Dose of Adrenaline and dopamine in bradycardia
Reading File
Finding Sources
Finding Sources
Searching PubMed
bradycardia management epinephrine dopamine
Reading File
Reading File
Reading File
I now have comprehensive data from multiple authoritative emergency medicine and anesthesia textbooks. Here is the complete answer:
Adrenaline (Epinephrine) and Dopamine in Bradycardia
Both drugs are second-line agents used when atropine fails or is contraindicated. They are given as IV infusions, not bolus doses (except in cardiac arrest).
Step-by-step Management Context
- First line: Atropine - 1 mg IV every 3-5 min, max total dose 3 mg
- If atropine fails or is inappropriate (e.g., heart transplant, Mobitz II / third-degree AV block with wide QRS): start epinephrine or dopamine infusion, and prepare for transcutaneous pacing (TCP)
- Atropine is unlikely to work in infranodal blocks (Mobitz II, complete heart block) - go straight to TCP + chronotropes
Adrenaline (Epinephrine) - IV Infusion for Bradycardia
| Parameter | Detail |
|---|---|
| Indication | Symptomatic bradycardia unresponsive to atropine; cardiogenic shock with bradycardia |
| Preparation | 1 mg in 500 mL normal saline (concentration: 2 mcg/mL) |
| Starting dose | 2 mcg/min IV infusion |
| Titration | Escalate as needed at 3-5 minute intervals |
| Range | 2-10 mcg/min |
| Mechanism | Alpha + Beta adrenergic effects: increases HR, BP, CO |
"For IV infusion in patients with cardiogenic shock or symptomatic bradycardia, the dose is 1 milligram in 500 mL of normal saline beginning at 2 to 10 micrograms/min and escalating as needed at 3- to 5-minute intervals." - Tintinalli's Emergency Medicine
Pediatric dose (cardiac arrest / symptomatic bradycardia): 0.01 mg/kg IV/IO of 1:10,000 solution (0.1 mL/kg), max single dose 1 mg, repeat every 3-5 min PRN.
Dopamine - IV Infusion for Bradycardia
| Parameter | Detail |
|---|---|
| Indication | Symptomatic bradycardia, especially if hypotension co-exists |
| Starting dose | 2-5 mcg/kg/min IV |
| Usual range | 2-20 mcg/kg/min, titrated by 5-10 mcg/kg/min increments |
| Maximum dose | Up to 50 mcg/kg/min (some sources 20-50 mcg/kg/min) |
| Mechanism (dose-dependent): | |
| - Low dose (2-5 mcg/kg/min) | Dopaminergic + mild beta-1: increases HR and inotropy |
| - Medium dose (5-10 mcg/kg/min) | Beta-1 dominant: increases HR, BP, CO |
