Basics of Mechanical Ventilation for the Neurosurgery Resident
A Neuro-Critical Care Oriented Framework
PART 1 - WHY THE BRAIN MAKES VENTILATION DIFFERENT
Before touching a single knob on the ventilator, you need the physiological framework embedded in your brain.
1.1 The Core Equation
CPP = MAP - ICP
Normal values: CPP (60-70 mmHg) = MAP (90-110 mmHg) - ICP (5-15 mmHg)
Every ventilator decision you make in the Neuro-ICU either protects or threatens this equation. - Bailey and Love's Surgery, 28th Ed.
1.2 Cerebral Blood Flow (CBF) and Its Regulators
Normal CBF = 55 mL/100g/min. Ischemia begins below 20 mL/100g/min. Three master regulators:
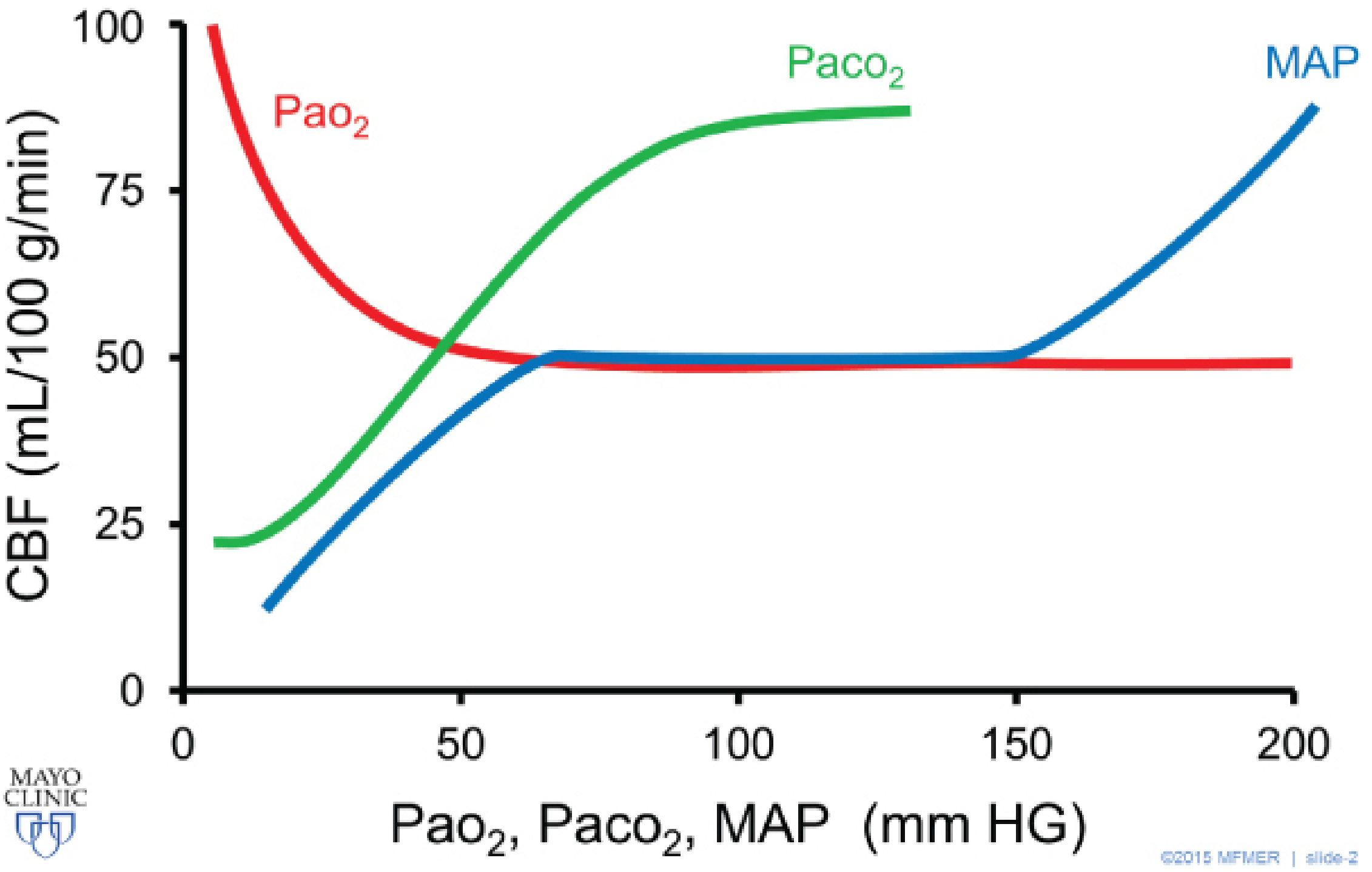
Figure: CBF Autoregulation (Barash Clinical Anesthesia, 9e, Fig 37-7)
CBF remains constant between MAP 60-160 mmHg (blue - autoregulation), varies linearly with PaCO2 20-80 mmHg (green), and stays constant above PaO2 50 mmHg (red).
