Febrile neutropenia treatment
Reading File
Finding Sources
Searching PubMed
"febrile neutropenia" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from three major textbooks. Let me compile the full answer.
Febrile Neutropenia: Treatment
Definition
- Fever: single oral temperature ≥38.3°C (101°F), or ≥38.0°C (100.4°F) sustained for >1 hour
- Neutropenia: ANC <1000/mm³; severe <500/mm³; profound <100/mm³
Most commonly caused by chemotherapy, with nadir typically 5-10 days after the last dose.
Step 1 - Risk Stratification
Before choosing inpatient vs. outpatient treatment, classify risk using the MASCC Risk Index (available at mascc.org):
High-risk features (hospitalize with IV antibiotics):
- Profound neutropenia expected to last >7-10 days
- Inpatient at time of fever onset
- Hemodynamic instability / septic shock
- Acute leukemia or uncontrolled cancer
- Evidence of organ failure (renal, hepatic)
- Pneumonia, severe soft tissue infection, or central line infection
- Abdominal pain, neurologic changes, severe mucositis
Low-risk features (consider outpatient oral therapy):
- Neutropenia expected to resolve within 7 days
- No comorbid medical conditions
- Well-appearing, no peritoneal signs, normal CXR
- Low MASCC score
Step 2 - Initial Evaluation (within 60 minutes)
- Two blood cultures: one from each lumen of central venous catheter + one peripheral site (or two peripheral sites if no CVC)
- CBC, electrolytes, renal/hepatic function, serum lactate
- Urinalysis + urine culture
- Chest radiograph (note: poorly sensitive for infiltrates in neutropenia)
- Additional cultures (sputum, stool, wound) if clinically indicated
- CT chest/abdomen/pelvis if no source identified on routine workup
- Influenza PCR (in season) - rapid antigen test has insufficient sensitivity
- Consider C. difficile testing if diarrhea present
- Careful physical exam: mouth, sinuses, lungs, skin, perineum/anus, nail beds, all catheter sites. Avoid digital rectal exam until after first antibiotic dose
Step 3 - Empiric Antibiotic Therapy
Start within 60 minutes of presentation. No specific regimen has proven consistently superior; monotherapy is as effective as dual therapy in most cases.
Inpatient - Monotherapy (first-line)
| Agent | Dose |
|---|---|
| Piperacillin/tazobactam | 4.5 g IV q6h |
| Cefepime | 2 g IV q8h |
| Ceftazidime | 2 g IV q8h |
| Imipenem/cilastatin | 1 g IV q8h |
| Meropenem | 1 g IV q8h |
- Use pip/tazo, cefepime, or ceftazidime if no known MDR colonization
- Use imipenem or meropenem if known ESBL-producing organism colonization
- Pseudomonas coverage must always be included
When to Add Vancomycin (not routine)
Vancomycin is not routinely recommended for all febrile neutropenic patients due to the risk of VRE emergence. Add it for:
- Hemodynamic instability / septic shock
- Catheter-related infection with hypotension
- Skin or soft tissue infection (cellulitis)
- Known MRSA or penicillin-resistant pneumococcal colonization
- Positive blood culture for gram-positive organisms (before final ID/sensitivities)
- Severe mucositis with prior fluoroquinolone prophylaxis
- Institutions with high prevalence of MRSA, VSE, or S. mitis
Penicillin Allergy
- Minor allergy: Cefepime, meropenem, or imipenem/cilastatin can usually be given safely
- Severe/anaphylactic allergy: Aztreonam + vancomycin. Avoid empiric fluoroquinolones for gram-negative coverage in this setting
Source-Directed Additions
| Suspected Source | Add |
|---|---|
| Community-acquired pneumonia | Atypical coverage (azithromycin or fluoroquinolone) |
| Suspected Pneumocystis | Trimethoprim-sulfamethoxazole |
| Perianal, oral, or abdominal infection (typhlitis) | Metronidazole or clindamycin (if cefepime used, which lacks anaerobic coverage) |
| Herpes simplex or VZV (ulcerative/vesicular lesions) | Acyclovir |
| Influenza (clinical suspicion) | Oseltamivir empirically if PCR unavailable |
Outpatient (low-risk patients only)
Ciprofloxacin 500 mg PO q12h or Levofloxacin 750 mg PO daily, plus amoxicillin/clavulanate 500/125 mg PO q8h (or clindamycin 300 mg q8h for penicillin allergy). Requires daily reassessment by a medical provider for the first 3 days.
