Give me research related data of ejaculation time i mean after intercourse how much time a man take to ejaculate, also give other related information
Reading File
Searching PubMed
intravaginal ejaculation latency time IELT normal distribution
Searching the Web
average ejaculation time during intercourse research IELT stopwatch study
Reading Article
PMID: 16422843
Finding Sources
Searching PubMed
ejaculation time factors age circumcision condom effect
Reading File
Searching PubMed
premature ejaculation prevalence definition DSM
Here is a thorough, research-backed overview of ejaculation time during intercourse.
Ejaculation Time During Intercourse: Research Data
What Is IELT?
The standard scientific measure is the Intravaginal Ejaculation Latency Time (IELT) - defined as the time from the moment of vaginal penetration to the moment of intravaginal ejaculation. It was formally introduced in 1994 by Waldinger et al. and is now the gold standard measure in clinical trials. The most accurate way to measure it is using a stopwatch operated by the female partner.
Key Research Findings
The Landmark Stopwatch Study (Waldinger et al., 2005)
The largest and most cited real-world study on IELT involved 491 men from 5 countries (Netherlands, UK, Spain, Turkey, USA) who used stopwatches over 4 weeks:
| Metric | Value |
|---|---|
| Median IELT (all countries) | 5.4 minutes |
| Range | 0.55 - 44.1 minutes |
| Distribution | Positively skewed (right-skewed) |
Source: Waldinger et al., Journal of Sexual Medicine (2005) - PMID: 16422843
Second Major Stopwatch Study (2009)
A follow-up study using a blinded timer device on 474 men from the same 5 countries found a nearly identical result - median IELT of 6.0 minutes (range: 0.1-52.7 minutes).
Distribution - The Full Picture
The IELT is not normally distributed - it follows a log-normal, positively skewed distribution, meaning:
- A large number of men ejaculate relatively quickly
- A smaller number have very long IELTs
- The tail extends to 30-50+ minutes
Rough percentile breakdown from population data:
- ~14% of men ejaculate in under 3 minutes 20 seconds
- ~50% of men ejaculate in under 5-6 minutes (median)
- ~26% of men take over 10 minutes
Effect of Age on IELT
Age has a statistically significant effect (P < 0.0001):
| Age Group | Median IELT |
|---|---|
| 18-30 years | 6.5 minutes |
| 31-50 years | 5.4 minutes |
| Over 51 years | 4.3 minutes |
Ejaculation time decreases with age, likely due to changes in neurological sensitivity and hormonal factors.
Country/Cultural Differences
From the 2005 multinational study:
| Country | Median IELT |
|---|---|
| Turkey | 3.7 minutes (significantly lower) |
| Netherlands, UK, Spain, USA | ~5.4-6.5 minutes |
The reason for Turkey's lower median is not fully established; researchers noted it may be related to circumcision patterns, cultural factors, or partner dynamics.
Effect of Condom Use and Circumcision
- Condom use: No significant effect on IELT
- Circumcision: Circumcised men had a median IELT of 6.7 min vs. 6.0 min in uncircumcised men - a difference that was not statistically significant
What Is "Premature Ejaculation" (PE)?
There are several official definitions:
| Organization | Definition |
|---|---|
| DSM-5 | Ejaculation occurring within ~1 minute of penetration (lifelong PE), or clinically bothersome reduction in latency |
| ICD-10 (WHO) | Ejaculation before or within 15 seconds of beginning intercourse |
| ISSM (International Society for Sexual Medicine) | Always/nearly always ejaculates within 1 min (lifelong PE) or within 3 min (acquired PE), with inability to delay and negative personal consequences |
From [Campbell-Walsh Wein Urology], the DSM criteria historically lacked objective time cutoffs, which caused significant problems in interpreting clinical research until stopwatch studies established evidence-based benchmarks.
In men with lifelong PE (who seek treatment):
- ~90% ejaculate within 1 minute of penetration
- ~10% ejaculate between 1-2 minutes
- Average IELT in PE patients: ~1.8 minutes
- Average IELT in non-PE men: ~7.3 minutes (from a 1,587-man study, ScienceDaily/J Sex Med 2005)
What Do Sex Therapists Consider "Normal"?
