhibitors block this cascade by preventing Ang I → Ang II conversion. (Costanzo Physiology, p.[Box 4.2])
CASE 5 - ADH and Urine Concentration
A 25-year-old man with head trauma develops polyuria (urine output 10 L/day). His plasma osmolality is 310 mOsm/L and urine osmolality is 60 mOsm/L (very dilute). Serum sodium is 155 mEq/L.
Q5. What is the most likely underlying mechanism?
A) Excess ADH secretion (SIADH)
B) Primary polydipsia with water overload
C) Deficiency of ADH (central diabetes insipidus)
D) Aldosterone excess causing water diuresis
Answer: C
Explanation: Urine osmolality < plasma osmolality (60 vs. 310 mOsm/L) = the kidneys are excreting dilute urine despite a hyperosmolar plasma - which is physiologically abnormal. ADH (antidiuretic hormone) is needed to insert aquaporin-2 channels in the collecting duct to concentrate urine. Head trauma has damaged the posterior pituitary or hypothalamic nuclei, causing central diabetes insipidus (failure to secrete ADH). The free water clearance is positive (water lost in excess of solute), leading to hypernatraemia. (Guyton & Hall, pp.331-332)
Bonus concept: Free water clearance (C_H2O) = V - C_osm. When C_H2O is positive, the kidney is excreting excess free water. In this patient, free water is being lost, raising plasma Na+.
CASE 6 - Countercurrent Mechanism
A medical student reads that loop diuretics (e.g., furosemide) can impair urinary concentrating ability even when ADH is present.
Q6. Which segment does furosemide primarily inhibit, and why does this impair urine concentration?
A) Proximal tubule Na/K-ATPase - reduces Na reabsorption
B) Thick ascending limb Na-K-2Cl cotransporter - destroys the medullary osmotic gradient
C) Collecting duct aquaporins - prevents water reabsorption
D) Distal convoluted tubule NaCl cotransporter - reduces final urine dilution
Answer: B
Explanation: The thick ascending limb of the loop of Henle actively reabsorbs NaCl (via NKCC2) but is impermeable to water. This creates the hyperosmotic medullary interstitium (gradient up to ~1200 mOsm/L at the papilla). This interstitial gradient is the driving force for water reabsorption from the collecting duct when ADH is present. Furosemide blocks NKCC2, abolishing the medullary gradient. Even if ADH is fully active, there is no osmotic gradient to drive water reabsorption, so concentrated urine cannot be formed. This explains why furosemide causes isotonic urine and is called a "loop diuretic." (Guyton & Hall, pp.331-332)
CASE 7 - Autoregulation of RBF and GFR
A healthy 28-year-old man exercises vigorously. His systolic BP transiently rises to 170 mm Hg. Despite this, his urine output does not dramatically increase.
Q7. Which mechanism primarily maintains GFR relatively constant when arterial pressure rises to 170 mm Hg?
A) Systemic baroreceptor reflex reducing cardiac output
B) Myogenic response - afferent arteriole constricts in response to increased wall stretch
C) Aldosterone suppression reducing tubular reabsorption
D) Increased Bowman capsule pressure opposing filtration
Answer: B
Explanation: Renal autoregulation keeps RBF and GFR stable over a mean arterial pressure range of ~70-170 mm Hg through two mechanisms:
- Myogenic reflex - when BP rises, the afferent arteriole stretches, causing it to contract (reducing RBF and preventing the rise in glomerular pressure).
- Tubuloglomerular feedback (TGF) - increased delivery of NaCl to the macula densa causes afferent arteriole constriction via adenosine/ATP release.
Both mechanisms prevent excessive GFR and pressure diuresis during transient BP rises. (Guyton & Hall)
CASE 8 - Acid-Base: Renal Regulation
A 60-year-old COPD patient has arterial blood gas: pH 7.28, PaCO2 70 mm Hg, HCO3 30 mEq/L. He has been in this state for several weeks.
Q8. What renal compensation is occurring, and which tubular segment is primarily responsible?
A) Kidneys excreting HCO3- via distal tubule to lower pH
B) Kidneys retaining HCO3- and secreting H+ - primarily in proximal tubule (80%) and intercalated cells of collecting duct
C) Kidneys increasing NH4+ excretion alone via the loop of Henle
D) No renal compensation occurs in respiratory acidosis
Answer: B
Explanation: In chronic respiratory acidosis (elevated PaCO2), the kidneys compensate by: (1) Reabsorbing filtered HCO3- - ~80% in the proximal tubule via H+/Na+ exchange (NHE3) and carbonic anhydrase; (2) Generating new HCO3- in the distal tubule and collecting duct via type A intercalated cells secreting H+ into the lumen; (3) Increasing NH4+ excretion (titratable acid excretion) to eliminate net acid. The result is elevated plasma HCO3- (compensatory metabolic alkalosis), partially correcting the pH. The fact that HCO3- = 30 mEq/L (elevated above normal 24 mEq/L) confirms this renal compensation is underway.
