Define sepsis Describe the anatomy and physiology involved in the body's response to infection. Explain the pathophysiology of sepsis and septic shock. Identify the causes, risk factors, signs, and symptoms of sepsis. Discuss the diagnostic tests used to confirm sepsis. Explain the medical and nursing management of patients with sepsis. Recognize the complications of sepsis and methods of prevention. Understand the role of nurses in early detection and timely intorontion to improuo pationt outcomor
Reading File
Finding Sources
Searching PubMed
sepsis AND "septic shock" AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed response.
Sepsis: A Comprehensive Clinical Overview
1. Definition of Sepsis
Sepsis is defined as a life-threatening organ dysfunction caused by a dysregulated host response to infection. This is the Sepsis-3 definition (2016), which replaced the older SIRS-based definition that was felt to be too nonspecific.
- Organ dysfunction in Sepsis-3 is identified as an increase in the Sequential Organ Failure Assessment (SOFA) score of ≥2 points from baseline, indicating that the infection has caused measurable end-organ harm.
- Septic shock is a subset of sepsis characterized by persistent hypotension requiring vasopressors to maintain a mean arterial pressure (MAP) ≥65 mmHg, despite adequate volume resuscitation, and a serum lactate >2 mmol/L. Mortality in septic shock approaches 40%.
- The older SIRS (Systemic Inflammatory Response Syndrome) criteria are no longer the primary definition but remain clinically useful as screening tools. SIRS requires ≥2 of: temperature >38°C or <36°C, heart rate >90 bpm, respiratory rate >20 breaths/min or PaCO2 <32 mmHg, WBC >12,000 or <4,000 cells/μL.
Washington Manual of Medical Therapeutics, p. 295
2. Anatomy and Physiology of the Body's Response to Infection
The Innate Immune System
When pathogens invade, the body's first line of defense involves pattern recognition receptors that detect molecular signatures of microbes:
- Toll-like receptors (TLRs) on macrophages and neutrophils recognize pathogen-associated molecular patterns (PAMPs) such as lipopolysaccharide (LPS) on gram-negative bacteria.
- G-protein-coupled receptors detect bacterial peptides.
- C-type lectin receptors (dectins) recognize fungal cell wall components.
Cellular Responders
- Neutrophils and monocytes/macrophages are the primary effector cells, releasing cytokines (TNF-α, IL-1β, IL-6, IL-12, IL-18), reactive oxygen species (ROS), prostaglandins, and platelet-activating factor (PAF).
- The complement system is activated by microbial components, producing anaphylatoxins (C3a, C5a), chemotactic factors (C5a), and opsonins (C3b) that amplify inflammation.
Vascular Physiology
Under normal infection responses, vasodilation and increased capillary permeability deliver immune cells to the site of infection. Controlled cytokine signaling recruits leukocytes, opsonizes pathogens, and clears infection without systemic spread. The coagulation system also plays a protective role by walling off infected foci.