A 2008 survey of Canadian and American sex therapists provided these benchmarks:
| Duration | Therapist Rating |
|---|---|
| 1-2 minutes | Too short |
| 3-7 minutes | Adequate |
| 7-13 minutes | Desirable |
| 13-30 minutes | Too long |
Factors That Influence IELT
Factors that shorten ejaculation time:
- Older age
- Anxiety, performance pressure
- Lifelong neurobiological predisposition (serotonin pathway variants)
- Thyroid hypersensitivity (hyperthyroidism linked to PE)
Factors that lengthen ejaculation time:
- Alcohol (CNS depressant)
- Opioids (heroin, morphine, oxycodone)
- SSRIs (e.g., dapoxetine) - used specifically to treat PE by blocking serotonin reuptake and delaying the "point of ejaculatory inevitability"
- Topical anesthetic creams
- PDE5 inhibitors (sildenafil, tadalafil) - some evidence for combined SSRI + PDE5i being more effective than SSRI alone
Delayed Ejaculation (DE)
The opposite problem - where ejaculation takes an abnormally long time or cannot occur at all:
- Spectrum ranges from prolonged latency to complete anejaculation
- Causes include: antidepressants, opioids, neurological injury, psychological factors
- No universally agreed time cutoff for DE (some use >30 minutes as a threshold)
Key Takeaway
The scientifically measured average time to ejaculation during intercourse is approximately 5-7 minutes, but there is enormous natural variability. The range of 0.5 minutes to 44+ minutes is documented in healthy, unselected men. IELT follows a log-normal distribution, so the median is a better descriptor than the mean. Anything between roughly 3 and 13 minutes can be considered within the broad normal range by clinical and therapist consensus.
Search for latest clinical guidelines on treating premature ejaculation
Searching PubMed
premature ejaculation treatment guidelines
Searching the Web
premature ejaculation clinical guidelines 2024 2025 AUA EAU treatment recommendations
Finding Sources
Reading Article
PMID: 40340108
Reading Web Page
https://www.frontiersin.org/journals/endocrinology/articles/…
Reading File
Reading File
Reading Article
PMID: 41031773
Loading Image
Finding Sources
Reading File
Here is a detailed, evidence-based overview of the latest clinical guidelines on treating premature ejaculation.
Latest Clinical Guidelines on Treating Premature Ejaculation (2025)
Most Current Guideline Source
The EAU (European Association of Urology) 2025 Guidelines on Male Sexual and Reproductive Health - published in July 2025 in European Urology - is currently the most up-to-date authoritative guideline, covering PE diagnosis, treatment, and follow-up based on a systematic review of literature from 2021-2024. (Salonia et al., Eur Urol 2025 - PMID: 40340108). A further limited update was released in March 2026.
Step 1: Classify the Type of PE
Before any treatment, guidelines require subtype classification:
| Type | Description |
|---|---|
| Lifelong PE | Present since first sexual encounter; neurobiological basis; ejaculates in ~1 min always |
| Acquired PE | Develops after a period of normal ejaculation; often due to erectile dysfunction, prostatitis, thyroid disease, or relationship issues |
| Natural variable PE | Occasional, situational; considered a normal variation |
| PE-like ejaculatory dysfunction | Subjective complaint without objective short IELT |
EAU 2025 key rule: For lifelong PE → pharmacotherapy is first-line. For acquired PE → treat the underlying cause first.
If PE is secondary to erectile dysfunction (ED), manage the ED first - once erection quality improves, ejaculatory control often normalizes.