| Regulator | Relationship to CBF | Clinical implication |
|---|
| PaCO2 | Linear: 1 mmHg change = 1-2 mL/100g/min change | Most powerful ventilator-controlled variable |
| MAP | Autoregulated 60-160 mmHg (normal brain) | Lost in TBI - must actively control |
| PaO2 | Hypoxia (<50 mmHg) causes vasodilation | Keep SpO2 >94% at minimum |
Key principle from Barash: "A change in PaCO2 of 1 mmHg roughly correlates to a similar change in CBF of 1-2 mL/100 g/min. Below PaCO2 20 mmHg, maximal cerebral vasoconstriction leads to tissue hypoxia and a reflex vasodilation." The hyperventilation effect on ICP lasts only ~6 hours as CSF pH renormalizes.
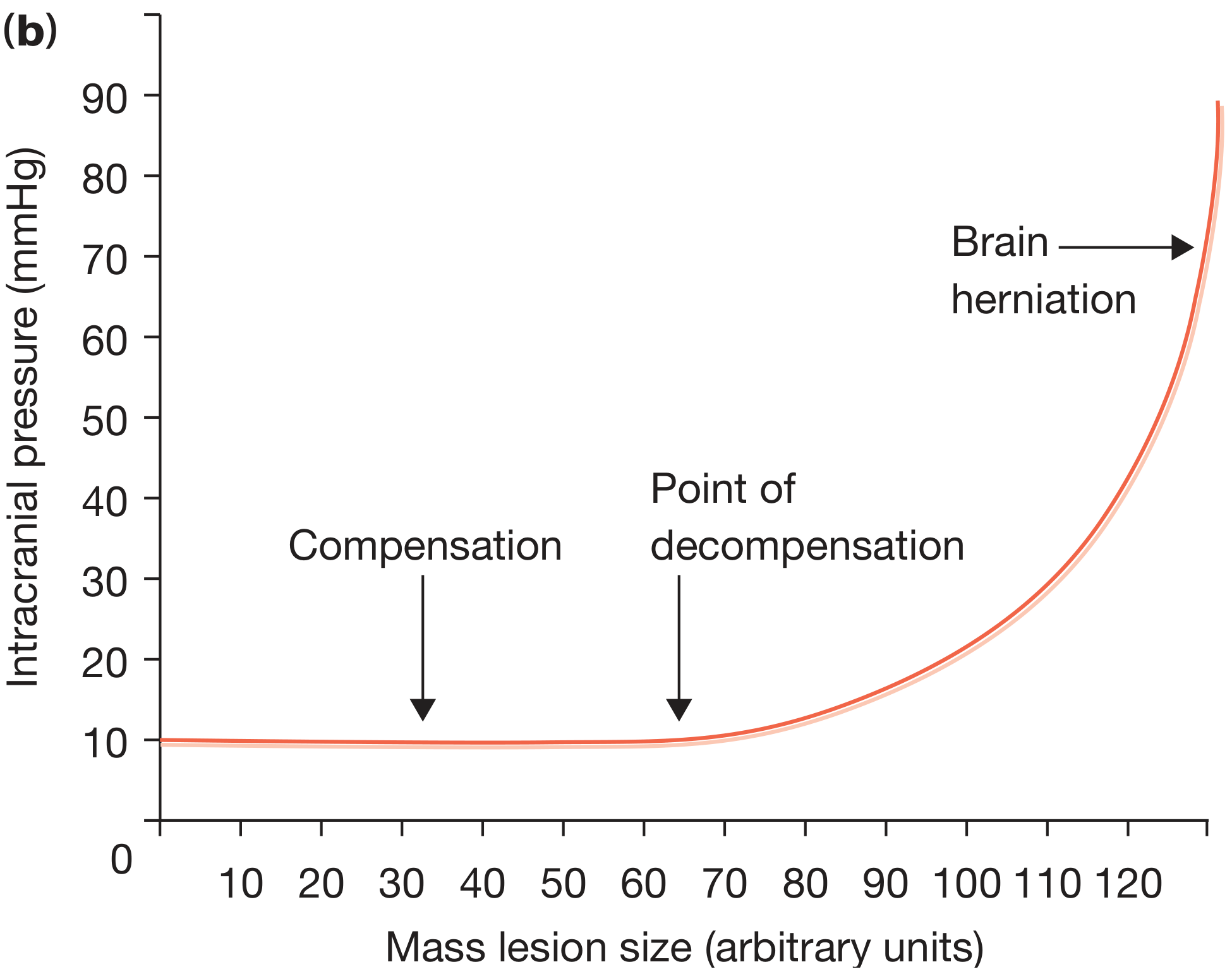
1.3 Monro-Kellie Doctrine - The Ventilator Context
The skull is a rigid box. ICP rises exponentially once compensatory mechanisms (CSF/venous blood shift) are exhausted:
Figure: ICP vs. Mass Lesion (Bailey and Love, 28th Ed.)
