Explain me the following topics from k.d. tripathi starting from basics
Asking for Preferences
Gout
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a thorough explanation. Here is the complete, structured explanation of Gout pharmacology - aligned with K.D. Tripathi's approach and supplemented from Katzung, Goodman & Gilman, and Lippincott:
GOUT - Complete Pharmacology (K.D. Tripathi Style)
1. What is Gout?
Gout is a metabolic disease characterized by recurrent episodes of acute arthritis caused by the deposition of monosodium urate (MSU) crystals in joints and surrounding tissues. It is directly associated with hyperuricemia (elevated serum uric acid).
Key features:
- Acute inflammatory arthritis (classically big toe - "podagra")
- Tophi (urate crystal deposits in soft tissues, bones, cartilage)
- Uric acid renal calculi (kidney stones)
- Interstitial nephritis
- Adverse cardiovascular outcomes
Risk factors: Male sex, diuretic use, alcohol, obesity, hypertension, high-purine diet (red meat, seafood), sweetened beverages, renal disease.
2. Pathophysiology (Why Uric Acid Rises & Why It Causes Pain)
Uric acid is the end product of purine metabolism in humans. Unlike most mammals, humans lack the enzyme uricase (which converts uric acid to the more soluble allantoin), so uric acid accumulates.
Why Does Hyperuricemia Occur?
- Underexcretion of urate (most common, ~90% of cases) - renal handling defect
- Overproduction of urate (~10%) - increased purine turnover (e.g., malignancies, hemolysis)
Normal serum urate ~5 mg/dL approaches the limit of solubility. Beyond this, MSU crystals precipitate, especially in colder, more acidic joints (peripheral joints, big toe).
Inflammatory Cascade (The Key Pharmacology Target):
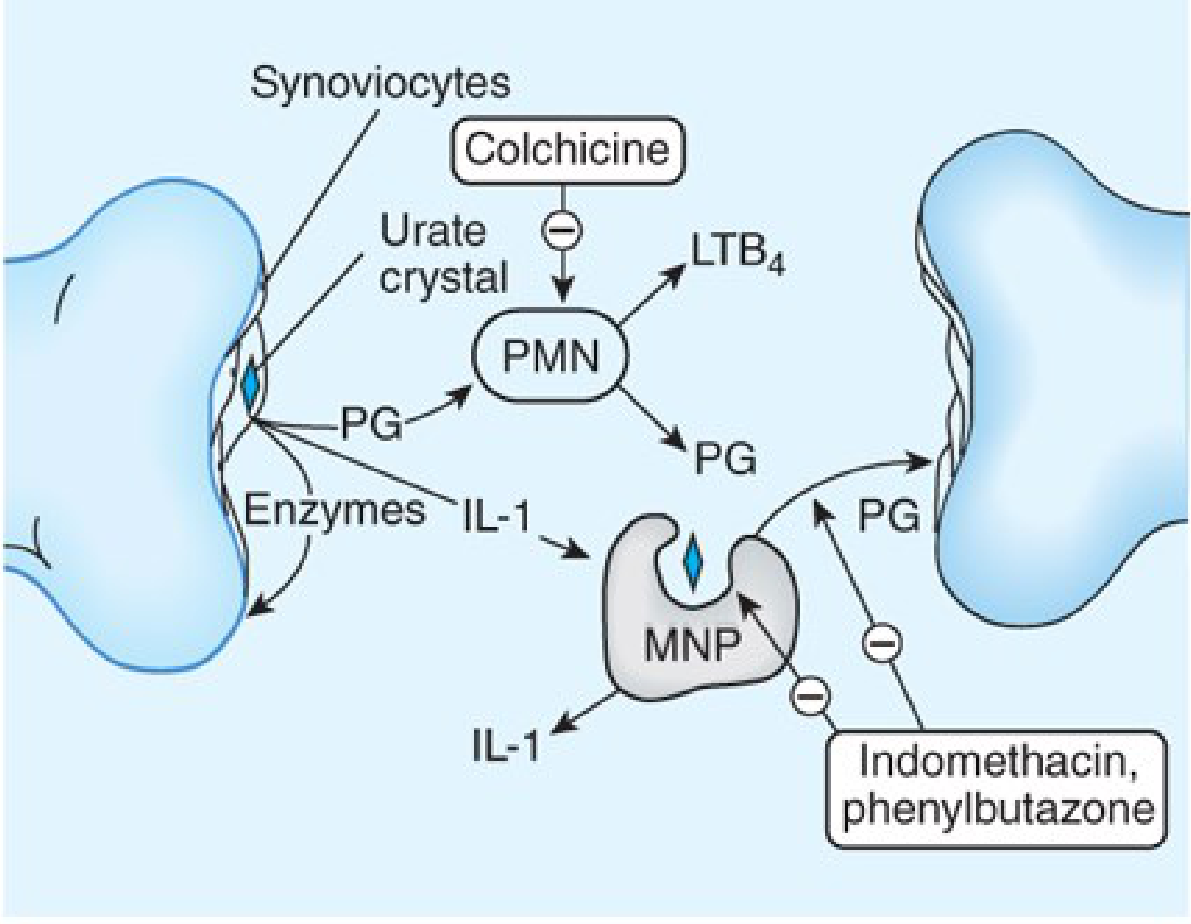
- MSU crystals are phagocytosed by synoviocytes and monocytes/macrophages (via toll-like receptors)
- This activates the NLRP3 inflammasome → releases IL-1β and TNF-α
- Synoviocytes release prostaglandins (PG), lysosomal enzymes, leukotriene B4 (LTB4)
- These act as chemotactic mediators → attract PMNs (neutrophils) into the joint
- PMNs phagocytose more crystals → release more PG, IL-1 → amplify inflammation
- Later, mononuclear phagocytes (macrophages) arrive, ingest crystals, release more mediators
This self-amplifying cycle causes the exquisitely painful acute attack.
3. Treatment Goals
- Relieve the acute attack (pain + inflammation)