CASE 9 - Juxtaglomerular Apparatus
A 3rd-year student is asked: "A patient on a low-sodium diet has her GFR measured. The macula densa cells detect decreased NaCl delivery. What happens next?"
Q9. The correct sequence following decreased NaCl at the macula densa is:
A) Macula densa → releases adenosine → constricts afferent arteriole → decreases GFR
B) Macula densa → reduces adenosine/ATP → dilates afferent arteriole → increases RBF/GFR → also stimulates JG cells to secrete renin
C) Macula densa → stimulates efferent arteriole dilation → decreases filtration fraction
D) Macula densa → directly secretes angiotensin II → causes systemic vasoconstriction
Answer: B
Explanation: The juxtaglomerular apparatus (JGA) consists of: macula densa cells (specialised DCT cells at the end of the loop of Henle), juxtaglomerular (JG/granular) cells in the afferent arteriole wall, and mesangial cells. When NaCl delivery to the macula densa falls (e.g., low-Na diet, reduced GFR), the macula densa signals a decrease in adenosine/ATP release → afferent arteriole dilates → increases RBF and GFR (restoring NaCl delivery). Simultaneously, JG cells are triggered to secrete renin → activates RAAS → increases Na+ reabsorption systemically. This is tubuloglomerular feedback. (Guyton & Hall)
CASE 10 - Potassium Balance
A patient taking spironolactone (aldosterone antagonist) for heart failure develops weakness and ECG changes (peaked T waves, widened QRS). Serum K+ = 6.8 mEq/L.
Q10. In the normal kidney, aldosterone acts primarily on which segment to regulate potassium?
A) Proximal tubule via Na/K-ATPase upregulation
B) Thick ascending limb via NKCC2 stimulation
C) Principal cells of the cortical collecting duct via stimulation of luminal K+ channels (ROMK) and Na+ channels (ENaC)
D) Podocytes of the glomerulus via increased filtration
Answer: C
Explanation: Aldosterone acts on principal cells of the cortical collecting duct (and connecting tubule) to:
- Upregulate ENaC (epithelial Na+ channels) on the luminal membrane → increases Na+ reabsorption
- Upregulate ROMK (K+ channels) on the luminal side → increases K+ secretion into the tubular lumen
- Stimulate basolateral Na/K-ATPase
Net effect: Na+ retained, K+ and H+ excreted. Spironolactone blocks aldosterone receptors → reduces K+ excretion → hyperkalaemia. The ECG changes (peaked T waves, widened QRS, risk of VF) reflect the dangerous cardiac effects of hyperkalaemia.
Quick Reference Summary Table
| Case | Topic | Key Concept |
|---|---|---|
| 1 | GFR determinants | Net filtration pressure = P_G - P_B - π_G |
| 2 | Clearance | Creatinine clearance overestimates GFR (secreted) |
| 3 | Tm for glucose | Glycosuria when filtered load > Tm (~375 mg/min) |
| 4 | RAAS | Renal artery stenosis → renin → Ang II → HTN |
| 5 | ADH/DI | Low urine osmolality + high plasma osm = central DI |
| 6 | Loop diuretics | Furosemide blocks NKCC2 → destroys medullary gradient |
| 7 | Autoregulation | Myogenic + TGF maintain GFR over 70-170 mm Hg |
| 8 | Acid-base | Chronic resp. acidosis → renal HCO3- retention |
| 9 | JGA/TGF | Low NaCl at macula densa → afferent dilation + renin |
| 10 | Aldosterone | Principal cells CCD → ENaC + ROMK → K+ excretion |
Sources: Guyton and Hall Textbook of Medical Physiology (10th/14th ed.) | Costanzo Physiology 7th ed. | Ganong's Review of Medical Physiology 26th ed.
patient with hypokalcema in case of primary hyperaldosteronism leads to impared glucose tolerance why?
Finding Sources
Finding Sources
Searching PubMed
hyperaldosteronism hypokalemia impaired glucose tolerance insulin secretion
Reading File
Reading File
Searching PubMed
primary aldosteronism diabetes glucose metabolism potassium
Reading Article
PMID: 32172621
Excellent - now I have both textbook and recent human clinical trial data. Here is the complete explanation:
Why Does Hypokalaemia in Primary Hyperaldosteronism Cause Impaired Glucose Tolerance?
This is a beautifully integrated physiology-pathology question. The chain runs from excess aldosterone → hypokalaemia → impaired beta-cell insulin secretion → glucose intolerance. Let me break each step down.
Step 1 - Primary Hyperaldosteronism (1° Hyperaldo)
Excess aldosterone (from adrenal adenoma - Conn's syndrome, or bilateral adrenal hyperplasia) acts on principal cells of the cortical collecting duct:
- Upregulates ENaC → Na⁺ retention → hypertension
- Upregulates ROMK (apical K⁺ channels) → excess K⁺ secretion into urine
- Net result: Hypokalaemia + metabolic alkalosis
Step 2 - The Role of K⁺ in Pancreatic Beta-Cell Physiology
This is the central mechanism. Understand the K_ATP channel system in beta cells:
Blood glucose rises
↓
Glucose enters beta cell via GLUT2 → metabolized
↓
ATP/ADP ratio rises
↓
ATP-sensitive K⁺ channels (K_ATP) CLOSE
↓
K⁺ can no longer exit → membrane DEPOLARIZES
↓
Voltage-gated Ca²⁺ channels open → Ca²⁺ enters
↓
Insulin granule exocytosis → INSULIN SECRETED
K⁺ is the pivotal electrolyte that sets the resting membrane potential of beta cells. The normal resting membrane potential of a beta cell is approximately -70 mV, maintained largely by K⁺ conductance.