Robbins & Kumar Basic Pathology, p. 97
3. Pathophysiology of Sepsis and Septic Shock
The pathophysiology of septic shock is complex, involving four major interconnected mechanisms:
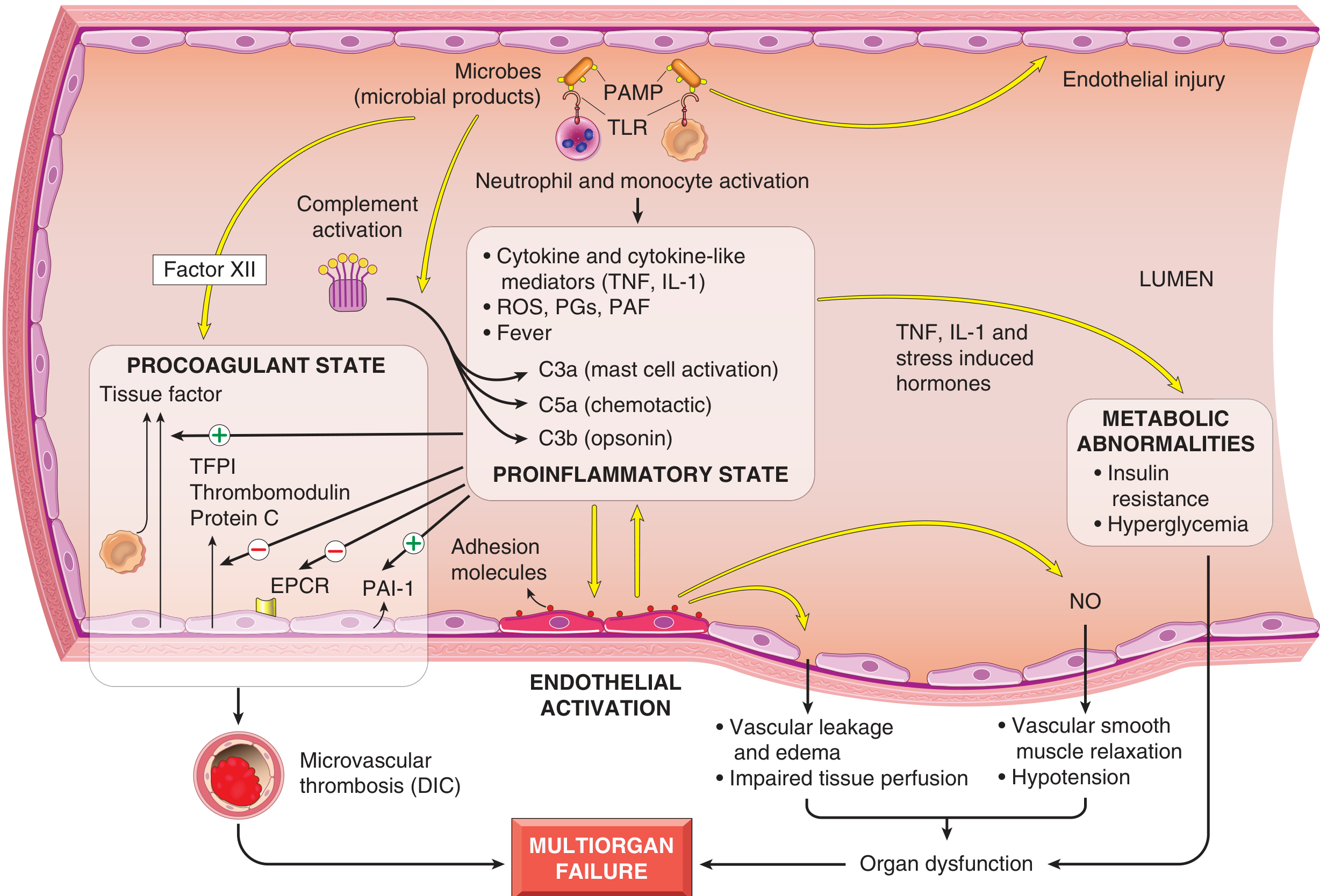
Fig. 3.19 - Major pathogenic pathways in septic shock (Robbins & Kumar Basic Pathology)
A. Inflammatory and Counter-inflammatory Responses
- Microbial products trigger massive, dysregulated cytokine release (TNF-α, IL-1β), far exceeding what is needed to clear the infection - this is the "cytokine storm."
- Pro-inflammatory cytokines cause fever, upregulate adhesion molecules on endothelium, and activate neutrophils.
- With time, the initial hyperinflammatory state triggers counterregulatory immunosuppression via a shift from Th1 to Th2 cytokines, production of IL-10 and IL-1 receptor antagonist, and lymphocyte apoptosis. Patients oscillate between hyperinflammatory and immunosuppressed states.
B. Endothelial Activation and Injury
- Inflammatory cytokines loosen tight junctions between endothelial cells, causing widespread vascular leakage and protein-rich edema throughout the body.
- This impedes tissue perfusion and nutrient delivery.