Treatment Algorithm (Campbell-Walsh Wein Urology)
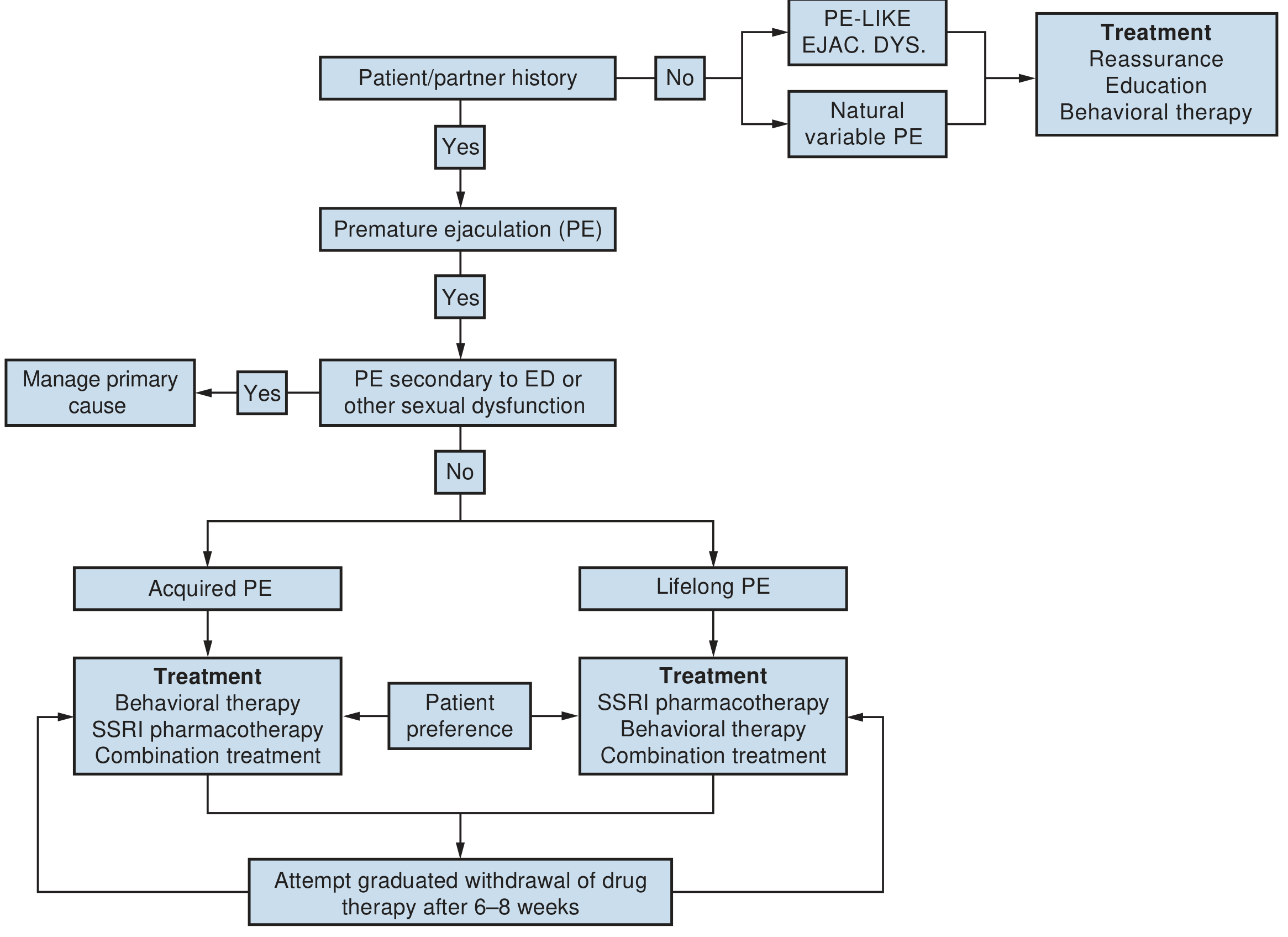
Fig. 71.3. Algorithm for the office management of premature ejaculation - Campbell-Walsh Wein Urology
First-Line Treatments
1. SSRIs (Oral Pharmacotherapy) - Primary First-Line
SSRIs are the most evidence-backed pharmacotherapy for PE. They work by delaying ejaculatory inevitability via serotonin reuptake inhibition.
Daily (chronic) SSRIs:
| Drug | Typical Dose | IELT Fold-Increase |
|---|---|---|
| Paroxetine | 20-40 mg/day | ~8-fold (highest efficacy) |
| Sertraline | 50-200 mg/day | ~4-8 fold |
| Fluoxetine | 20-40 mg/day | ~3-5 fold |
| Clomipramine | 12.5-50 mg/day | ~5 fold |
On-demand therapy:
- Dapoxetine 30-60 mg (taken 1-3 hours before sex) - the only SSRI specifically approved for PE; licensed across Europe, Asia, and many other markets (but not in the USA). Studies show IELT increases from ~0.9 min baseline to ~2.5-3.5 min.
- Clomipramine 15 mg on-demand is also used.
From Goldman-Cecil Medicine: "The first-line treatment for premature ejaculation is SSRIs or a serotonin transporter inhibitor (e.g., dapoxetine 60 mg or clomipramine 15 mg as on-demand therapy) together with behavioral therapy and relationship counseling."