Step 3 - How Hypokalaemia Blocks This Process
When serum K⁺ is LOW (e.g., 2.5 - 3.0 mEq/L in 1° hyperaldo):
| Effect | Consequence |
|---|---|
| Reduced extracellular K⁺ increases the K⁺ concentration gradient across the beta-cell membrane | More K⁺ tends to leave the cell → membrane becomes hyperpolarized (more negative, e.g., -85 mV) |
| Hyperpolarization raises the threshold needed for depolarization | Voltage-gated Ca²⁺ channels are harder to open |
| Ca²⁺ influx is blunted even when glucose rises | Insulin granule release is suppressed |
The result: Reduced first-phase insulin secretion in response to a glucose load → blood glucose stays elevated longer → impaired glucose tolerance (IGT) and eventually type 2 diabetes mellitus.
Step 4 - Additional Mechanisms Beyond K⁺ (Direct Aldosterone Effect)
Recent human evidence (Adler et al., Hypertension 2020, PMID 32172621) shows aldosterone has direct, K⁺-independent effects on beta cells:
"Aldosterone impairs insulin secretion in isolated islets... After treatment [adrenalectomy or mineralocorticoid receptor antagonist], the C-peptide and insulin response during hyperglycaemic clamp increased significantly (ΔC-peptide +530.5 pmol/L, P=0.004)."
This means aldosterone itself - independent of K⁺ - acts on mineralocorticoid receptors in pancreatic islets to suppress insulin secretion. Additionally, insulin clearance was elevated in active 1° hyperaldo (872 vs. 632 mL/min after treatment), further lowering effective circulating insulin.
Step 5 - Evidence from Diuretic-Induced Hypokalaemia (Parallel Model)
The same mechanism is confirmed by thiazide diuretic studies. From Goodman & Gilman's Pharmacological Basis of Therapeutics:
"The mechanism of impaired glucose tolerance appears to involve reduced insulin secretion... Hyperglycaemia is reduced when K⁺ or a K⁺-sparing diuretic (amiloride) is given along with the thiazide diuretic."
From the National Kidney Foundation Primer on Kidney Diseases:
"Hyperglycaemia/glucose intolerance has been linked to diuretic-induced hypokalaemia, with subsequent inhibition of pancreatic β-cell mediated insulin secretion - a likely dose-dependent effect that is potentially reversible upon withdrawal."
The SHEP trial quantified this: 45% higher risk of new-onset diabetes per 0.5 mEq/L decline in serum K⁺.
Complete Mechanistic Summary Diagram
Primary Hyperaldosteronism (Conn's Adenoma / Bilateral Hyperplasia)
↓
Excess Aldosterone
/ \
↑ Na⁺ reabsorption ↑ K⁺ secretion in CCD
(via ENaC) ↓
→ Hypertension HYPOKALEMIA (K⁺ < 3.5 mEq/L)
↓
Beta-cell membrane HYPERPOLARIZES
(more K⁺ efflux due to ↑ K⁺ gradient)
↓
K_ATP channels stay open (paradoxically)
Voltage-gated Ca²⁺ channels do NOT open
↓
↓ Ca²⁺ influx → ↓ Insulin exocytosis
↓
IMPAIRED GLUCOSE TOLERANCE / Diabetes
PLUS: Direct aldosterone effect on islet MR receptors
→ ↓ Insulin secretion (K⁺-independent pathway)
→ ↑ Insulin clearance
Clinical Correlation - Why This Matters
| Feature | Explanation |
|---|---|
| Reversal after treatment | Adrenalectomy or spironolactone restores K⁺ and improves insulin secretion |
| Not permanent | IGT in 1° hyperaldo is often reversible once K⁺ is corrected (unlike T2DM) |
| Screening implication | In a hypertensive diabetic patient, always check for 1° hyperaldo - correction may improve glycaemia |
| Potassium supplementation | K⁺ replacement alone can partially restore insulin secretion |
One-Line Answer for Exams
Hypokalaemia in primary hyperaldosteronism hyperpolarizes pancreatic beta-cell membranes by increasing the K⁺ efflux gradient, preventing voltage-gated Ca²⁺ channel opening, blunting Ca²⁺-mediated insulin exocytosis, and thus impairing glucose-stimulated insulin secretion - leading to impaired glucose tolerance.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics | National Kidney Foundation Primer on Kidney Diseases, 8e | Adler GK et al., Hypertension 2020, PMID 32172621 - Primary Aldosteronism Decreases Insulin Secretion and Increases Insulin Clearance in Humans
what is meant by impaired glucose tolerance
Finding Sources
Finding Sources
Reading File
Reading File
Here is a clear, complete explanation:
Impaired Glucose Tolerance (IGT) - What It Means
Simple Definition
Impaired Glucose Tolerance (IGT) is a pre-diabetic condition where the body's response to a glucose load is abnormal - blood glucose rises higher than it should and stays elevated longer than normal - but does not yet reach the threshold for a diabetes diagnosis.