- Activated endothelium upregulates nitric oxide (NO) production via inducible NO synthase (iNOS), causing vascular smooth muscle relaxation, systemic vasodilation, and hypotension.
- The result is distributive (vasogenic) shock: high cardiac output with low systemic vascular resistance.
C. Induction of a Procoagulant State
- Proinflammatory cytokines increase tissue factor production by monocytes and endothelial cells.
- They simultaneously reduce anticoagulant factors: tissue factor pathway inhibitor (TFPI), thrombomodulin, and endothelial protein C receptor are all downregulated.
- Fibrinolysis is dampened by increased plasminogen activator inhibitor-1 (PAI-1).
- Vascular stasis from edema and vasodilation further promotes clotting.
- The result is disseminated intravascular coagulation (DIC) in up to 50% of cases: widespread microvascular thrombosis consumes clotting factors and platelets, causing paradoxical bleeding.
D. Metabolic Abnormalities
- TNF-α, IL-1, stress hormones (glucagon, growth hormone, glucocorticoids), and catecholamines drive gluconeogenesis.
- Proinflammatory cytokines suppress insulin release and promote insulin resistance (impaired GLUT-4 expression), producing hyperglycemia.
- Mitochondrial dysfunction from oxidative stress impairs cellular oxygen utilization, producing lactic acidosis even when oxygen delivery appears adequate (cytopathic hypoxia).
E. Cardiovascular Depression
Septic shock causes three primary hemodynamic effects:
- Hypovolemia (absolute from GI losses/sweating, and relative from vasodilation and capillary leak into third spaces).
- Direct myocardial depression - TNF-α, IL-1β, and NO impair contractility; global longitudinal strain on echocardiography shows dysfunction early even before frank ejection fraction reduction.
- Systemic inflammation driving multiorgan failure through microvascular and mitochondrial dysfunction.
F. Stages of Shock
| Stage | Features |
|---|---|
| Nonprogressive | Compensatory mechanisms activated (baroreceptors, catecholamines, RAAS, ADH); tachycardia, vasoconstriction, warm/flushed skin in early septic shock |
| Progressive | Widespread tissue hypoxia; aerobic respiration fails; anaerobic glycolysis produces lactic acid; metabolic acidosis; multiorgan hypoperfusion |
| Irreversible | Cellular injury so severe that even correcting hemodynamics cannot ensure survival; multiorgan failure and death |
Robbins & Kumar Basic Pathology, pp. 97-98; Rosen's Emergency Medicine; Sabiston Textbook of Surgery
4. Causes, Risk Factors, Signs, and Symptoms
Causes
Sepsis can result from infection with any microorganism. A specific organism is not identified in at least half of cases. Common causative organisms and sources include:
| Source | Typical Pathogens |
|---|---|
| Pneumonia (most common) | S. pneumoniae, Klebsiella, Pseudomonas, S. aureus |
| Urinary tract | E. coli, Klebsiella, Enterococcus |
| Abdominal/GI | E. coli, Bacteroides, Enterococcus |
| Skin/soft tissue | S. aureus (including MRSA), Streptococcus |
| Bloodstream (catheter-related) | Coagulase-negative Staph, Candida |
| Gram-negative (hospital-acquired) | E. coli, Klebsiella, Pseudomonas, Acinetobacter |
- Gram-positive organisms represent the leading cause of sepsis in hospitalized patients.
- Gram-negative LPS is the classic model of sepsis induction, though the pathophysiology cannot be explained by LPS alone.
- Fungal sepsis (Candida, Aspergillus) is increasingly common in immunocompromised patients.
