Genitourinary urinary incontinence
Reading File
Finding Sources
Finding Sources
Searching PubMed
"urinary incontinence"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material to write a detailed answer. Let me compile it.
Urinary Incontinence
Definition
Urinary incontinence (UI) is the involuntary leakage of urine sufficient to be a health or social problem. It is one of the most prevalent and underreported conditions in clinical practice. - Goldman-Cecil Medicine, p. 1324
Epidemiology
- More than twice as common in women as men; prevalence increases with age.
- At least some degree of UI is reported by 11% of women aged 22-27 years.
- Afflicts 15-30% of older adults living at home, one third of those in acute care settings, and >50% of nursing home residents.
- Estimated US cost exceeded $83 billion in 2020, with out-of-pocket patient costs >$500.
- Over 20 million women in the US are affected; projected to increase by >50% in the coming decade.
- Average prevalence by subtype: Stress UI 13%, Urgency UI 5%, Mixed UI 11%. - Berek & Novak's Gynecology, p. 1524
Despite its prevalence and adverse consequences, UI remains largely neglected by both patients and physicians. - Goldman-Cecil Medicine, p. 1324
Prevalence by Subtype and Age
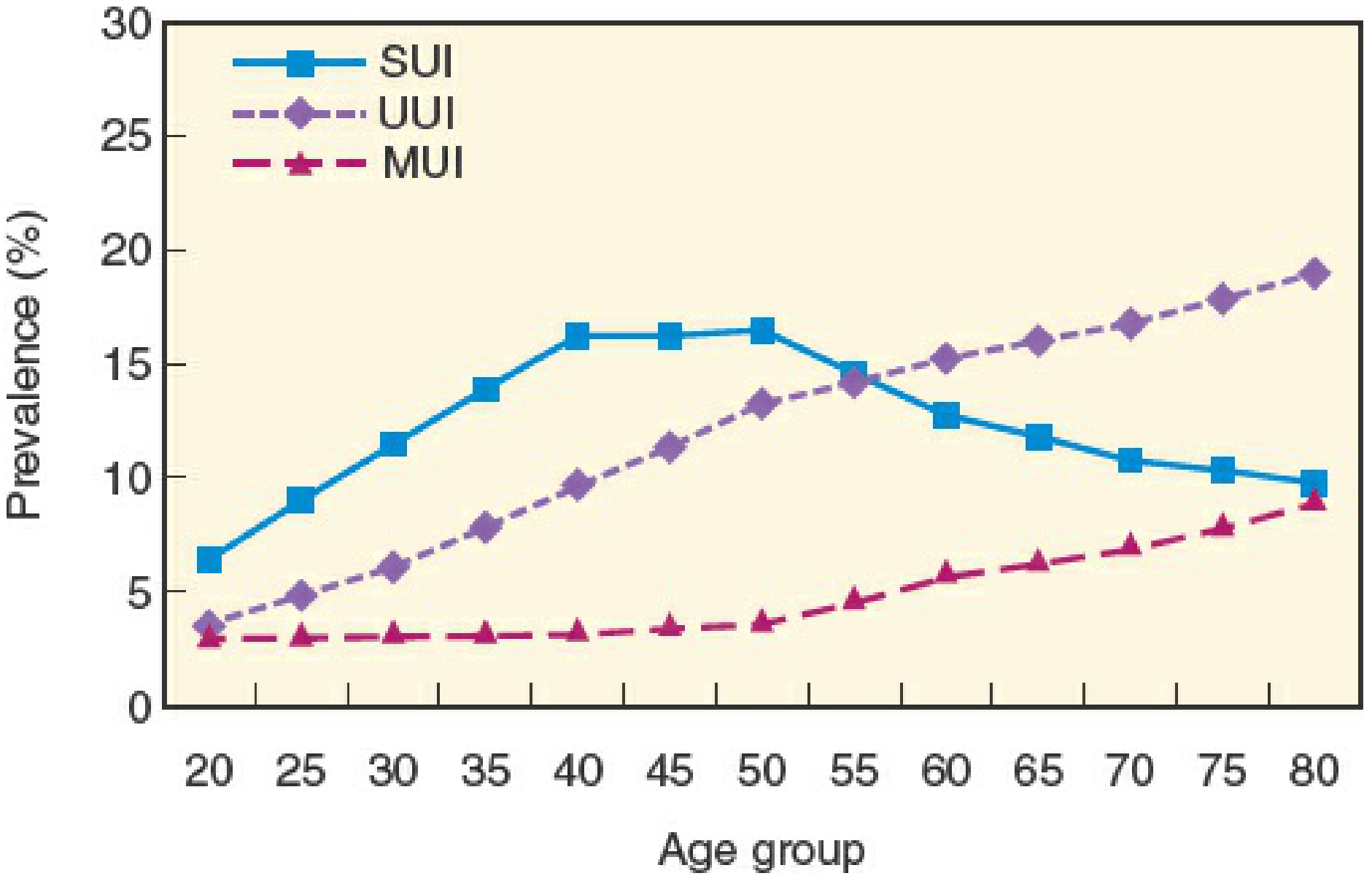
SUI peaks at age 50 then declines; UUI and MUI increase continuously into late adulthood. Mixed UI becomes the dominant subtype in late adulthood. - Berek & Novak's Gynecology, p. 1524
Classification and Types
| Type | Definition | Key Features |
|---|---|---|
| Stress UI (SUI) | Involuntary leakage on effort, exertion, sneezing, or coughing | Coincides instantaneously with onset AND cessation of increased abdominal pressure; rare nocturnal leakage |
| Urgency UI (UUI) | Involuntary leakage associated with a sudden, strong urge to void | May follow sounds of running water, temperature change, arriving home |
| Mixed UI (MUI) | Leakage associated with both urgency and effort/exertion | Determine most bothersome component to guide treatment |
| Overflow incontinence | Leakage from an overfull, poorly emptying bladder | Caused by outlet obstruction or detrusor underactivity |
| Continuous UI | Continuous involuntary urine loss | Suggests fistula (vesicovaginal, urethrovaginal) |
| Postural UI | Leakage with change in body position | e.g., rising from seated or lying position |
| Insensible UI | Patient unaware of how leakage occurred | Often neurogenic |
| Nocturnal enuresis | Involuntary loss during sleep | |
| Coital UI | Loss during intercourse | May occur with penetration or at orgasm |
- Berek & Novak's Gynecology, p. 1523
Women frequently transition between subtypes: in a large study, over 2 years, 34-38% of those with UUI remitted, while others transitioned to SUI or MUI. - Berek & Novak's Gynecology, p. 1522
Pathophysiology
Normal Continence Requirements
Continence depends not only on lower urinary tract integrity but also on:
