
IMG_3146.jpeg
Diagnose it
Reading File
Finding Sources
Searching PubMed
ring enhancing brain lesion MRI differential diagnosis
Finding Sources
Reading Article
PMID: 39475033
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have enough to provide a thorough, well-sourced analysis. The textbook GBM image is strikingly similar to the submitted scan.
MRI Brain Analysis - Post-Gadolinium T1-Weighted
Imaging Findings (What I See)
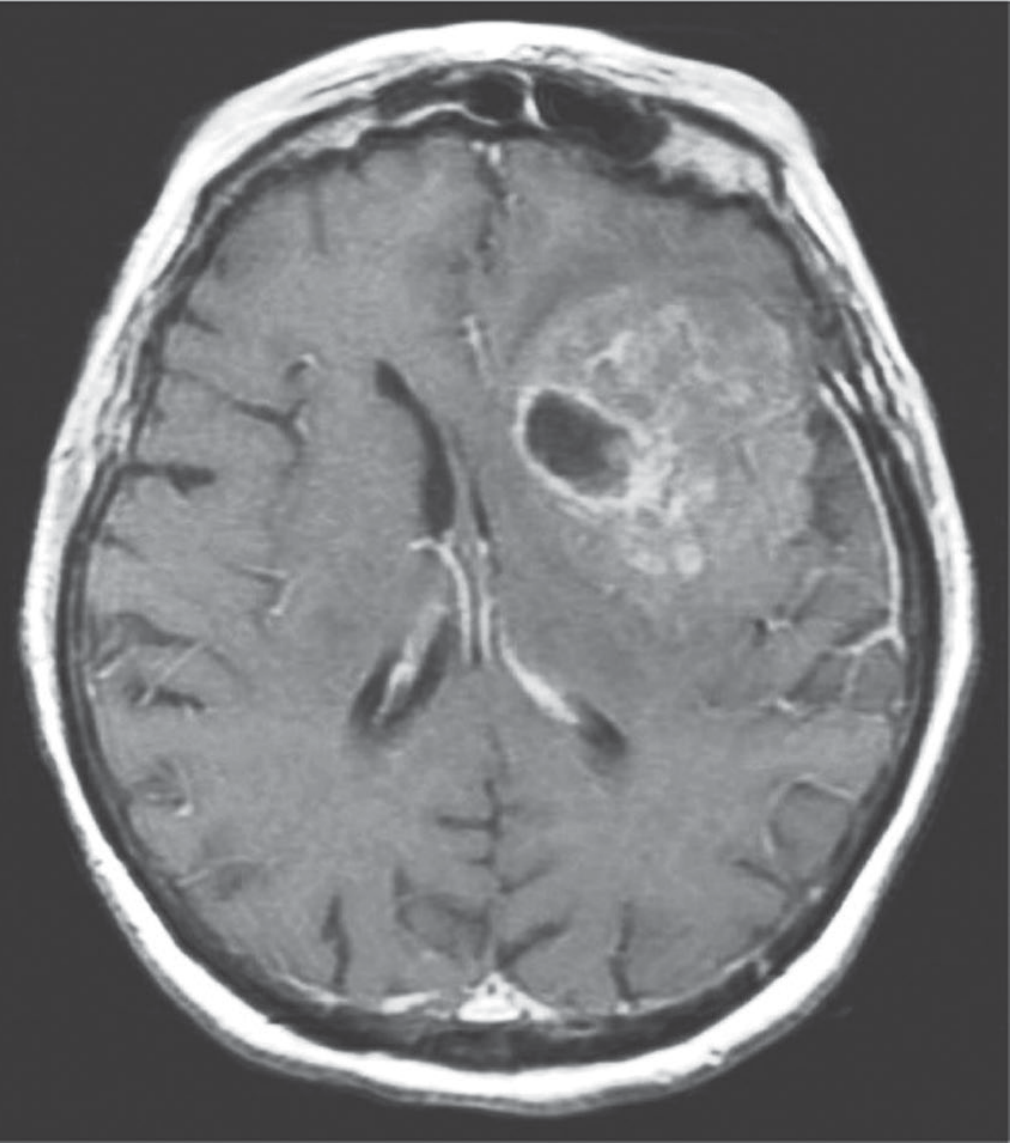
The axial post-contrast T1-weighted MRI shows:
- Large ring-enhancing lesion in the left parietal/temporal region with a thick, bright, irregular peripheral rim of gadolinium enhancement
- Central hypointense core - consistent with necrosis (not a simple cystic fluid)
- Irregular, nodular inner wall of the enhancing rim - the ring is not smooth or thin-walled
- Mass effect with midline shift toward the right (the falx cerebri appears deviated)
- The enhancing ring is thick and heterogeneous, not thin and regular
- No obvious satellite lesions visible on this single slice
Most Likely Diagnosis
Glioblastoma (GBM), IDH-Wildtype (WHO Grade 4)
This is the leading diagnosis. As described in Adams and Victor's Principles of Neurology (12th ed.):
"The imaging appearance is usually that of an inhomogeneous mass, often with a center that is hypointense and nonenhancing. An irregular rim of contrast enhancement surrounds the core lesion, and is surrounded by nonenhancing edematous brain tissue, consisting of a combination of infiltrating tumor cells and vasogenic edema."