Risk Factors
- Age extremes (elderly, neonates)
- Immunosuppression (HIV/AIDS, chemotherapy, steroids, organ transplant)
- Chronic diseases (diabetes, liver cirrhosis, chronic kidney disease, COPD, malignancy)
- Invasive devices (IV catheters, urinary catheters, mechanical ventilation)
- Major surgery or trauma
- Burns
- Malnutrition
- Hospital-acquired infections
Signs and Symptoms
Early/Warm Phase (Hyperdynamic State):
- Fever (>38°C) or hypothermia (<36°C) - hypothermia is an ominous sign
- Tachycardia (>90 bpm)
- Tachypnea (>20 breaths/min)
- Warm, flushed skin (from vasodilation)
- Altered mental status (confusion, agitation)
- Decreased urine output
Late/Cold Phase (Hypodynamic State):
- Cool, mottled, clammy skin
- Hypotension (SBP <90 mmHg or MAP <65 mmHg)
- Worsening confusion/obtundation
- Oliguria/anuria
- Cyanosis
- Signs of end-organ failure
Quick SOFA (qSOFA) screening criteria (2 of 3 = high risk):
- Altered mental status
- Respiratory rate ≥22 breaths/min
- Systolic BP ≤100 mmHg
Note: The 2021 Surviving Sepsis Campaign guidelines recommend against using qSOFA alone as a screening tool, favoring NEWS or MEWS for clinical screening.
5. Diagnostic Tests for Sepsis
Hematology
- WBC count: Leukocytosis (>12,000) or leukopenia (<4,000) - present in SIRS but nonspecific. Febrile neutropenia (<500 cells/mm³) demands urgent action.
- Differential: Bandemia (≥5-10% bands) = release of immature cells, suggestive of active infection.
- Platelets: Thrombocytopenia in sepsis/DIC.
- Coagulation panel: Elevated PT/aPTT, decreased fibrinogen, elevated fibrin split products - all indicate DIC.
Blood Chemistry
- Lactate: Most critical prognostic marker. >2 mmol/L triggers septic shock classification. Lactate 0-2.5 mEq/L ~ 5% mortality; 2.5-4 mEq/L ~ 9%; >4 mEq/L ~ 28% mortality. Serial lactate clearance guides resuscitation.
- Creatinine/BUN: Renal dysfunction (AKI).
- Liver function tests: Hepatic dysfunction; elevated bilirubin may indicate biliary source.
- Blood glucose: Hyperglycemia is common in sepsis.
- Electrolytes: Bicarbonate low in metabolic acidosis; anion gap elevated in lactic acidosis.
- Lipase: Elevated in pancreatitis as the sepsis source.
- Troponin/BNP: Assess for myocardial depression.
Biomarkers
- Procalcitonin (PCT): >0.5 ng/mL suggests bacterial infection; <0.1 ng/mL makes it less likely. Most valuable for serial measurements and antibiotic stewardship. Does not exclude severe bacterial infection if low.
- C-reactive protein (CRP): Elevated in infection/inflammation; less specific than PCT.
Microbiology
- Blood cultures (minimum 2 sets from different sites): Obtain before antibiotics if possible. Only 30-40% of clinically septic patients have positive cultures.
- Urine culture/urinalysis: Particularly important in elderly patients.
- Sputum culture, wound cultures, CSF (if meningitis suspected).
- Gram stain results guide initial targeted therapy.
Organ Function Scoring
- SOFA score: Evaluates 6 organ systems (respiratory - PaO2/FiO2; coagulation - platelets; liver - bilirubin; cardiovascular - MAP/vasopressors; CNS - GCS; renal - creatinine). SOFA ≥2 above baseline = sepsis.
Imaging
- Chest X-ray: Pneumonia (focal infiltrate) or ARDS (bilateral infiltrates); free air under diaphragm for perforation.
- CT scan (abdomen/pelvis): Source identification - appendicitis, diverticulitis, abscess, pancreatitis.
- Ultrasound: Cholecystitis, pelvic source, cardiac function, volume assessment.
- MRI: Soft tissue infections (necrotizing fasciitis, epidural abscess).
- Echocardiography: Vegetations in endocarditis; myocardial function.
