Next investigation if INR is raised
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a structured approach to investigating a raised INR (prolonged PT/INR):
Raised INR — Next Investigations
Understanding What the PT/INR Measures
The PT (reported as INR) reflects the extrinsic and common pathways: Factor VII, Factor X, Factor V, prothrombin (Factor II), and fibrinogen.
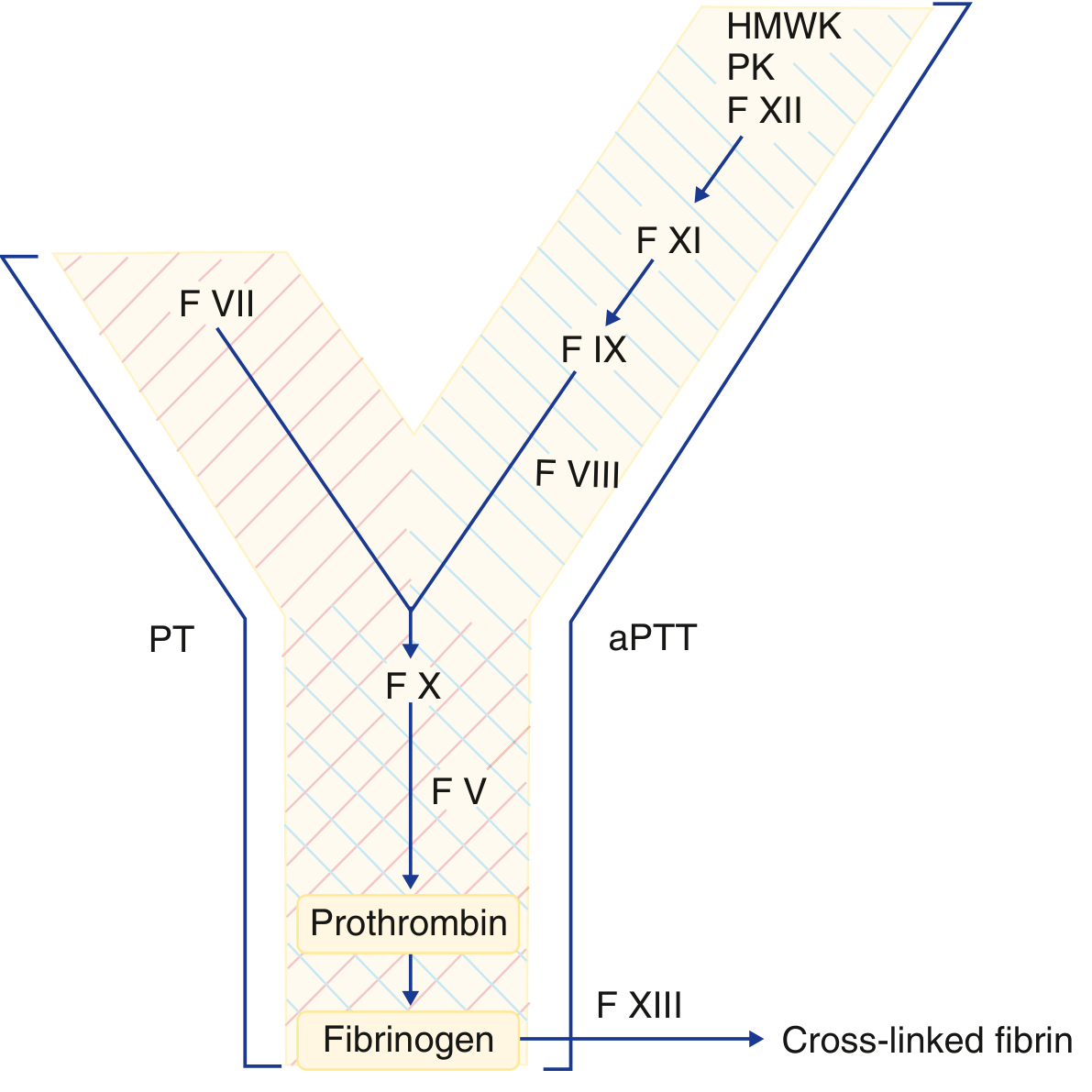
Step 1: Check the aPTT
This is the critical first step. The pattern of PT vs aPTT narrows the differential:
| PT (INR) | aPTT | Likely Cause |
|---|---|---|
| ↑ | Normal | Factor VII deficiency; early vitamin K deficiency; early liver disease |
| ↑ | ↑ | Common pathway defect (FV, FX, FII, fibrinogen); DIC; severe liver disease; vitamin K deficiency (advanced); warfarin; supratherapeutic heparin |
| Normal | ↑ | Intrinsic pathway defect (FVIII, FIX, FXI — haemophilia A/B; vWD); lupus anticoagulant |
Step 2: Mixing Study (1:1 Mix)
Mix patient plasma 1:1 with normal pooled plasma, then re-run the PT:
- Corrects → factor deficiency (the normal plasma supplies the missing factor to 50%, which is sufficient for clotting)
- Proceed to individual factor assays (FVII, FX, FV, FII, fibrinogen depending on aPTT result)
- Does NOT correct → inhibitor present (an antibody is interfering with coagulation in both the patient's and normal plasma)
- Proceed to inhibitor identification (specific factor antibody, e.g. anti-FVIII; or lupus anticoagulant testing)
Step 3: Targeted Follow-Up Tests
If factor deficiency (mixing study corrects):
- Individual factor assays: FVII (if aPTT normal), or FX, FV, FII (if both PT and aPTT raised)
- Fibrinogen level (functional/clottable + antigenic) — if Thrombin Time (TT) also prolonged
- Vitamin K levels / response to vitamin K administration
- Liver function tests — liver produces all coagulation factors (except FVIII)
- Consider DIC screen: fibrinogen, D-dimer, platelet count, peripheral blood film
If inhibitor suspected (mixing study does not correct):
- Factor VIII inhibitor assay (Bethesda assay) — most common acquired inhibitor
- Lupus anticoagulant screen: dilute Russell's viper venom time (dRVVT), Silica clotting time
Additional tests based on clinical context:
- LFTs + synthetic function (albumin, bilirubin) — liver disease
- Vitamin K status — nutritional, malabsorption (coeliac screen, faecal elastase), broad-spectrum antibiotics
- Drug history — warfarin, broad-spectrum antibiotics disrupting gut flora
- FBC + film — DIC (thrombocytopenia, schistocytes), haematological malignancy
- TT (Thrombin Time) — prolonged in fibrinogen deficiency, dysfibrinogenaemia, heparin effect
Common Causes to Guide Investigation
| Cause | Key Distinguishing Tests |
|---|---|
| Warfarin / anticoagulant drugs | Drug history; corrects with vitamin K |
| Liver disease | LFTs, albumin; both PT and aPTT raised |
| Vitamin K deficiency | Nutritional Hx; responds to IV vitamin K |
| DIC | D-dimer ↑↑, fibrinogen ↓, platelets ↓ |
| Isolated FVII deficiency | aPTT normal; FVII assay |
| Acquired inhibitor | Mixing study does not correct |
| Dysfibrinogenaemia | Prolonged TT; discordant clottable vs antigenic fibrinogen |
Sources: Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E (2025)
This is a shared conversation. Sign in to Orris to start your own chat.