- Prevent recurrent attacks (prophylaxis)
- Lower serum urate levels (urate-lowering therapy)
4. Drugs Used in Gout
PART A - Drugs for ACUTE GOUT Attack
A1. NSAIDs
First-line for acute gout. Indomethacin is the classic NSAID of choice, though all NSAIDs are likely effective.
Mechanism: Inhibit COX-1 and COX-2 → reduce prostaglandin synthesis → decrease inflammation and pain.
Dose: High-dose indomethacin (50 mg 3 times daily) for 3-5 days, then taper.
Adverse Effects: GI irritation, peptic ulcer, renal impairment, fluid retention.
Contraindication: Avoid in renal failure, peptic ulcer disease.
A2. Colchicine
Colchicine is a plant alkaloid from the autumn crocus (Colchicum autumnale) - one of the oldest known therapies for gout (used since ~1500 BCE).
Mechanism of Action:
- Binds to tubulin (microtubular protein) → causes depolymerization of microtubules
- Disrupts neutrophil migration and function
- Reduces neutrophil recruitment into the inflamed joint (impairs chemotaxis)
- Blocks NLRP3 inflammasome activation → prevents IL-1β and IL-18 release
- Blocks cell division by disrupting mitotic spindles
- Not a uricosuric and not an analgesic - it is purely anti-inflammatory
Important: Colchicine must be given within 36 hours of onset of attack to be effective. It usually alleviates pain within 12 hours.
Pharmacokinetics:
- Well absorbed orally; peak plasma concentration in 0.5-2 hours
- Metabolized by CYP3A4 (hepatic); substrate of P-glycoprotein
- Enterohepatic recirculation
- 40-65% excreted unchanged in urine
- Half-life ~31 hours
- NOT removed by hemodialysis
Dose (Acute): Low-dose regimen - 1.2 mg initially, then 0.6 mg 1 hour later. Low-dose is as effective as high-dose but with fewer GI side effects.
Dose (Prophylaxis): 0.5-0.6 mg once or twice daily.
Adverse Effects:
- GI toxicity (most common): nausea, vomiting, abdominal pain, diarrhea - dose-limiting
- Bone marrow suppression: agranulocytosis, aplastic anemia (chronic use)
- Myopathy and neuropathy (chronic use)
- Alopecia (hair loss)
- Contraindicated in hepatic/renal impairment when used with CYP3A4 inhibitors
Drug Interactions:
- CYP3A4 inhibitors (e.g., clarithromycin, ketoconazole) increase colchicine levels - risk of toxicity
- P-glycoprotein inhibitors (e.g., cyclosporine) - increased toxicity
A3. Glucocorticoids
Used when NSAIDs and colchicine are contraindicated (e.g., renal failure).