Rosen's Emergency Medicine, pp. 2756-2757; Washington Manual, pp. 295-297
6. Medical and Nursing Management
The "Hour-1 Bundle" (Surviving Sepsis Campaign 2021)
The Surviving Sepsis Campaign guidelines (most recently updated in 2021) recommend initiating the following within 1 hour of sepsis recognition:
| Action | Details |
|---|---|
| 1. Measure lactate | Remeasure if initial lactate >2 mmol/L |
| 2. Blood cultures | Before antibiotics if achievable without delay |
| 3. Broad-spectrum antibiotics | Administer immediately |
| 4. Fluid resuscitation | 30 mL/kg IV crystalloid for hypotension or lactate ≥4 mmol/L |
| 5. Vasopressors | If MAP <65 mmHg despite fluid resuscitation |
Fluid Resuscitation
- 30 mL/kg ideal body weight IV crystalloid within the first hour of presentation.
- Balanced crystalloids (lactated Ringer's) are preferred over normal saline - associated with lower rates of AKI and potentially improved mortality (SMART trial).
- Albumin offers no significant benefit over crystalloid in most septic patients.
- Reassess volume responsiveness continuously (passive leg raise, pulse pressure variation, point-of-care echo) to prevent volume overload.
Cardiovascular Support (Vasopressors)
| Agent | Mechanism | Role |
|---|---|---|
| Norepinephrine | α1 + β1 agonist; potent vasoconstriction | First-line vasopressor in septic shock |
| Vasopressin | G-protein receptor vasoconstriction | Second-line adjunct; may benefit less severe shock (NE 5-14 mcg/min) |
| Epinephrine | α + β agonist dose-dependent | Third-line; also used in anaphylactic shock |
| Phenylephrine | Selective α1 agonist | Limited evidence in septic shock |
| Angiotensin II | RAAS activation | Emerging evidence in refractory vasodilatory shock |
| Dobutamine | β1 agonist inotrope | For myocardial depression; risk of arrhythmia |
| Dopamine | Dose-dependent mixed | No longer preferred - more adverse events than NE |
Antimicrobial Therapy
- Administer immediately (ideally within 1 hour of recognition) - delays are directly associated with increased mortality.
- Use empirical broad-spectrum antibiotics covering the most likely pathogens based on suspected source and local resistance patterns.
- Narrow therapy when culture and sensitivity results are available (antibiotic stewardship).
- Duration guided by clinical response and serial procalcitonin measurements.
Source Control
- Identify and eliminate the infectious source as soon as feasible: drain abscesses, debride necrotic tissue, remove infected devices, treat necrotizing fasciitis surgically.
Respiratory Support
- Supplemental oxygen for all patients.
- Mechanical ventilation for ARDS: lung-protective ventilation strategy - tidal volume 6 mL/kg predicted body weight, plateau pressure <30 cmH2O, PEEP titration.
Glucose Control
- Target blood glucose 140-180 mg/dL - avoid both hyperglycemia and iatrogenic hypoglycemia.
Corticosteroids
- Hydrocortisone (200-300 mg/day in divided doses or infusion) may be used for refractory septic shock not responding adequately to fluids and vasopressors - evidence remains mixed but current guidelines suggest potential benefit.
Renal Replacement Therapy
- For AKI with metabolic acidosis, hyperkalemia, or oliguria unresponsive to treatment.
Lactate Clearance
- Targeting normalization of elevated lactate levels during resuscitation is associated with improved mortality. Serial measurements guide adequacy of resuscitation.