The textbook reference image (shown below for comparison) is nearly identical to this scan:
Key features favoring GBM over other ring-enhancing lesions:
| Feature | This Scan | GBM | Brain Abscess | Metastasis |
|---|---|---|---|---|
| Ring thickness | Thick, irregular | Thick + irregular | Thin, uniform | Variable |
| Inner wall | Nodular/irregular | Nodular | Smooth | Smooth-ish |
| Core | Dark, heterogeneous | Necrotic | Pus (very dark, uniform) | Necrotic |
| Mass effect | Present | Yes | Moderate | Yes |
| Location | Left hemisphere, deep | Frontal/temporal/parietal | Any | Gray-white junction |
Differential Diagnoses (in order of likelihood)
-
Glioblastoma (GBM) - Most likely. Thick irregular enhancing ring, central necrosis, solitary, in cerebral hemisphere. Peak incidence 5th-6th decade, male predominance. - Bradley and Daroff's Neurology in Clinical Practice
-
Brain metastasis - Second consideration. Metastases and gliomas both appear as ring-enhancing lesions on contrast imaging (Bailey and Love's Surgery, 28th ed.). However, metastases typically sit at the gray-white junction, are often multiple, and tend to have thinner, smoother walls with more surrounding edema relative to lesion size.
-
Brain abscess - Less likely here. Abscesses appear as "well-demarcated, ring-enhancing, thin-walled lesions" with very smooth inner walls (Schwartz's Principles of Surgery, 11th ed.). The irregular, thick, nodular rim argues against abscess. Abscess core is also more uniformly dark (pus) with restricted diffusion on DWI.
-
Primary CNS lymphoma - Typically shows homogeneous solid enhancement (not ring) in immunocompetent patients; ring-enhancing pattern more common in HIV/immunocompromised.
-
Tumefactive MS - Incomplete (open) ring enhancement differentiates MS from tumors/abscess (Grainger & Allison's Diagnostic Radiology). The closed, thick ring here argues against this.
Additional Imaging Recommended
To confirm and characterize further:
- DWI/ADC map - Abscess shows restricted diffusion in the core (low ADC); GBM typically does not
- MR Spectroscopy - GBM shows elevated Cho:NAA ratio, elevated lipid/lactate peak
- MR Perfusion (DSC) - GBM has high rCBV; abscess and demyelination do not
- FDG-PET or MR-Amino acid PET - High uptake favors high-grade glioma
Clinical Implication
If GBM is confirmed on biopsy:
- Standard of care: Stupp protocol - maximal safe surgical resection + concurrent temozolomide + radiotherapy, followed by adjuvant temozolomide
- Test for MGMT promoter methylation (favorable prognostic marker) and IDH status (IDH-wildtype = true GBM, worse prognosis)
- Median survival remains approximately 15 months even with treatment
Important caveat: This is a radiological interpretation for educational/clinical decision-support purposes. Definitive diagnosis requires tissue biopsy and neuropathology. Clinical context (age, symptoms, history of systemic cancer) should guide the differential prioritization.
Sources: Adams and Victor's Principles of Neurology 12th Ed., Bradley and Daroff's Neurology in Clinical Practice, Schwartz's Principles of Surgery 11th Ed., Bailey and Love's Surgery 28th Ed., Grainger & Allison's Diagnostic Radiology; Peker et al., Br J Hosp Med, 2024 [PMID: 39475033]
This is a shared conversation. Sign in to Orris to start your own chat.