It sits in the "grey zone" between normal glucose metabolism and frank diabetes mellitus.
The Spectrum of Glucose Homeostasis
(Harrison's Principles of Internal Medicine, 22e)
Normal Glucose → Pre-diabetes → Diabetes Mellitus
Tolerance (IGT / IFG)
←————————————————————————————————————————————————————————————→
(a spectrum, not abrupt categories)
Diagnostic Criteria (OGTT - Oral Glucose Tolerance Test)
The test: patient fasts overnight, drinks 75 g glucose in water, blood glucose measured at 2 hours.
| Category | Fasting Plasma Glucose | 2-hr Post-glucose (OGTT) | HbA1c |
|---|---|---|---|
| Normal | < 100 mg/dL (5.6 mmol/L) | < 140 mg/dL (7.8 mmol/L) | < 5.6% |
| IGT (Pre-diabetes) | 100-125 mg/dL | 140-199 mg/dL (7.8-11.0 mmol/L) | 5.7-6.4% |
| Diabetes | ≥ 126 mg/dL | ≥ 200 mg/dL (11.1 mmol/L) | ≥ 6.5% |
(Quick Compendium of Clinical Pathology, 5th ed. | Harrison's 22e)
So in IGT:
- The 2-hour glucose = 140 to 199 mg/dL after a 75 g oral glucose load
- It does NOT meet the ≥ 200 mg/dL cutoff for diabetes
Companion Condition: Impaired Fasting Glucose (IFG)
IGT and IFG are related but different:
| IFG (Impaired Fasting Glucose) | IGT (Impaired Glucose Tolerance) | |
|---|---|---|
| When measured | Fasting state | 2 hours after glucose load |
| Glucose range | 100-125 mg/dL | 140-199 mg/dL |
| What it reflects | Increased hepatic glucose output (liver not suppressed well) | Reduced insulin secretion from beta cells + peripheral insulin resistance |
A person can have IFG alone, IGT alone, or both together.
Why Does It Happen? - The Underlying Physiology
In a normal person, when you eat/drink glucose:
Glucose absorbed → Blood glucose rises
↓
Pancreatic beta cells detect rise
↓
Rapid FIRST-PHASE insulin release (within 0-10 min)
↓
Insulin drives glucose into liver, muscle, fat
↓
Blood glucose returns to normal within 2 hours
In IGT, this process is sluggish or incomplete:
- Reduced first-phase insulin secretion - beta cells don't respond quickly enough to the glucose spike
- Insulin resistance - liver, muscle, and fat cells don't respond well to the insulin that IS secreted
- Increased hepatic glucose output - the liver keeps releasing glucose even after a meal
Result: glucose peaks higher and stays elevated longer → 2-hr glucose = 140-199 mg/dL.
Why IGT Matters Clinically
| Risk | Detail |
|---|---|
| Progression to T2DM | ~25-30% of IGT patients develop T2DM within 5 years |
| Cardiovascular risk | Elevated even before frank diabetes develops |
| Reversible | Lifestyle changes (diet, exercise, weight loss) can normalize glucose tolerance |
| Metformin | Can be used to delay progression in high-risk pre-diabetic individuals |
Harrison's 22e specifically notes: "Individuals with type 2 DM may return to the impaired glucose tolerance category with weight loss" - confirming IGT is a dynamic, reversible state, not a one-way door.
Connecting Back to Primary Hyperaldosteronism
In your previous question's context:
- Hypokalaemia → beta-cell hyperpolarization → blunted first-phase insulin secretion
- This specifically impairs the 0-30 minute insulin response to glucose
- The 2-hour glucose therefore stays elevated in the 140-199 mg/dL range = IGT
- Once the K⁺ is corrected (spironolactone or adrenalectomy), beta-cell function can recover and glucose tolerance normalises - which is why IGT in primary hyperaldosteronism is potentially reversible, unlike primary T2DM
One-line exam answer: IGT is a pre-diabetic state defined by a 2-hour plasma glucose of 140-199 mg/dL on OGTT, reflecting reduced insulin secretion and/or peripheral insulin resistance, placing the individual at significant risk for progression to type 2 diabetes mellitus.