Nursing Management
Assessment:
- Continuous vital sign monitoring (BP, HR, RR, SpO2, temperature, urine output every hour)
- Neurological assessment (GCS, orientation)
- Assess skin color, temperature, capillary refill
- Monitor for new signs of organ dysfunction
Interventions:
- Establish IV access (2 large-bore peripheral IVs or central line)
- Draw blood cultures and other specimens promptly
- Administer IV fluids and vasopressors as ordered; titrate to MAP ≥65 mmHg
- Administer antibiotics on time - every hour of delay matters
- Maintain accurate fluid balance and strict hourly urine output (target ≥0.5 mL/kg/hr)
- Position patient appropriately (semi-Fowler for respiratory support)
- Elevate head of bed 30-45° if mechanically ventilated (VAP prevention)
- Oral care every 2-4 hours for intubated patients
- Nutritional support - early enteral nutrition when feasible
- Skin assessment and pressure injury prevention
- Venous thromboembolism (VTE) prophylaxis
- Emotional support to patient and family; clear communication
Monitoring Parameters:
- Vital signs, MAP, urine output (hourly)
- Serial lactate levels
- Blood glucose (goal 140-180 mg/dL)
- Daily weights, fluid balance
- Laboratory trends: CBC, CMP, coagulation, lactate, cultures
- Signs of developing complications
Rosen's Emergency Medicine; Washington Manual, pp. 295-298; Sabiston Textbook of Surgery
7. Complications of Sepsis and Methods of Prevention
Major Complications
| Complication | Mechanism |
|---|---|
| Acute Respiratory Distress Syndrome (ARDS) | Capillary leak in the lung from systemic inflammation causes bilateral non-cardiogenic pulmonary edema; impairs oxygenation |
| Acute Kidney Injury (AKI) | Renal hypoperfusion + microvascular inflammation + nephrotoxic medications |
| Disseminated Intravascular Coagulation (DIC) | Simultaneous microvascular thrombosis and consumption of clotting factors causing bleeding |
| Septic Cardiomyopathy | TNF-α, IL-1β, and NO directly depress myocardial contractility; may be reversible |
| Liver Failure | Hepatic hypoperfusion and inflammatory injury; elevated bilirubin, transaminases |
| Encephalopathy | Cerebral hypoperfusion, microthrombi, metabolic derangements causing altered consciousness |
| Multiple Organ Dysfunction Syndrome (MODS) | Culmination of the above; failure of ≥2 organ systems; highest mortality |
| Hypoglycemia | Can occur after initial hyperglycemia phase or from insulin treatment |
| Adrenal Insufficiency | Initial glucocorticoid surge may be followed by adrenal suppression |
| Secondary Infections | Immunosuppressive phase leaves patients vulnerable to opportunistic infections and ventilator-associated pneumonia (VAP) |
| Critical Illness Polyneuropathy/Myopathy | ICU-acquired weakness; functional disability post-sepsis |
| Post-Sepsis Syndrome | Long-term cognitive impairment, psychological sequelae (PTSD), physical weakness in survivors |
Prevention Strategies
Hospital-level Prevention:
- Hand hygiene - the single most effective measure to prevent healthcare-associated infections
- Central line-associated bloodstream infection (CLABSI) bundles: sterile technique during insertion, daily assessment of line necessity, prompt removal when no longer needed
- Catheter-associated urinary tract infection (CAUTI) prevention: minimize urinary catheter use, aseptic insertion, daily review
- Ventilator-associated pneumonia (VAP) bundle: head of bed elevation 30-45°, oral hygiene, daily sedation vacations, spontaneous breathing trials, peptic ulcer prophylaxis
- Surgical site infection prevention: perioperative antibiotics, normothermia, glucose control
Patient-Level Prevention:
- Appropriate vaccination (pneumococcal, influenza, COVID-19)
- Early recognition and treatment of infections before progression
- Optimizing chronic comorbidities (diabetes control, immunosuppression management)
- Early mobilization in ICU patients
Early Recognition (Sepsis Screening Tools):
- MEWS (Modified Early Warning Score) or NEWS (National Early Warning Score) - recommended by 2021 Surviving Sepsis guidelines as screening tools alongside SIRS
- Sepsis alerts and rapid response team activation
- Electronic health record-based sepsis alert algorithms
8. The Nurse's Role in Early Detection and Timely Intervention
Nurses are the primary point of contact for patients and are uniquely positioned to detect early signs of sepsis and initiate the chain of care. Research consistently demonstrates that earlier recognition and intervention improve survival.