Route: Intra-articular injection (when 1-2 joints affected) OR systemic oral/IV (widespread involvement).
Mechanism: Inhibit phospholipase A2 → reduce arachidonic acid release → decrease prostaglandin and leukotriene synthesis. Also inhibit COX-2 expression. Reduce IL-1β production.
Examples: Triamcinolone, methylprednisolone, prednisone.
Adverse effects: Hyperglycemia, hypertension, osteoporosis (with long-term use).
A4. IL-1 Inhibitors (Biologics)
Used in patients who fail or cannot tolerate NSAIDs, colchicine, and corticosteroids.
- Canakinumab (anti-IL-1β monoclonal antibody) - approved in Europe for refractory gout
- Anakinra (IL-1 receptor antagonist) - used off-label
Mechanism: Block IL-1β, a key cytokine in the NLRP3 inflammasome-mediated gouty inflammation.
PART B - Drugs for CHRONIC GOUT (Urate-Lowering Therapy / ULT)
Important principle: ULT should NOT be started during an acute attack. Initiating ULT can actually precipitate a new attack due to rapid changes in serum urate. When starting ULT, always co-prescribe prophylactic colchicine or NSAIDs for at least 6 months.
Indication for ULT: >2 gouty attacks/year, chronic kidney disease, kidney stones, or tophi.
Target serum uric acid: <6 mg/dL (for most patients) or <5 mg/dL (for tophaceous gout).
B1. Allopurinol (Xanthine Oxidase Inhibitor)
First-line ULT and the most widely used drug for chronic gout.
Mechanism:
- Allopurinol is a purine analogue (isomer of hypoxanthine)
- Competitively inhibits xanthine oxidase - the enzyme responsible for converting hypoxanthine → xanthine → uric acid
- Result: serum urate levels fall; the less soluble uric acid is replaced by the more soluble xanthine and hypoxanthine
- Allopurinol is itself metabolized by xanthine oxidase to alloxanthine (oxypurinol), which is also a xanthine oxidase inhibitor (prolonging the action)
Pharmacokinetics:
- Oral, ~80% absorbed
- Half-life of allopurinol: 1-2 hours (short)
- Half-life of alloxanthine (active metabolite): 15-18 hours → allows once-daily dosing
- Renally cleared - dose adjustment needed if GFR <30 mL/min
Starting Dose: 100 mg/day; titrate up by 100 mg every 2-5 weeks until uric acid <6 mg/dL (maximum 800 mg/day).
Adverse Effects:
- Skin rash (most common, ~3%) - stop immediately at first sign
- GI intolerance (nausea, vomiting, diarrhea)
- Allopurinol Hypersensitivity Syndrome (AHS) - rare but LETHAL: Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), eosinophilia, fever, hepatitis, renal failure. Occurs within 2-4 weeks.
- Peripheral neuritis, bone marrow suppression, aplastic anemia (rare)
HLA-B*5801 Alert: Patients of Han Chinese, Korean, or Thai descent have a high prevalence of the HLA-B*5801 allele, which dramatically increases risk of AHS. FDA recommends genetic screening before starting allopurinol in these populations.
Key Drug Interactions:
- Azathioprine / 6-mercaptopurine: Both are metabolized by xanthine oxidase. Allopurinol blocks their metabolism → toxic accumulation → reduce dose by 75%
- Cyclophosphamide: Allopurinol increases its effect (bone marrow toxicity)
- Oral anticoagulants (warfarin): Allopurinol inhibits their metabolism → increased bleeding risk
- Probenecid: Allopurinol inhibits probenecid metabolism
- Do NOT stop allopurinol during an acute flare (can worsen and prolong the attack)
B2. Febuxostat (Xanthine Oxidase Inhibitor)
A non-purine, selective xanthine oxidase inhibitor - structurally unrelated to allopurinol.
Mechanism: Selectively inhibits xanthine oxidase (both oxidized and reduced forms) → reduces uric acid synthesis.