Sources: Harrison's Principles of Internal Medicine 22e | Quick Compendium of Clinical Pathology 5th ed. | Tintinalli's Emergency Medicine
mechanism of action of insulin via insulin receptor
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Excellent - I have the full signaling diagram and rich textbook content. Here is the complete explanation:
Mechanism of Action of Insulin via the Insulin Receptor
The Insulin Receptor - Structure First
The insulin receptor is a receptor tyrosine kinase (RTK) - a transmembrane glycoprotein made of two α and two β subunits linked by disulfide bonds into a heterotetrameric structure (α₂β₂).
| Subunit | Location | Function |
|---|---|---|
| α subunit (×2) | Entirely extracellular | Insulin binding site; also inhibits β subunit kinase activity in the resting state |
| β subunit (×2) | Spans the membrane; cytoplasmic tail | Contains the tyrosine kinase domain |
- Receptor density varies enormously: 40 receptors/cell on erythrocytes → 300,000 receptors/cell on hepatocytes and adipocytes
- Insulin binds with picomolar affinity (extremely high sensitivity)
(Katzung Basic & Clinical Pharmacology 16e | Goodman & Gilman's)
The Signaling Cascade - Step by Step
Here is the full pathway diagram from Goodman & Gilman's:
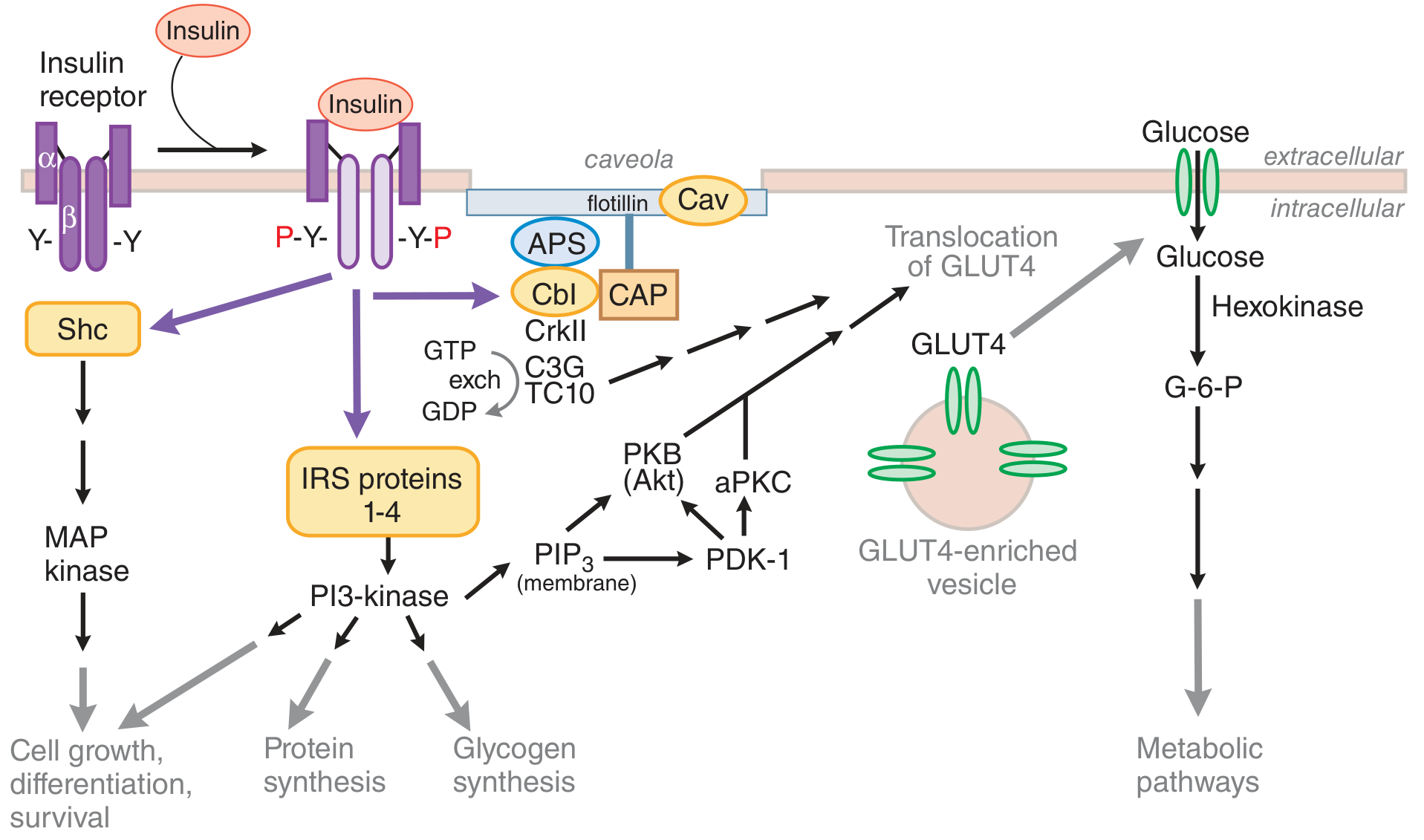
STEP 1 - Insulin Binding → Conformational Change
- Insulin binds to the α subunits on the extracellular surface
- The α subunits normally inhibit the β subunit kinase activity
- Binding releases this inhibition and causes a conformational change that brings the two cytoplasmic β subunit tails into close proximity
STEP 2 - Autophosphorylation (Tyrosine Kinase Activation)
- The two β subunits transphosphorylate each other - each phosphorylates tyrosine (Y) residues on the other's cytoplasmic tail
- This is called autophosphorylation
- Key tyrosines phosphorylated span from the juxtamembrane region to the intracellular tail
- Result: the receptor's intrinsic tyrosine kinase is now fully active
Resting state: α ——[inhibits]—— β (kinase OFF)
After insulin: α-insulin β-P (kinase ON) ←→ β-P
↑ mutual transphosphorylation
STEP 3 - IRS Protein Phosphorylation (First Docking Step)
- The activated receptor now phosphorylates IRS proteins (Insulin Receptor Substrates 1-4) on multiple tyrosine residues
- IRS proteins are docking/adaptor proteins - they have no enzymatic activity themselves but carry SH2-domain binding motifs
- Phosphorylated IRS proteins then recruit and activate downstream effectors
STEP 4 - TWO Major Downstream Pathways Branch Off
Pathway A: PI3K → Akt → GLUT4 (Metabolic Pathway)
This is the main metabolic arm - responsible for glucose uptake, glycogen synthesis, and fat metabolism.