Step 4 - Antifungal Therapy
Up to one-third of febrile neutropenic patients who fail to respond after 7 days of antibiotics have systemic fungal infections (usually Candida or Aspergillus).
- Amphotericin B (or lipid formulations) is the drug of choice for invasive fungal infections
- Micafungin or voriconazole may be used for specific fungal pathogens (preferred when amphotericin toxicity is a concern)
Step 5 - Duration of Therapy
- Median fever duration after starting antibiotics: ~2 days (low-risk) vs. 5-7 days (high-risk)
- Reassess at 2-4 days before changing regimen (earlier if clinical deterioration or culture results)
- Continue antibiotics until:
- Documented infection has clinically resolved AND
- Patient has been afebrile for ≥2 days AND
- ANC has recovered to >500/mm³
Step 6 - Antibiotic De-escalation
A 2025 meta-analysis (PMID 40079575) in Antimicrobial Agents and Chemotherapy found that early antibiotic de-escalation in febrile neutropenia for patients with hematologic malignancy is safe and does not increase mortality - supporting de-escalation once cultures and clinical response are available.
Special Populations
Children with cancer and febrile neutropenia: Principles are similar. Risk stratification is mandatory before deciding inpatient vs. outpatient. Consult the MASCC pediatric criteria; clinical judgment and oncologist guidance are especially important.
Septic patient: Rapid IV fluids and maintain MAP ≥65 mmHg as immediate priority before antibiotic workup is complete.
Sources: Tintinalli's Emergency Medicine, p. 1559; Rosen's Emergency Medicine, p. 3478; Goldman-Cecil Medicine, p. 3132
How sildinafil can be used for ED in diabetes patients
Reading File
Finding Sources
Finding Sources
Searching PubMed
"sildenafil" AND "erectile dysfunction" AND "diabetes"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the content needed for a thorough answer. Here it is:
Sildenafil for Erectile Dysfunction in Diabetic Men
Why Diabetes Causes ED
ED in diabetes is multifactorial and more severe than in the general population:
- Prevalence: Men with type 2 DM develop ED approximately 3× more frequently than the general population, and ED can be the presenting symptom of undiagnosed diabetes - Smith & Tanagho's General Urology, p. 625
- Mechanisms: Diabetes damages multiple systems simultaneously:
- Microvascular disease - small vessel damage to cavernous arteries reduces arterial inflow
- Cavernous nerve terminal damage - autonomic neuropathy impairs neurogenic NO release
- Endothelial dysfunction - reduced eNOS activity, decreased NO production
- Smooth muscle changes - cavernous smooth muscle fibrosis and reduced relaxation capacity
- Veno-occlusive dysfunction - impaired compression of penile venous plexus
- The net result: decreased responsiveness to PDE5 inhibitors due to the combined neurovascular damage - Smith & Tanagho's, p. 625
Mechanism of Action of Sildenafil
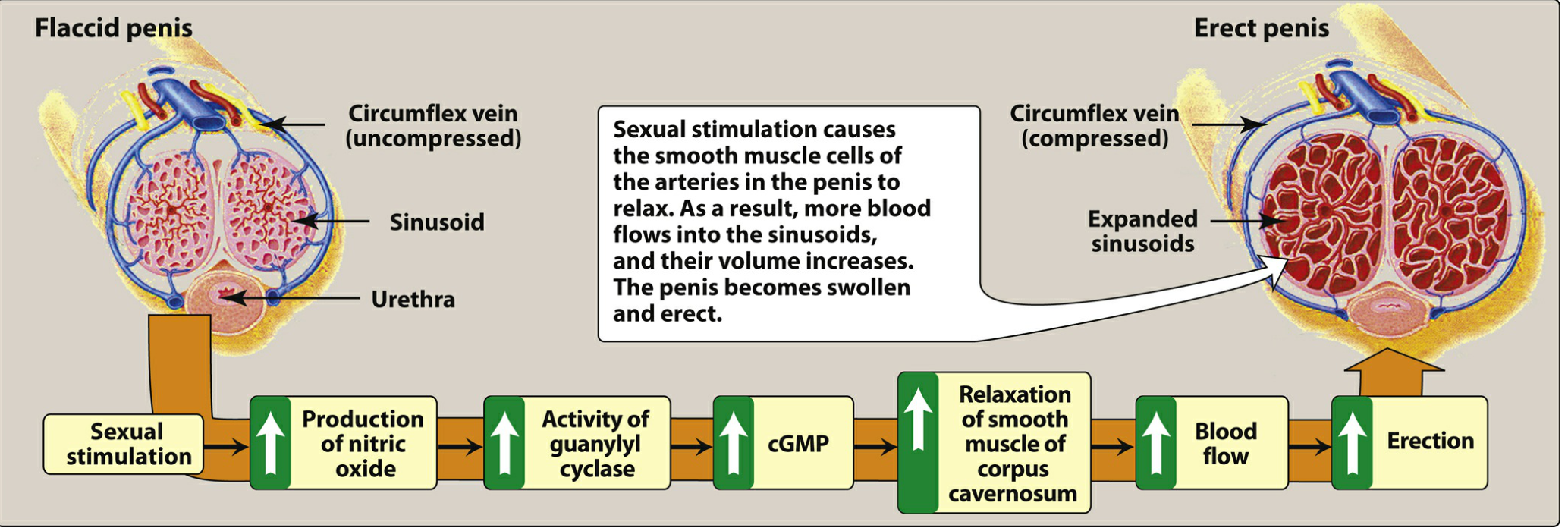
Figure: Mechanism of penile erection - Lippincott Illustrated Reviews: Pharmacology
- Sexual stimulation triggers nitric oxide (NO) release in the corpus cavernosum
- NO activates guanylyl cyclase → converts GTP to cGMP
