Epidemic dropsy in psm
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a complete account of Epidemic Dropsy as covered in Preventive and Social Medicine (PSM):
Epidemic Dropsy
Definition
Epidemic dropsy refers to periodic outbreaks of non-inflammatory oedema, predominantly seen in India, caused by consumption of mustard oil adulterated with argemone oil (oil extracted from Argemone mexicana, commonly called prickly poppy).
Causative Agent
- Plant: Argemone mexicana (prickly poppy) - grows wild across India, has prickly leaves and bright yellow flowers
- Toxic alkaloid: Sanguinarine (and dihydrosanguinarine) - isolated by Mukherji et al. in 1941
- Mechanism of toxicity: Sanguinarine interferes with oxidation of pyruvic acid, which accumulates in the blood; it also causes oxidative stress, pulmonary toxicity, and cardiac damage
Historical note: The cause was unknown until 1926, when Sarkar first ascribed it to mustard oil-argemone oil adulteration. Lal and Roy (1937) and Chopra et al. (1939) provided experimental proof.
Why Contamination Occurs
Seeds of A. mexicana closely resemble mustard seeds in size and are harvested together in March (when both crops mature simultaneously). Contamination may be:
- Accidental - argemone weeds mixed during harvest
- Deliberate - unscrupulous dealers adding argemone oil to mustard oil
Clinical Features
Symptoms appear gradually after consuming adulterated oil:
| System | Features |
|---|---|
| General | Sudden, bilateral, non-inflammatory, pitting oedema of legs; generalized anasarca |
| GI | Loss of appetite, nausea, vomiting, dyspepsia, diarrhoea |
| CVS | Fall of BP, quick/weak pulse, dyspnoea, features of myocardial damage, CCF, palpitation, tachycardia |
| Respiratory | Breathlessness on exertion, pulmonary oedema |
| Hepatic | Enlarged, tender liver |
| Skin | Subcutaneous telangiectasis/haemangiomas (peripheral vasodilatation), purplish blotches over lower limbs, hair loss; burning sensation if oil applied to scalp |
| Mucosa | Small fleshy dark-red growths on cheek, gums, tongue, nose |
| Neurological | Tingling, hyperaesthesia, diminished/absent deep tendon reflexes |
| Eyes | Glaucoma (~1/10 cases) with raised intraocular pressure, retinal haemorrhages, disc oedema, dimness of vision |
| Blood | Normocytic hypochromic anaemia |
| Renal | Renal failure (severe cases) |
- Disease may occur at all ages except breast-fed infants
- Mortality: 5-50%, death results from heart failure
Differential Diagnosis
- Anaemia/hypoproteinaemia
- Nephrotic syndrome
- Beri-Beri
- Filariasis
- Hypothyroidism
Detection / Diagnosis
Tests for Argemone Oil in Suspected Oil Sample
| Test | Method | Result |
|---|---|---|
| Nitric acid test | Add nitric acid to oil, shake | Brown to orange-red colour (positive when argemone oil ≥0.25%) |
| Paper chromatography | Most sensitive test | Detects argemone oil down to 0.0001% in edible oils/fats |
| TLC | Thin-layer chromatography | Confirmatory |
| Ferric chloride test | Used in clinical lab | Detection of sanguinarine |
Clinical diagnosis is supported by history of food habits and toxicological analysis of food/grain samples.