IRS (phosphorylated)
↓
Activates PI3K (Phosphatidylinositol-3-Kinase)
↓
PI3K generates PIP₃ (Phosphatidylinositol 3,4,5-trisphosphate) at membrane
↓
PIP₃ recruits and activates PDK-1 (Phosphoinositide-dependent kinase-1)
↓
PDK-1 phosphorylates and activates Akt2 (PKB - Protein Kinase B)
↓
Akt2 substrates:
├── GLUT4 vesicle translocation → glucose uptake ↑
├── Glycogen synthase kinase 3 (GSK-3) inhibited → Glycogen synthase ACTIVE → Glycogen synthesis ↑
├── mTOR activation → Protein synthesis ↑
└── Inhibits gluconeogenesis in liver
Pathway B: Shc → Ras → MAPK (Mitogenic Pathway)
This is the growth and proliferation arm.
Receptor also phosphorylates Shc (Src-homology protein)
↓
Shc recruits Grb2 (Growth factor receptor-binding protein 2)
↓
Grb2 activates SOS (guanine nucleotide exchange factor)
↓
SOS activates Ras (GTP-binding protein)
↓
Ras → Raf → MEK → MAPK (MAP Kinase / ERK)
↓
Nuclear effects: gene transcription, cell growth, differentiation, survival
Pathway C: Caveolar Pathway (Alternative GLUT4 route)
- In the caveola (lipid raft microdomains), the insulin receptor phosphorylates Cav (caveolin), APS, and Cbl
- Cbl recruits CAP → CrkII → C3G → activates TC10 (small GTPase)
- TC10 coordinates actin cytoskeleton remodeling needed for GLUT4 vesicle docking at the plasma membrane
- Works in parallel with the PI3K pathway to ensure GLUT4 translocation
STEP 5 - GLUT4 Translocation (The Key Glucose Uptake Step)
This is the most important outcome for blood glucose lowering:
Resting state:
~95% of GLUT4 is stored inside the cell in
"GLUT4-enriched vesicles" (intracellular compartment)
→ Very little glucose enters the cell
After insulin signaling (Akt2 + TC10 activation):
GLUT4 vesicles move to the plasma membrane
GLUT4 inserts into the membrane (exocytosis)
Insulin also REDUCES GLUT4 endocytosis
→ More GLUT4 stays on the surface longer
→ Glucose enters by FACILITATED DIFFUSION down its concentration gradient
Tissues where this matters: Skeletal muscle (~85% of post-meal glucose uptake) and adipose tissue. The liver uses GLUT2 (insulin-independent, always present).
STEP 6 - Intracellular Glucose Metabolism
Once glucose enters the cell via GLUT4:
Glucose
↓ (Hexokinase II - also upregulated by insulin)
Glucose-6-Phosphate (G6P)
├── → Glycogen (via glycogen synthase - activated by insulin)
├── → Glycolysis (ATP production)
└── → Pentose phosphate pathway (NADPH, nucleotide synthesis)
Insulin also enhances glycogen synthase activity directly via Akt → GSK-3 inhibition.