- Adequate mentation, mobility, motivation, and manual dexterity
- These "4 Ms" are rarely deficient in younger patients but commonly impaired in older patients
Age-Related Changes (Predisposing, Not Causative)
- Bladder capacity is preserved, but sensation and contractility decrease
- Detrusor smooth muscle develops a "dense band pattern" with depleted caveolae - impairs contractility
- Incomplete disjunction pattern (protrusion junctions) - underlies high prevalence of involuntary detrusor contractions (overactivity) in older adults
- Urethral length and sphincter strength decrease in women
- Prostate enlarges in men, causing obstruction in ~50%
- Postvoid residual increases (but normally <100 mL)
- Older adults excrete most fluid intake at night (nocturia)
None of these changes alone causes incontinence, but all predispose to it. - Goldman-Cecil Medicine, p. 1324-1325
Mechanisms by Type
Detrusor Overactivity (Urge UI):
- Most common cause in the elderly (~2/3 of cases)
- Histologically: widening of intercellular space, emergence of novel protrusion junctions and ultraclose abutments creating electrical coupling -> involuntary contractions
- Usually idiopathic, but may associate with cerebral disease, upper motor neuron lesions, urethral obstruction, bladder calculus, bladder carcinoma
- Detrusor Hyperactivity with Impaired Contractility (DHIC) - a subset unique to the elderly: may mimic stress incontinence, outlet obstruction (in men), or overflow; bladder relaxants may precipitate retention
Stress Incontinence:
-
Reflects insufficient urethral support plus some degree of sphincter weakness
-
Most common cause in middle-aged women; second most common in older women
-
In men with radical prostatectomy: resembles "intermittent drip of a leaky faucet"
-
Goldman-Cecil Medicine, p. 1325-1329
Causes of Transient Incontinence - "DIAPERS" Mnemonic
| Letter | Cause | Mechanism |
|---|---|---|
| D | Delirium | Incontinence is secondary; resolves when delirium treated |
| I | Infection (symptomatic UTI) | Acute UTI worsens UI; asymptomatic bacteriuria does NOT |
| A | Atrophic urethritis/vaginitis | Vaginal erosions, telangiectasia, petechiae; contributes to UI |
| P | Pharmaceuticals | See drug table below |
| E | Excess urine output | Large intake, diuretics, caffeine, alcohol; hyperglycemia, hypercalcemia; nocturnal from OSA or peripheral edema mobilization |
| R | Restricted mobility | Arthritis, pain, foot problems, postprandial hypotension, fear of falling |
| S | Stool impaction | Causes both fecal and urinary incontinence; resolves with disimpaction |
Transient causes account for up to 1/3 of community-dwelling elderly and up to half of hospitalized patients. - Goldman-Cecil Medicine, p. 1328
Medications That Cause or Worsen Incontinence
| Drug Class | Effect |
|---|---|
| Sedative-hypnotics (benzodiazepines, alcohol) | Sedation, delirium, decreased mobility; alcohol also diuresis |