- cGMP causes smooth muscle relaxation via reduced intracellular Ca²⁺ → increased blood inflow → erection
- PDE-5 normally degrades cGMP, terminating erection
- Sildenafil inhibits PDE-5 → prevents cGMP degradation → prolongs and amplifies the erectile response
Key point: Sildenafil has no effect in the absence of sexual stimulation - it enhances, not initiates, the physiological process. - Lippincott Pharmacology, p. 1459
Sildenafil Dosing and Pharmacokinetics
| Parameter | Detail |
|---|---|
| Approved doses | 25 mg, 50 mg, 100 mg |
| Starting dose | 50 mg (25 mg in elderly, renal/hepatic impairment) |
| Timing | ~1 hour before anticipated sexual activity |
| Duration of effect | Up to 4 hours |
| Food interaction | High-fat meal delays absorption - take on empty stomach or light meal |
| Metabolism | CYP3A4 (hepatic) |
| Dose adjustment | Reduce in mild-moderate hepatic dysfunction; reduce in severe renal dysfunction |
Efficacy in Diabetic Patients
Sildenafil is effective and recommended as first-line for ED in diabetic men, but with important caveats:
- Efficacy is lower than in non-diabetic men: Sildenafil fails to produce adequate erections in approximately 50% of men with long-standing, insulin-dependent diabetes compared to a ~25-30% failure rate in the general ED population - Kaplan & Sadock's Comprehensive Textbook, p. 6140
- Despite this, it remains the first-line pharmacological treatment alongside the other PDE5 inhibitors
- Systematic reviews confirm efficacy of sildenafil citrate for ED in men with diabetes mellitus - Campbell-Walsh Wein Urology, p. 185
Why response is blunted in diabetes:
- Diabetic neuropathy reduces the neurogenic NO signal that sildenafil depends on to amplify
- Endothelial dysfunction reduces the eNOS contribution to NO
- Advanced glycation end-products impair smooth muscle relaxation
- The longer the duration and poorer the control of diabetes, the lower the response rate
Clinical Use in Diabetic Patients
Before Starting
- Check fasting glucose and HbA1c (better glycemic control improves ED outcomes)
- Lipid profile (dyslipidemia worsens vasculogenic ED)
- Morning testosterone (calculated free T) - hypogonadism is common in type 2 DM and reduces PDE5i response; replace testosterone if low
- Cardiovascular risk assessment is mandatory - diabetic men are at high cardiovascular risk; assess whether sexual activity is safe (must be able to perform ≥6 METs without symptoms)
- Use IIEF-5 questionnaire for baseline severity scoring - Smith & Tanagho's, p. 626
Contraindications
| Contraindication | Reason |
|---|---|
| Concurrent organic nitrates (nitroglycerin, isosorbide) | Synergistic hypotension - potentially fatal BP drop |
| Severe hepatic impairment | Markedly elevated drug levels |
| Recent MI, stroke, or life-threatening arrhythmia (within 6 months) | Cardiovascular risk of sexual activity |
| Severe hypotension or uncontrolled hypertension | Hemodynamic instability |
| Retinitis pigmentosa | Risk of optic complications |
Note for diabetic patients: Many diabetics take antihypertensives - additive hypotension may occur. Start at 25 mg. Many diabetic patients with angina may be on nitrates, which is an absolute contraindication.