Complete Summary Table of Insulin's Cellular Effects
| Pathway | Key Mediators | Metabolic Effect |
|---|---|---|
| PI3K → Akt2 | PIP₃, PDK-1, Akt2 | GLUT4 translocation → ↑ glucose uptake |
| PI3K → mTOR | Akt, mTORC1 | ↑ Protein synthesis, cell growth |
| PI3K → GSK-3 inhibition | Akt → GSK-3 OFF | ↑ Glycogen synthesis |
| PI3K → liver | Akt → FOXO1 inhibition | ↓ Gluconeogenesis, ↓ hepatic glucose output |
| MAPK/ERK | Shc → Ras → MAPK | Cell growth, differentiation, survival |
| Lipid metabolism | Akt → lipase inhibition | ↓ Lipolysis in adipose, ↑ lipogenesis |
| Na/K-ATPase | (mechanism still being clarified) | ↑ K⁺ uptake into cells (explains why insulin treats hyperkalaemia) |
Signal Termination
The insulin signal is terminated by:
- Protein tyrosine phosphatases - especially PTP1B which dephosphorylates the receptor and IRS proteins
- Receptor internalization (endocytosis) after insulin binding
- PI-3 phosphatases (PTEN, SHIP2) that break down PIP₃
Connecting to Insulin Resistance (T2DM)
In type 2 diabetes and obesity:
- Serine phosphorylation (not tyrosine) of IRS-1 by inflammatory signals (TNF-α, free fatty acids, JNK kinase) blocks downstream signaling
- PI3K/Akt pathway is blunted → reduced GLUT4 translocation → hyperglycaemia
- MAPK pathway is often preserved → continued cell growth effects (one reason for cardiovascular complications)
One-Line Exam Summary
Insulin binds α subunits of its tetrameric RTK receptor → releases inhibition of β subunit tyrosine kinase → autophosphorylation → IRS proteins phosphorylated → (1) PI3K/Akt/GLUT4 pathway mediates glucose uptake and glycogen synthesis; (2) Shc/Ras/MAPK pathway mediates cell growth and gene transcription.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics | Katzung Basic & Clinical Pharmacology 16e
i need in simple way and clear understanidning
Here is the same concept explained in the simplest possible way:
Insulin Receptor - Simple Explanation
Think of it Like a DOOR and a KEY 🔑
Insulin = the Key Insulin Receptor = the Lock + Door mechanism GLUT4 = the door for glucose to enter the cell
The Receptor Structure (Simple)
The insulin receptor sits on the surface of cells (muscle, fat, liver).
It has 4 parts joined together:
OUTSIDE the cell: [α]———[α] ← these grab insulin
| |
INSIDE the cell: [β] [β] ← these do the work
- α parts → outside → hold insulin
- β parts → inside → have the "engine" (tyrosine kinase = a phosphorylating enzyme)
What Happens Step by Step
🔴 BEFORE Insulin (fasting state)
- The α parts are sitting on top of β parts and blocking them
- The engine is OFF
- GLUT4 channels are hiding inside the cell
- Glucose cannot enter the cell
🟢 AFTER Insulin Binds (fed state)
Step 1 - Insulin grabs the receptor
Insulin binds to the α subunits
↓
α subunits change shape
↓
They STOP blocking the β subunits
Step 2 - The β subunits wake up and phosphorylate each other
β subunit 1 adds a phosphate (P) to β subunit 2
β subunit 2 adds a phosphate (P) to β subunit 1
↓
Both β subunits are now ACTIVE
(This is called autophosphorylation)
Think of it like two people slapping each other awake simultaneously!
Step 3 - IRS proteins get activated
Active β subunits grab IRS proteins
(IRS = Insulin Receptor Substrate = a "messenger")
↓
IRS proteins get phosphorylated (switched ON)
↓
IRS now go and deliver the message inside the cell
Step 4 - Two messages are sent (two pathways)
The Two Pathways (Super Simple)
Path 1 - The GLUCOSE PATH (most important)
IRS → activates PI3K
↓
PI3K makes PIP₃
↓
PIP₃ activates Akt (also called PKB)
↓
Akt tells GLUT4 vesicles:
"GO TO THE SURFACE!"
↓
GLUT4 channels pop up on the cell membrane
↓
Glucose rushes INTO the cell
Blood sugar FALLS ✅
Key point: GLUT4 is normally hiding inside the cell. Insulin is the only signal that brings it to the surface in muscle and fat cells.
Path 2 - The GROWTH PATH
IRS → activates MAPK pathway
↓
Cell growth, protein synthesis,
cell survival, gene activation
What Happens to Glucose Once Inside?
Glucose enters via GLUT4
↓
Hexokinase converts it to Glucose-6-Phosphate
↓
┌────────────────────────┐
↓ ↓
Stored as GLYCOGEN Burned for ENERGY (ATP)
(in liver & muscle) (glycolysis)
Insulin also:
- Stops the liver from making new glucose (gluconeogenesis OFF)
- Stops fat breakdown (lipolysis OFF)
- Promotes fat storage (lipogenesis ON)
- Drives K⁺ into cells (that's why insulin is used to treat high potassium in emergencies)
The FULL Picture in One Diagram
INSULIN
↓
[α]———[α] ← insulin binds here
| |
[β]-P-[β] ← autophosphorylation (engine ON)
↓
IRS proteins
↙ ↘
PI3K pathway MAPK pathway
↓ ↓
Akt activation Ras → ERK
↓ ↓
GLUT4 → surface Cell growth
↓
GLUCOSE enters cell
↓
Glycogen + Energy
Memory Trick
"IBM-GAG"
- I - Insulin binds α subunit
- B - Beta subunit autophosphorylation
- M - Messenger IRS activated
- G - PI3K → Akt → GLUT4 translocation
- A - Akt also activates glycogen synthesis
- G - Glucose enters, blood sugar falls
Why This Matters in Disease
| Situation | What Goes Wrong |
|---|---|
| Type 2 Diabetes | IRS proteins are blocked → PI3K/Akt doesn't work properly → GLUT4 doesn't move to surface → glucose stays in blood |
| Primary Hyperaldosteronism (your previous question) | Low K⁺ → beta cells can't release insulin → so the whole cascade above never even starts |
| Type 1 Diabetes | No insulin at all → receptor never activated → GLUT4 never reaches surface |
Bottom line in one sentence:
Insulin binds its receptor → switches on a tyrosine kinase engine → sends a message via IRS and PI3K → GLUT4 channels move to the cell surface → glucose enters the cell → blood sugar falls.
what is akt mentioned above
Great question! Akt is simply a protein kinase (an enzyme that adds phosphate groups to other proteins, switching them ON or OFF). It's one of the most important "relay switches" inside the cell.