| Anticholinergics (antihistamines, TCAs, antipsychotics, antispasmodics, anti-Parkinson agents) | Urinary retention, overflow, delirium, constipation |
| Opiates | Retention, impaction, sedation, delirium |
| Alpha-adrenergic blockers (prazosin, terazosin) | Relax sphincter -> stress UI in women |
| Alpha-adrenergic agonists (OTC cold remedies) | Increase outlet resistance -> retention in men |
| Calcium channel blockers | Reduce detrusor contractility -> voiding problems; peripheral edema -> nocturia |
| ACE inhibitors | Drug-induced cough -> stress UI in women |
| Loop diuretics | Polyuria, frequency, urgency |
| Thiazolidinediones, NSAIDs, gabapentin/pregabalin | Nocturnal diuresis due to fluid retention |
| Cholinesterase inhibitors | Urinary incontinence |
| Vincristine | Urinary retention (neuropathy) |
- Goldman-Cecil Medicine, p. 1328; Berek & Novak's Gynecology, p. 1534
Diagnosis and Evaluation
History
- Type of UI (urge, stress, overflow, or mixed)
- Frequency, severity, and duration
- Pattern (diurnal, nocturnal, postural, positional)
- Triggers: coughing, sneezing, urgency, sound of running water
- Prior pelvic surgeries, childbirth history, prolapse symptoms
- Neurological conditions, medications
- Fluid intake (volume, caffeine, alcohol)
Physical Examination
- Cough stress test: patient coughs with full bladder while supine/standing; instantaneous leakage confirms SUI
- Pelvic exam: atrophic vaginitis, prolapse, pelvic floor tone, urethral hypermobility
- Neurological exam: sacral reflexes, perineal sensation
Investigations
First-line (all patients):
| Test | Purpose |
|---|---|
| Urinalysis/culture | Rule out UTI as cause |
| Postvoid residual (PVR) | Catheter or ultrasound; PVR <50 mL = normal; >150 mL = abnormal; guides management |
| Bladder diary (2-3 days) | Fluid intake, voiding frequency, voided volumes, incontinence episodes with circumstances; 2-3 days equally reliable as 7 days |
Pad test: Pads weighed over 24-48 hours; more objective measure of leakage severity. Longer duration = more reproducible (48-hour correlation coefficient 0.90). Does NOT distinguish stress from urge or capture bother. - Campbell-Walsh Wein Urology, p. 143
Urodynamics (second-line, selected patients):
-
Not required for straightforward SUI prior to surgery
-
Indicated when: diagnosis unclear after history/exam/simple testing; complex/mixed symptoms failing conservative therapy; planned prolapse surgery to detect occult SUI; prior anti-incontinence surgery failed; elevated PVR; neurologic conditions (e.g., MS)
-
Components: uroflowmetry, filling cystometry, pressure-flow studies, urethral pressure profilometry
-
Berek & Novak's Gynecology, p. 1533-1540; Goldman-Cecil Medicine, p. 1329
Treatment
Treatment requires a multifactorial approach: address precipitants, underlying medical conditions, functional impairments, fluid intake, AND the urinary tract abnormality. Treatment of precipitants alone may restore continence.