Treatment
- Decontamination - remove the source (stop consuming adulterated oil)
- Supportive measures - Vitamin A, Vitamin E, calcium supplementation
- Treat complications (cardiac failure, glaucoma, pulmonary oedema)
Prevention and Control
- At source: Remove argemone weeds growing among oil-seed crops before harvest
- Legislative: Strict enforcement of the Prevention of Food Adulteration Act
- Testing: Routine chemical testing of edible oils at production and retail level
Key Points for Exam
| Feature | Detail |
|---|---|
| Cause | Mustard oil + argemone oil adulteration |
| Toxin | Sanguinarine |
| Plant | Argemone mexicana (prickly poppy) |
| Discovery | Sarkar, 1926; isolated by Mukherji, 1941 |
| Mechanism | Pyruvic acid accumulation |
| Hallmark sign | Bilateral non-inflammatory leg oedema |
| Unique feature | Telangiectasis/haemangiomas on skin |
| Eye complication | Glaucoma (10% cases) |
| Spared group | Breast-fed infants |
| Mortality | 5-50% |
| Best detection test | Paper chromatography (0.0001%) |
| Simple bedside test | Nitric acid test (≥0.25%) |
Sources: Park's Textbook of Preventive and Social Medicine; PC Dikshit Textbook of Forensic Medicine & Toxicology; Essentials of Forensic Medicine & Toxicology (36th ed., 2026)
Herd immunity
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
I have comprehensive information from multiple authoritative sources. Here is the complete answer:
Herd Immunity
Definition
Herd immunity (also called community immunity) describes a type of immunity that occurs when the vaccination (or prior infection) of a sufficient proportion of a population provides indirect protection to unprotected individuals. When large numbers in a population are immune, it becomes difficult to maintain a chain of infection - the higher the proportion of immune individuals, the lower the likelihood that a susceptible person will contact an infectious agent.
- Park's Textbook of Preventive and Social Medicine
Concept and Mechanism
Herd immunity provides an immunological barrier to the spread of disease through the human herd. The key principle is this: in diseases passed person-to-person, a susceptible individual is protected not because they are personally immune, but because surrounding immune people block transmission chains.
Classic example - Faroe Islands measles epidemic (1854):
When measles was introduced into a "virgin" population with no prior immunity, attack rates and case-fatality rates were extremely high, affecting practically all susceptibles. The epidemic wave declined only with build-up of herd immunity from natural infection.
Elements Contributing to Herd Immunity
Three factors determine herd immunity in any population:
| Element | Details |
|---|---|
| (a) Clinical and subclinical infections | Natural infection in the herd confers immunity to survivors |
| (b) Immunization of the herd | Vaccination programs - most reliable way to build and sustain immunity |
| (c) Herd structure | The composition, density, and social behaviour of the population |
Herd Structure - Key Points
- Never constant - subject to variation due to new births, deaths, and population mobility
- Includes not just the human hosts, but also presence of alternative animal hosts, insect vectors, and environmental/social factors favouring or inhibiting spread
- An ongoing immunization programme keeps herd immunity at a consistently high level
Herd Immunity Threshold (HIT)
The herd immunity threshold is the proportion of immune individuals in a population above which a disease can no longer persist.
Formula:
HIT = 1 - (1/R₀)
Where R₀ = Basic reproduction number (number of secondary cases produced by one case in a fully susceptible population)
Its value varies with:
- Virulence of the disease
- Efficacy of the vaccine
- Contact parameter for the population (how densely people interact)
HIT Values for Common Diseases
| Disease | R₀ | HIT Required |
|---|---|---|
| Measles | 12-18 | 93-95% |
| Poliomyelitis | 5-7 | ~80-85% |
| Diphtheria | 6-7 | ~75-85% |
| Rubella | 5-7 | ~83-85% |
| Mumps | 4-7 | ~75-85% |
| Smallpox | 5-7 | ~80-85% |
Measles requires the highest coverage (~93-95%) because it is one of the most contagious human viruses. National coverage at 92% in the US and Canada has still allowed outbreaks in pockets of under-vaccinated communities.
Important Practical Points
100% Immunity is NOT Required
Studies have shown it is neither possible nor necessary to achieve 100% herd immunity to halt an epidemic or control disease - as demonstrated by the eradication of smallpox and near-elimination of poliomyelitis.
Disease-specific Limitations
- Tetanus: Herd immunity does NOT protect the individual, because the organism (Clostridium tetani) persists in soil as spores from animal faeces - there is no human-to-human transmission chain to break.
- Diphtheria: ~75% immunization of children led to disappearance of disease from communities.
- Smallpox eradication: While herd immunity was important, eradication was achieved primarily through surveillance and containment (elimination of the source of infection), not herd immunity alone. After abolition of smallpox vaccination, herd immunity naturally declines over time.