Advantage over allopurinol:
- Does not have the same degree of renal elimination → less dose adjustment needed in mild-to-moderate renal impairment
- May have reduced risk of rash and hypersensitivity reactions compared to allopurinol
Disadvantage:
- Associated with greater cardiovascular risk (heart attack, stroke) compared to allopurinol (per CARES trial)
- Reserved for patients who cannot tolerate or have contraindications to allopurinol
- Use with caution in history of heart disease or stroke
Dose: 40-80 mg once daily.
B3. Probenecid (Uricosuric Agent)
Mechanism:
- Weak organic acid
- Inhibits the URAT-1 urate-anion exchanger in the proximal renal tubule
- Blocks reabsorption of uric acid → increased urinary excretion of uric acid (uricosuria)
- At low doses paradoxically inhibits secretion (not used therapeutically)
Indications: Underexcretors of uric acid; used when xanthine oxidase inhibitors are not tolerated.
Adverse Effects:
- Uric acid kidney stones (must maintain high fluid intake and alkalinize urine)
- GI upset
- Hypersensitivity reactions
Contraindications:
- Renal failure (GFR <50 mL/min) - ineffective
- History of uric acid kidney stones
- Overproducers of uric acid (risk of stones)
Drug Interactions:
- Inhibits tubular secretion of many drugs (penicillin - historically used to prolong penicillin levels), methotrexate, NSAIDs
- Aspirin (even low-dose) blocks probenecid's uricosuric effect - avoid combination
B4. Pegloticase (Recombinant Uricase)
Mechanism:
- Recombinant pegylated uricase (polyethylene glycol-conjugated uricase)
- Converts uric acid → allantoin (highly soluble, easily excreted)
- Dramatically reduces serum uric acid
Used for: Severe, refractory, tophaceous gout unresponsive to conventional therapy.
Route: IV infusion every 2 weeks.
Adverse Effects:
- Anaphylaxis and infusion reactions (major concern - monitor closely)
- Risk of gout flares during initiation
- Development of anti-drug antibodies (reduces efficacy over time)
B5. Rasburicase
- Recombinant uricase; given IV
- Used primarily for tumor lysis syndrome (not chronic gout management)
- Contraindicated in G6PD deficiency (can cause severe hemolysis)
5. Summary Table
| Drug | Class | Mechanism | Use |
|---|---|---|---|
| Indomethacin | NSAID | COX inhibitor | Acute attack (first-line) |
| Colchicine | Alkaloid | Anti-tubulin, NLRP3 inhibitor | Acute + prophylaxis |
| Glucocorticoids | Steroid | Phospholipase A2 inhibition | Acute (if NSAIDs/colchicine CI) |
| Canakinumab | Biologic | Anti-IL-1β | Refractory acute |
| Allopurinol | Xanthine oxidase inhibitor | Blocks uric acid synthesis | Chronic (first-line ULT) |
| Febuxostat | Xanthine oxidase inhibitor | Blocks uric acid synthesis | Chronic (if allopurinol CI) |
| Probenecid | Uricosuric | Blocks tubular reabsorption of urate | Chronic (underexcretors) |
| Pegloticase | Recombinant uricase | Converts urate → allantoin | Refractory tophaceous gout |
6. Key Clinical Pearls (Exam Points)
- Never start ULT during acute attack - it can precipitate or worsen the flare
- When starting allopurinol, always co-prescribe colchicine prophylaxis for ≥6 months
- Do not stop allopurinol if a flare occurs during therapy - continue and treat the flare
- Colchicine must be given within 36 hours of attack onset
- Allopurinol + azathioprine = reduce azathioprine dose by 75% (or deadly toxicity)
- Low-dose aspirin blocks the uricosuric effect of probenecid
- Probenecid is ineffective if GFR <50 mL/min
- Febuxostat has a cardiovascular safety warning - prefer allopurinol as first-line
- Screen Han Chinese/Korean/Thai patients for HLA-B*5801 before prescribing allopurinol
- Rasburicase is contraindicated in G6PD deficiency
- Thiazide and loop diuretics raise serum uric acid (increase gout risk)
- Low-dose losartan and fenofibrate have mild uricosuric properties (used off-label)
Sources: Katzung's Basic & Clinical Pharmacology 16e; Goodman & Gilman's Pharmacological Basis of Therapeutics; Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.