1. Lifestyle Interventions (all types)
- Fluid and caffeine intake reduction/adjustment
- Weight loss (overweight women with SUI)
- Smoking cessation (reduces chronic cough -> SUI)
- Scheduled voiding (timed toileting)
- Bedside urinal for nocturia
- Phone-based apps (show promise for urge/mixed UI)
2. Behavioral Therapy
| Intervention | Type of UI | Evidence |
|---|---|---|
| Pelvic floor muscle training (PFMT/Kegel exercises) | SUI, UUI, MUI | Effective; less effective than surgery for SUI alone; combining with surgery offers no added benefit |
| Bladder retraining (progressively increasing voiding intervals + urgency suppression techniques) | UUI | As effective as pharmacotherapy for UUI |
| Prompted voiding | Institutionalized patients with cognitive impairment who can state their name and are partly mobile | Effective for daytime incontinence |
| Pessaries | SUI | Can be effective as conservative management |
| Acupuncture | SUI | Some evidence of effectiveness |
| Group vs. individual education | Both | Equally effective alternative |
A 2024 Cochrane systematic review confirmed the effectiveness of PFMT across multiple approaches for UI in women. [PMID: 39704322]
For UUI: behavioral therapy + pharmacotherapy combined is more effective than either alone, since neither abolishes involuntary contractions. - Goldman-Cecil Medicine, p. 1329
3. Pharmacotherapy
For Urgency UI (detrusor overactivity):
| Drug Class | Examples | Notes |
|---|---|---|
| Antimuscarinics (bladder relaxants) | Oxybutynin, tolterodine, solifenacin, darifenacin, trospium | Modestly and equally effective; ADRs: dry mouth, constipation, visual blurring; use with caution in elderly (cognitive effects); DHIC patients may develop retention |
| Beta-3 adrenergic agonist | Mirabegron | Alternative/adjunct to antimuscarinics; fewer anticholinergic effects |
For Stress UI:
- No currently approved pharmacotherapy has proved effective
- Duloxetine (SNRI) increases urethral sphincter tone - used in some countries (not FDA-approved for SUI in the US)
For Overflow:
-
Treat the underlying cause (obstruction: alpha-blockers in men; urinary retention: catheterization, cholinergic agents rarely used)
-
Goldman-Cecil Medicine, p. 1329-1330
4. Surgical Treatment
Stress UI in women:
- Mid-urethral sling (MUS) - retropubic (TVT) or transobturator (TOT) - current gold standard for SUI
- Burch colposuspension - open or laparoscopic retropubic suspension
- Pubovaginal sling (autologous fascia)
- Bulking agents (periurethral injection) - less durable, for patients unfit for surgery or sphincteric deficiency
- Artificial urinary sphincter - mainly for intrinsic sphincter deficiency
Urgency UI:
- Sacral neuromodulation (SNM) - for refractory OAB
- Intradetrusor botulinum toxin A (onabotulinumtoxinA) - effective for refractory UUI; risk of urinary retention
- Posterior tibial nerve stimulation (PTNS) - percutaneous or transcutaneous
Overflow/Obstruction:
- TURP or other procedures for BPH
- Clean intermittent self-catheterization (CISC) for neurogenic or refractory retention
Special Populations
Elderly
- Broader multifactorial assessment required
- Functional factors (mobility, dexterity, cognition) must be addressed alongside bladder pathology
- DHIC common - bladder relaxants may cause retention at standard doses
- Anticholinergics pose higher cognitive risk in frail elderly
- Catheterization is rarely appropriate for chronic UI due to high UTI risk
Men
- UUI from detrusor overactivity and SUI from radical prostatectomy are most common
- Post-prostatectomy UI: pelvic floor exercises first line; artificial urinary sphincter for persistent, severe cases
- DHIC may mimic prostatic obstruction
Pregnancy/Postpartum
- SUI common due to mechanical factors and pelvic floor changes
- PFMT is the primary intervention
Impact and Consequences
UI is associated with:
- Perineal rashes, pressure ulcers, UTIs
- Falls and fractures
- Embarrassment, stigmatization, isolation
- Depression, anxiety, sexual dysfunction
- Risk for institutionalization
Many seriously ill elderly patients rate UI as an outcome worse than death. - Goldman-Cecil Medicine, p. 1324
Key Sources
- Goldman-Cecil Medicine International Edition, Ch. 115 (Resnick & Dubeau)
- Berek & Novak's Gynecology, Ch. 29
- Campbell-Walsh Wein Urology, 3-Volume Set
- Hay-Smith et al. [Cochrane 2024 - PMID: 39704322] - PFMT comparisons for UI in women
- Moris et al. [Eur Urol 2025 - PMID: 39848866] - Prevalence, diagnosis, and management of SUI in women (current systematic review confirming mid-urethral slings as standard of care)
This is a shared conversation. Sign in to Orris to start your own chat.