Determination of Herd Immunity
Herd immunity levels in a population can be assessed by:
- Serological surveys (serological epidemiology) - measuring circulating antibody titres in representative population samples
When Herd Immunity Breaks Down
When the level of immunity in a community falls below the threshold:
- Susceptible individuals accumulate (new births, waning immunity, vaccine hesitancy)
- Even fully vaccinated individuals can become infected (e.g., measles cases in 2-dose vaccinated persons)
- Outbreaks occur in clusters - such as mumps outbreaks among university students, or measles in religious communities objecting to vaccination
- Unvaccinated travelers can "import" infection from endemic areas and spark outbreaks in under-vaccinated pockets
Significance in Disease Control
| Level of Herd Immunity | Outcome |
|---|---|
| Low | Epidemic spread likely |
| Moderate | Slower spread, smaller epidemics |
| At/above HIT | Disease dies out; epidemic halted |
| Sustained high level | Possible elimination/eradication |
The key public health message: there is no room for complacency - herd immunity must be actively maintained through ongoing immunization programmes. Individual vaccine refusal not only puts the unvaccinated person at risk, but removes their contribution to community protection, endangering immunocompromised persons, newborns, and others who cannot be vaccinated.
Sources: Park's Textbook of Preventive and Social Medicine; Roitt's Essential Immunology; Harrison's Principles of Internal Medicine 22E (2025); Jawetz, Melnick & Adelberg's Medical Microbiology 28E
Marasmus
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, exam-ready account of Marasmus:
Marasmus
Definition
Marasmus is a severe form of Protein-Energy Malnutrition (PEM) caused by chronic, global deficiency of both protein and total calories. It represents the body's adapted starvation response - a progressive wasting of muscle and subcutaneous fat in infancy and early childhood.
- The word derives from the Greek marasmos meaning "wasting"
- It is the "dry" form of PEM (contrast with kwashiorkor, the "wet"/oedematous form)
Aetiology / Causes
- Inadequate intake of both protein AND energy (total caloric deficiency)
- Early weaning from breastfeeding without adequate replacement nutrition
- Poverty, food insecurity, chronic infections (impose catabolic stress)
- Chronic diarrhoeal illness, malabsorption
- Children with marasmus are <60% of expected body weight for age
Pathophysiology - "Adapted Starvation"
In marasmus, decreased intake of all macronutrients (especially carbohydrates) leads to:
- Suppressed insulin production - catabolic hormones act unopposed
- Early: Glycogen converted to glucose; then muscle breakdown begins within 24 hours, enabling gluconeogenesis
- Later: Fat breakdown creates ketone bodies, which the brain and CNS can use - this reduces the need for further muscle breakdown, partially sparing lean body mass
- Low leptin stimulates the hypothalamic-pituitary-adrenal axis → high cortisol → promotes lipolysis
- Visceral protein compartment is depleted only marginally - serum albumin is therefore normal or near-normal
- In prolonged starvation, all fat stores are exhausted and lean body mass is consumed
This adaptive mechanism explains why marasmic children do not develop oedema (contrast with kwashiorkor where non-suppressed insulin + protein deficiency → hypoalbuminaemia → oedema).