| - High dose (>10-15 mcg/kg/min) | Alpha dominant: vasoconstriction, decreases renal perfusion |
"Dopamine is a catecholamine with both alpha- and beta-adrenergic actions and can be titrated to target heart rate or vasoconstriction more selectively. At lower doses, dopamine has a more selective effect on inotropy and heart rate; at higher doses (>10 mcg/kg/min), it also has vasoconstrictive effects." - Miller's Anesthesia
Quick Comparison
| Feature | Epinephrine | Dopamine |
|---|---|---|
| Dose form in bradycardia | 2-10 mcg/min infusion | 2-20 mcg/kg/min infusion |
| Weight-based dosing? | No (fixed mcg/min) | Yes (mcg/kg/min) |
| Preferred if hypotension present | Yes | Yes |
| Preferred if low risk of arrhythmia | Either | Dopamine preferred |
| Arrhythmia risk | Higher | Lower at low doses |
Key Points
- Both are bridge therapies until transcutaneous or transvenous pacing is established
- Neither works well in complete heart block with wide QRS - pacing is the definitive treatment
- In post-cardiac transplant patients, atropine is ineffective (denervated heart); use isoproterenol 2-10 mcg/min or pacing
- Do not add epinephrine to alkaline infusion solutions
Sources: Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Miller's Anesthesia, 10e; Harriet Lane Handbook, 23e
bradycardia algorithm according to ACLS
Finding Sources
Finding Sources
Searching the Web
ACLS bradycardia algorithm 2020 AHA steps
Loading Image
Reading File
Reading File
Here is the complete ACLS Bradycardia Algorithm:
ACLS Adult Bradycardia Algorithm (2020 AHA Guidelines)
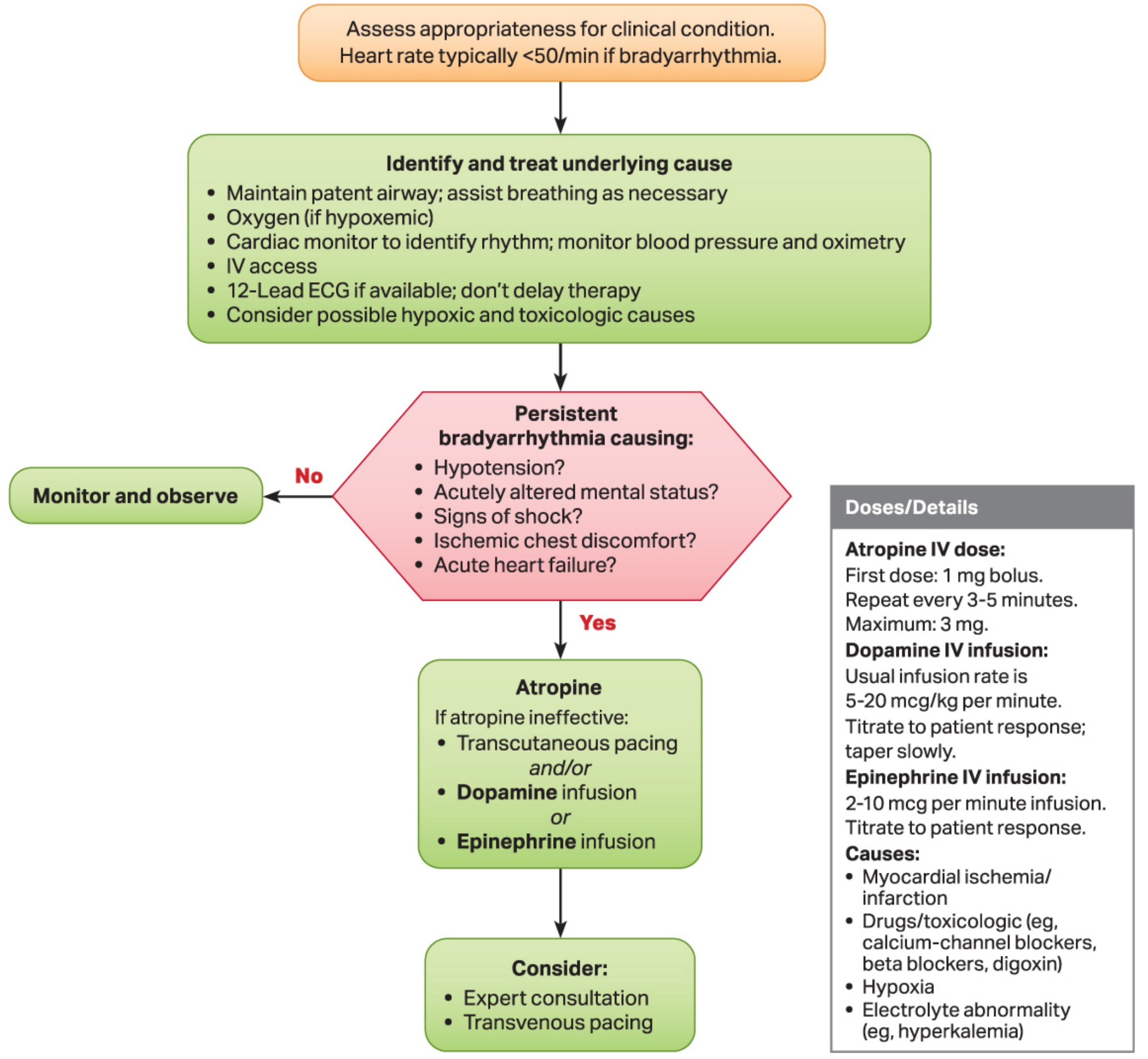
(Reprinted with permission - ACLS Advanced Cardiovascular Life Support Provider Manual. © 2020 American Heart Association)
Step-by-Step Breakdown
Step 1 - Initial Assessment
- Confirm heart rate < 50/min with bradyarrhythmia
- Check for a pulse - if no pulse, switch to Cardiac Arrest Algorithm
Step 2 - Identify and Treat Underlying Cause (Simultaneously)
- Maintain patent airway; assist breathing if needed
- Oxygen (if hypoxemic)
- Cardiac monitor to identify rhythm; monitor BP and SpO2
- Establish IV access
- 12-lead ECG if available - do NOT delay therapy
- Consider possible hypoxic and toxicologic causes
Common underlying causes:
- Myocardial ischemia / infarction