What is Akt? - Simple Explanation
The Name First
Akt has three names - all mean the same thing:
| Name | What it stands for |
|---|---|
| Akt | Named after a mouse cancer virus "AKT8" where it was first discovered |
| PKB | Protein Kinase B |
| RAC-PK | Related to A and C kinase |
For exams: just remember Akt = PKB = a serine/threonine kinase inside the cell.
What Kind of Protein is Akt?
Akt is a serine/threonine kinase - meaning it adds phosphate groups specifically to serine or threonine amino acids on other proteins.
- When Akt is inactive → sitting in the cytoplasm, doing nothing
- When Akt is active → it goes around phosphorylating (switching ON/OFF) many target proteins
Where Does Akt Sit in the Insulin Pathway?
Think of it as the "main manager" in the PI3K pathway:
Insulin
↓
Receptor tyrosine kinase activated
↓
IRS proteins activated
↓
PI3K activated
↓
PI3K makes PIP₃ (a lipid signal at the membrane)
↓
PIP₃ recruits Akt to the membrane
↓
PDK-1 phosphorylates Akt → Akt is NOW ACTIVE ✅
↓
Akt goes and does its jobs...
So Akt is activated by PIP₃ + PDK-1, and it sits right in the middle of the insulin signaling chain.
What Does Akt Actually Do? (Its Jobs)
Once active, Akt phosphorylates many downstream targets. Think of Akt as a manager sending orders to multiple departments:
ACTIVE Akt
↓
┌──────────┼──────────┬────────────┐
↓ ↓ ↓ ↓
GLUT4 GSK-3 FOXO1 mTOR
moves to turned turned activated
surface OFF OFF
↓ ↓ ↓ ↓
Glucose Glycogen Stops Protein
enters synthesis making new synthesis
cell turns ON glucose increases
Job by job:
Job 1 - GLUT4 translocation
- Akt (specifically the Akt2 isoform) signals GLUT4 vesicles to move to the cell surface
- This is the main way insulin lowers blood glucose in muscle and fat
Job 2 - Glycogen synthesis
- Akt phosphorylates and switches OFF GSK-3 (glycogen synthase kinase-3)
- GSK-3 normally blocks glycogen synthase
- When GSK-3 is OFF → glycogen synthase turns ON → glycogen is made
- Think: Akt turns OFF the "glycogen blocker"
Job 3 - Stop liver glucose production
- Akt phosphorylates and inactivates FOXO1 (a transcription factor)
- FOXO1 normally turns ON genes for gluconeogenesis (making new glucose)
- When FOXO1 is OFF → liver stops making glucose → blood sugar falls further
Job 4 - Protein synthesis
- Akt activates mTOR (mammalian target of rapamycin)
- mTOR promotes protein synthesis → muscle growth, cell building
Job 5 - Cell survival
- Akt phosphorylates and inactivates Bad (a pro-apoptosis protein)
- Cell does NOT die → survival promoted
Simple Analogy
Imagine Akt is like a factory supervisor who just got orders from head office (insulin). The supervisor runs around telling each department what to do:
- "Glucose department - open the gates (GLUT4)!"
- "Storage department - start making glycogen!"
- "Fuel department - stop making new glucose!"
- "Construction department - build more proteins!"
The 3 Isoforms of Akt (Simple)
There are 3 types of Akt in the body:
| Isoform | Main Location | Main Job |
|---|---|---|
| Akt1 | Everywhere | Cell survival and growth |
| Akt2 | Muscle, fat, liver | Glucose metabolism (main insulin-relevant one) |
| Akt3 | Brain | Brain development |
For insulin action, Akt2 is the key player.
Why Akt is Important in Disease
| Disease | What happens to Akt |
|---|---|
| Type 2 Diabetes | Akt activation is reduced because IRS is blocked by inflammation → less GLUT4 on surface → hyperglycaemia |
| Cancer | Akt is overactive in many cancers (keeps cells alive, promotes growth) - PTEN (the Akt "brake") is often mutated |
| PCOS | Impaired Akt signaling in muscle → insulin resistance |
One-Line Summary
Akt (PKB) is a serine/threonine kinase activated by PI3K/PIP₃ during insulin signaling - it is the central "relay switch" that drives GLUT4 to the cell surface, activates glycogen synthesis, suppresses liver glucose production, and promotes protein synthesis.
This is a shared conversation. Sign in to Orris to start your own chat.