2. Topical Anesthetics - First-Line Alternative
- Lidocaine/prilocaine cream or spray applied to the glans 20-30 minutes before intercourse
- Reduce penile sensitivity and delay ejaculation
- Wash off before intercourse to avoid numbing the partner
- Available OTC in many countries
- Evidence: moderate IELT improvement with good tolerability
Second-Line / Combination Treatments
3. Dapoxetine + PDE5 Inhibitor Combination (Emerging Evidence)
A 2025 meta-analysis of 5 RCTs (498 men) found that dapoxetine + PDE5 inhibitor (e.g., sildenafil, tadalafil) significantly outperforms dapoxetine monotherapy:
- IELT improvement: MD +1.08 min (95% CI: 0.34-1.83, p=0.004)
- Sexual satisfaction scores significantly higher
- Trade-off: higher rates of headache, flushing, nasal congestion
- (Mahesvara et al., 2025 - PMID: 41031773)
This combination is particularly useful when PE co-exists with mild ED or performance anxiety.
4. Alpha-1 Blockers (Emerging)
Silodosin (a selective alpha-1 blocker used for BPH) has shown promise as a new PE treatment. A 2024 meta-analysis of RCTs found it significantly increased IELT with a favorable safety profile (Fauzan et al., Arch Ital Urol Androl 2024 - PMID: 39692416). Mechanism: blocks sympathetic-mediated seminal emission.
5. Off-Label Tramadol (On-Demand)
- Used off-label in some countries at 50 mg on-demand
- Mechanism: weak serotonin/noradrenaline reuptake inhibition + mu-opioid agonism
- Evidence shows IELT increases ~2.5x vs. placebo but is weaker than daily paroxetine (~5-fold vs. 22-fold)
- Concerns: addiction potential, serotonin syndrome risk if combined with SSRIs - use with caution
- A 2021 meta-analysis (PMID: 33566469) confirmed efficacy but called for cautious interpretation
Behavioral and Psychological Therapies
Guidelines strongly recommend these - either alone (especially for acquired/situational PE) or combined with pharmacotherapy:
Classic techniques:
- Stop-start technique (Semans method): Stimulate to near-ejaculatory threshold, stop, repeat - builds ejaculatory control
- Squeeze technique (Masters & Johnson): Squeeze the glans firmly at the ejaculatory threshold to inhibit the reflex
- Pelvic floor (Kegel) exercises: Strengthening the bulbospongiosus muscle improves voluntary control
Psychosexual therapy / CBT:
- Addresses performance anxiety, relationship dynamics, and unrealistic expectations
- A 2025 Frontiers review notes that after 3 months of pelvic floor retraining (3 sessions/week) in men who failed pharmacotherapy, PEDT scores dropped from 16.3 to 10.6 and IELT improved from 50 sec to ~192 sec
Combined (pharmacotherapy + behavioral) is superior to either modality alone - recommended by all major guidelines.
Emerging and Experimental Treatments (2024-2026)
These are not yet standard but appear in recent literature:
| Treatment | Evidence Status |
|---|---|
| Botulinum toxin A injected into bulbospongiosus muscle | RCTs showing efficacy (2024-2025) |
| Transcutaneous posterior tibial nerve stimulation | RCT published 2025 |
| Penile hyaluronic acid injection (glans augmentation) | Small studies, 2025 |
| Acupuncture | Comparative RCT data available (EAU 2026 update) |
| Gene therapy / targeted neurological approaches | Experimental only |
| Traditional Chinese medicine | Systematic review 2023 - evidence insufficient but promising |
| Low-intensity shockwave therapy | Under investigation |
Guideline Summary Table
| Scenario | Recommended Approach |
|---|---|
| Lifelong PE (no ED) | Daily SSRI (paroxetine preferred) OR dapoxetine on-demand + behavioral therapy |
| Acquired PE (with ED) | Treat ED first (PDE5i), then reassess |
| Acquired PE (without ED) | Investigate cause; SSRI + behavioral therapy |
| Mild/situational PE | Education, reassurance, behavioral therapy alone |
| PE + performance anxiety | Dapoxetine + PDE5i + psychosexual counseling |
| SSRI-intolerant patients | Topical anesthetic OR tramadol (off-label, with caution) |
| Failed pharmacotherapy | Pelvic floor therapy, combination strategies, emerging options |
Key References
- EAU 2025 Guidelines - Salonia et al., Eur Urol (PMID 40340108)
- EAU 2026 Full Guideline PDF
- Dapoxetine + PDE5i meta-analysis 2025 (PMID 41031773)
- Silodosin meta-analysis 2024 (PMID 39692416)
- Frontiers comprehensive review 2025
- Goldman-Cecil Medicine; Campbell-Walsh Wein Urology (textbook sources)
This is a shared conversation. Sign in to Orris to start your own chat.