Early Detection
- Continuous assessment: Systematic vital sign monitoring and trending. Recognize the subtle early signs - a rising respiratory rate or new confusion before frank hypotension develops.
- Pattern recognition: Know each patient's baseline - a heart rate of 95 may be tachycardia for one patient and normal for another.
- Apply validated screening tools: Use qSOFA, MEWS, or NEWS scores at every assessment to flag deteriorating patients.
- Trust clinical judgment: Nurses often recognize "the patient doesn't look right" before objective numbers confirm deterioration. Escalate early.
Timely Intervention
- Activate rapid response teams or sepsis protocols immediately when sepsis is suspected - do not wait for physician confirmation to begin preparing.
- Initiate the sepsis bundle: Draw blood cultures, establish IV access, collect labs (lactate, CBC, CMP, coagulation), and prepare for fluid administration.
- Advocate for prompt antibiotic administration - the 1-hour antibiotic goal requires nursing vigilance in ordering, pharmacy communication, and bedside delivery.
- Titrate vasopressors accurately: Frequent reassessment of MAP response; recognize early signs of over- or under-resuscitation.
- Escalation of care: Identify patients who need ICU transfer early; communicate using SBAR (Situation, Background, Assessment, Recommendation) for clear, efficient handoff.
Ongoing Monitoring and Nursing Surveillance
- Reassess every 30-60 minutes during active resuscitation
- Monitor for complications: falling urine output, worsening confusion, new skin mottling, rising lactate
- Ensure ordered tests are completed and results communicated to the team
- Prevent iatrogenic complications: pressure injuries, VAP, CLABSI, VTE
Patient and Family Education
- Explain the diagnosis, treatments, and expected course in understandable language
- Teach early warning signs of infection and sepsis to patients with chronic conditions for community-level prevention
- Support family members through an often frightening ICU experience
Advocacy and Quality Improvement
- Nurses drive sepsis quality improvement initiatives: compliance with bundles, simulation training, protocol development.
- Documentation accuracy supports data collection for sepsis outcomes reporting.
- Participation in multidisciplinary rounds ensures nursing observations are incorporated into the care plan.
Summary Table: Sepsis at a Glance
| Feature | Key Points |
|---|---|
| Definition | Life-threatening organ dysfunction (SOFA ≥2) from dysregulated host response to infection |
| Septic Shock | Sepsis + vasopressor-dependent hypotension + lactate >2 mmol/L; ~40% mortality |
| Key Pathogens | Gram-positive (most common in hospital), gram-negative, fungal |
| Core Pathophysiology | Cytokine storm → endothelial injury + vasodilation + DIC + metabolic failure → MODS |
| Diagnosis | Clinical + SOFA score + lactate + cultures + imaging |
| 1-Hour Bundle | Lactate, blood cultures, broad antibiotics, 30 mL/kg fluid, vasopressors for MAP <65 |
| First-line Vasopressor | Norepinephrine |
| Key Biomarker | Lactate (prognostic + guides resuscitation); procalcitonin (antibiotic stewardship) |
| Major Complications | ARDS, AKI, DIC, MODS, septic cardiomyopathy |
| Nursing Priority | Early recognition, sepsis bundle initiation within 1 hour, continuous reassessment |
Recent Evidence Note: A 2024 JAMA meta-analysis (PMID 38864162) found that prolonged infusions of β-lactam antibiotics are associated with improved outcomes in sepsis/septic shock compared with intermittent dosing. The 2026 Surviving Sepsis Campaign Pediatric Guidelines (PMID 41869844) have also been published for reference in pediatric cases. Methylene blue has been studied as an adjunct vasopressor in refractory septic shock (PMID 38904978), though its role remains investigational.
Sources: Rosen's Emergency Medicine; Robbins & Kumar Basic Pathology; Washington Manual of Medical Therapeutics; Sabiston Textbook of Surgery; Surviving Sepsis Campaign Guidelines 2021
This is a shared conversation. Sign in to Orris to start your own chat.