Clinical Features
Age: Typically infants <1 year of age
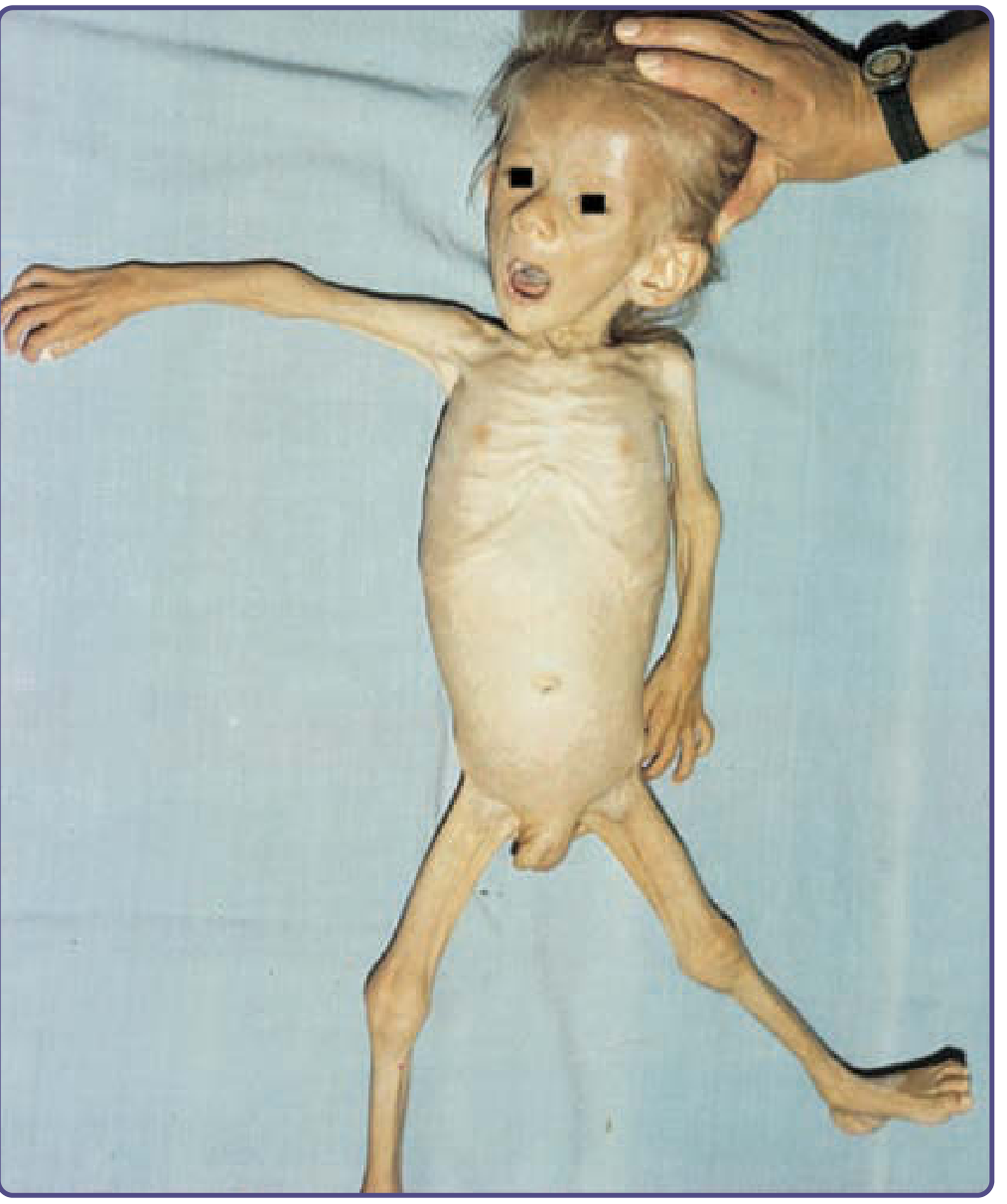
(Left in comparison image below: Marasmus showing visible ribs and severe wasting. Right: Kwashiorkor with oedema and abdominal distension)

| System | Clinical Features |
|---|---|
| General | Severe wasting, failure to thrive, growth retardation, weight <60% expected |
| Face | Loss of buccal fat pads → aged/"monkey facies" (wizened appearance) |
| Skin | Dry, thin, loose, wrinkled skin (from loss of subcutaneous fat); no oedema |
| Hair | Loss of hair; fine, brittle, sparse; alopecia; increased lanugo hair |
| Nails | Fissuring, impaired nail growth |
| Musculoskeletal | Profound muscle atrophy and wasting; visible ribs and bones; head appears too large for body |
| Abdomen | Abdominal muscle hypotonia → abdominal distension; rectal prolapse (from perianal fat loss) |
| GI | Alternating diarrhoea and constipation; angular cheilitis |
| CVS | Bradycardia, decreased resting body temperature |
| Blood | Anaemia (hypochromic microcytic due to iron deficiency; mixed if folate deficient too) |
| Immune | Immunodeficiency - particularly T-cell-mediated immunity; concurrent infections common |
| Neuro | Cerebral atrophy, reduced neurons, impaired myelination (if malnutrition in first 1-2 years) |
| Albumin | Normal or slightly reduced (key distinguishing point from kwashiorkor) |
Morphology / Pathological Findings (Robbins)
| Organ | Finding in Marasmus |
|---|---|
| Growth | Growth failure, stunting |
| Muscle | Profound atrophy |
| Subcutaneous fat | Severely depleted |
| Liver | NOT enlarged, NOT fatty (contrast with kwashiorkor) |
| Small bowel | Relatively preserved (mucosal atrophy seen mainly in kwashiorkor) |
| Bone marrow | Hypoplastic, reduced red cell precursors → anaemia |
| Lymphoid tissue | Thymic and lymphoid atrophy (less marked than in kwashiorkor) |
| Brain | Cerebral atrophy, impaired myelination |
Marasmus vs Kwashiorkor - Key Differences
| Feature | Marasmus | Kwashiorkor |
|---|---|---|
| Deficiency | Calories + protein both | Protein >> calorie deficit |
| Age | <1 year | 1-5 years (post-weaning) |
| Type of starvation | Adapted | Non-adapted |
| Oedema | Absent | Present (hallmark) |
| Weight | <60% expected | 60-80% expected (masked by oedema) |
| Serum albumin | Normal/near-normal | Low (hypoalbuminaemia) |