- Drugs (beta-blockers, calcium channel blockers, digoxin)
- Hypoxia
- Electrolyte abnormalities (e.g., hyperkalemia)
Step 3 - Key Decision: Is the Bradycardia Causing Symptoms?
Ask: Is there persistent bradyarrhythmia causing any of the following?
| Sign of Instability |
|---|
| Hypotension |
| Acutely altered mental status |
| Signs of shock |
| Ischemic chest discomfort |
| Acute heart failure |
- NO → Monitor and observe
- YES → Proceed to treatment
Step 4 - Symptomatic/Unstable: Give Atropine
Atropine - First-line drug
| Dose | |
|---|---|
| First dose | 1 mg IV bolus |
| Repeat | Every 3-5 minutes |
| Maximum total dose | 3 mg |
Key 2020 update: Dose increased from 0.5 mg to 1 mg per dose to improve efficacy and avoid paradoxical bradycardia (doses < 0.5 mg can cause paradoxical bradycardia).
Note: Atropine is NOT expected to work in:
- Mobitz type II second-degree AV block
- Third-degree (complete) AV block with wide QRS
- Post-cardiac transplant patients (denervated heart)
Step 5 - If Atropine is Ineffective: Three Options (can use simultaneously)
| Option | Drug / Intervention | Dose |
|---|---|---|
| A | Transcutaneous Pacing (TCP) | Rate typically 60-80/min; use sedation |
| B | Dopamine IV infusion | 5-20 mcg/kg/min - titrate; taper slowly |
| C | Epinephrine IV infusion | 2-10 mcg/min - titrate to response |
TCP and drug infusion can be used together (and/or).
Step 6 - Consider
- Expert consultation (cardiology)
- Transvenous pacing (definitive treatment for high-degree AV block)
Important Clinical Notes
| Scenario | Action |
|---|---|
| Mobitz II / complete heart block | Skip atropine - go directly to TCP + pacing preparation |
| Post-cardiac transplant | Atropine ineffective - use isoproterenol 2-10 mcg/min or pace |
| Suspected drug toxicity (BB, CCB) | Treat the cause (glucagon, calcium, lipid emulsion) |
| Reversible cause found | Treat the cause first |
Quick Dose Summary Box (from the Algorithm)
| Drug | Dose |
|---|---|
| Atropine | 1 mg IV bolus, repeat q3-5 min, max 3 mg |
| Dopamine | 5-20 mcg/kg/min IV infusion |
| Epinephrine | 2-10 mcg/min IV infusion |
Sources: Barash's Clinical Anesthesia 9e; Miller's Anesthesia 10e (Fig. 82.6 - 2020 AHA Adult Bradycardia Algorithm); AHA ACLS Guidelines 2020
This is a shared conversation. Sign in to Orris to start your own chat.