Key Adverse Effects
- Headache (most common), flushing, dyspepsia, nasal congestion
- Visual disturbance - blue-tinted vision (cyanopsia) due to mild PDE-6 inhibition in the retina; transient
- Nonarteritic anterior ischemic optic neuropathy (NAION) - rare but serious; avoid in patients with optic pathology
- Sudden hearing loss - rare association
When Sildenafil Alone is Insufficient in Diabetes
Because diabetic ED is frequently refractory to monotherapy, combination and step-up strategies are used:
Optimize Glycemic Control First
Poor glycemic control worsens vascular and neural damage. Improving HbA1c can improve ED independent of medication.
Testosterone Replacement + Sildenafil
Men with type 2 DM often have low testosterone. Combining testosterone replacement therapy with PDE5 inhibitors significantly improves response in hypogonadal men who fail PDE5i monotherapy - Campbell-Walsh, Combination Therapies section
Alternative PDE5 Inhibitors
- Tadalafil (Cialis): longer half-life (~18 hours), effective for up to 36 hours, once-daily dosing option (5 mg/day) available - avoids timing pressure and may provide more consistent coverage; food does not affect absorption
- Vardenafil, Avanafil: similar efficacy to sildenafil; avanafil has fastest onset (30 min)
Intracavernosal Injection (alprostadil)
- Acts locally, independent of the neurogenic NO pathway
- Can produce erections without sexual stimulation
- Prostaglandin E1 - direct cavernous smooth muscle relaxant
- Useful in diabetic men who fail oral PDE5 inhibitors due to severe autonomic neuropathy
Combination Therapy Options
- Oral PDE5i + intracavernous alprostadil
- Oral PDE5i + vacuum erection device
- Oral PDE5i + transurethral alprostadil (MUSE)
- Tadalafil 5 mg daily + sildenafil 50 mg on-demand (for partial responders) - Campbell-Walsh, Combination Therapies
Low-Intensity Extracorporeal Shockwave Therapy (Li-ESWT)
A 2026 RCT (PMID 41933953) confirmed Li-ESWT and pelvic floor muscle training each mitigate ED in men with diabetes. Diabetic animal model data shows Li-ESWT promotes regeneration of nerves, endothelium, and smooth muscle - which addresses the root pathology rather than just augmenting NO signaling - Campbell-Walsh, Alternative Therapies
Penile Prosthesis
For complete non-responders to all medical therapies. Arterial revascularization surgery is not recommended in diabetic men (diabetes is an exclusion criterion for arterial surgery due to diffuse vasculopathy) - Campbell-Walsh, p. 953
Summary: Step-Up Approach in Diabetic ED
- Lifestyle + glycemic optimization - weight loss, HbA1c control, stop smoking
- Check testosterone - replace if hypogonadal before or alongside PDE5i
- Sildenafil 50 mg (or other PDE5i) on demand - titrate to 100 mg if tolerated and needed
- Switch or add: tadalafil daily dosing, or combine with testosterone replacement
- Intracavernosal alprostadil or vacuum erection device if PDE5i fails
- Combination therapies (PDE5i + alprostadil, PDE5i + VED)
- Penile prosthesis for refractory cases
Sources: Lippincott Illustrated Reviews: Pharmacology, p. 1459; Smith & Tanagho's General Urology 19e, p. 625-626; Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 6140-6141; Campbell-Walsh Wein Urology, Combination Therapies & Alternative Therapies sections; Textbook of Family Medicine 9e, p. 1194
This is a shared conversation. Sign in to Orris to start your own chat.