| Subcutaneous fat | Severely lost | Relatively spared |
| Muscle wasting | Severe | Moderate |
| Buccal fat pads | Lost (monkey facies) | Present |
| Liver | Normal | Enlarged, fatty |
| Skin changes | Wrinkled, loose | Hyperpigmented, desquamation |
| Hair changes | Fine, brittle, alopecia | Depigmentation, flag sign |
| Insulin | Suppressed | Not suppressed |
| Cortisol | High | - |
Marasmic Kwashiorkor
A hybrid form where stunting is combined with oedema - features of both conditions overlap.
Assessment / Detection of PEM
| Tool | Details |
|---|---|
| Weight for age | First and most practical indicator of PEM |
| Growth charts | Can be used by field health workers |
| Mid-upper arm circumference (MUAC) | Used 1-5 years; >13.5 cm = normal; 12.5-13.5 cm = mild-moderate malnutrition; <12.5 cm = severe malnutrition |
| BMI | Height/weight ratio for age |
Treatment
- Nutritional rehabilitation - gradual refeeding (avoid refeeding syndrome - risk of hypophosphatemia with aggressive refeeding)
- Treat concurrent infections
- Correct micronutrient deficiencies (iron, folate, vitamins)
- WHO 10-step protocol for severe acute malnutrition
Prevention of PEM (including Marasmus)
(a) Health Promotion:
- Nutritional support for pregnant and lactating women
- Promote breastfeeding
- Develop low-cost weaning foods; frequent small feeds
- Improve family diet
- Nutrition education - correct feeding practices
- Family planning and birth spacing
(b) Specific Protection:
- Protein and energy-rich foods - milk, eggs, fresh fruits
- Immunization (infections worsen PEM)
- Food fortification
Key Exam Points
| Point | Detail |
|---|---|
| Type of malnutrition | PEM - calorie + protein deficiency |
| Hallmark | Severe wasting, NO oedema |
| Age group | <1 year |
| Pathophysiology | Adapted starvation - insulin suppressed, ketosis |
| Albumin | Normal/near-normal |
| Liver | NOT enlarged (unlike kwashiorkor) |
| Unique facial sign | Monkey facies (loss of buccal fat pads) |
| MUAC for severe malnutrition | <12.5 cm |
| Immune defect | T-cell-mediated immunity most affected |
| Refeeding risk | Hypophosphatemia |
Sources: Park's Textbook of Preventive and Social Medicine; Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Fitzpatrick's Dermatology
This is a shared conversation. Sign in to Orris to start your own chat.