What this means for ventilation: The vascular compartment (CBV) is one of the three intracranial volumes. PaCO2 and mean airway pressure both directly manipulate cerebral blood volume. In a patient at the "point of decompensation," small changes in PaCO2 cause disproportionately large ICP swings.
PART 2 - THE VENTILATOR: CORE SETTINGS AND WHAT THEY DO
2.1 The Four Variables of Ventilation (TCLOV Framework)
Every breath is controlled by four interacting variables:
| Variable | What it means | Who sets it |
|---|
| Trigger | What starts the breath (flow/pressure/time) | Patient effort or timer |
| Limit | Maximum value during inspiration (pressure or flow) | Clinician |
| Cycle | What ends inspiration (volume, time, flow%) | Clinician/Ventilator |
| Baseline | End-expiratory pressure (PEEP) | Clinician |
2.2 The Core Parameters - Every One Mapped to Neuro-Physiology
A. TIDAL VOLUME (Vt)
What it is: Volume of gas delivered per breath. Usually set as mL/kg of Ideal Body Weight (IBW) - not actual weight.
- Standard lung-protective: 6-8 mL/kg IBW
- In neurological patients, this is non-negotiable - high Vt raises plateau pressure, raises Pmean, raises thoracic pressure, impairs venous drainage, raises ICP
IBW Formula:
- Males: 50 + 0.91 × (height in cm - 152.4)
- Females: 45.5 + 0.91 × (height in cm - 152.4)
Neuro scenarios:
| Patient | Vt target | Reasoning |
|---|
| Severe TBI, ICP 28 mmHg | 6 mL/kg IBW | Minimize Pmean, avoid high airway pressures |
| Post-op posterior fossa (Day 1) | 6-7 mL/kg IBW | Brain swelling risk, lung protection |
| SAH (Hunt-Hess 4, no lung injury) | 7-8 mL/kg IBW | Lung protection, maintain PaCO2 35-40 |
| MCA infarct + aspiration pneumonia | 6 mL/kg IBW strictly | ARDS protocol applies simultaneously |
B. RESPIRATORY RATE (RR)
What it is: Number of machine-delivered breaths per minute. Together with Vt, determines minute ventilation (MV).
MV = Vt × RR
PaCO2 is inversely proportional to MV (alveolar ventilation)
This is your primary PaCO2 control knob. In neuro patients, RR is the most powerful tool you have.
Targets by scenario:
| Situation | PaCO2 Target | RR Adjustment |
|---|
| Routine neuro-ICU ventilation | 35-40 mmHg (normocarbia) | 12-16/min |
| Acute ICP crisis / herniation (short-term) | 30-35 mmHg (controlled hyperventilation) | 18-22/min |
| Post-cardiac arrest neuroprotection | 35-45 mmHg (strict normocarbia) | Titrate to ABG |
| SAH with vasospasm | 35-40 mmHg | Avoid hypocarbia (causes vasoconstriction in already spastic vessels) |
Clinical warning: Chronic prophylactic hyperventilation (PaCO2 <35) is contraindicated in TBI except as a temporizing bridge. The Brain Trauma Foundation (BTF) guidelines: "Hyperventilation is recommended as a temporizing measure for reduction of elevated ICP. Prophylactic hyperventilation is not recommended in the first 24 hours after injury." - Barash Clinical Anesthesia, Table 57-2
C. FiO2 (Fraction of Inspired Oxygen)
What it is: Proportion of oxygen in delivered gas (0.21-1.0 = 21%-100%)
Brain physiology: CBF remains constant above PaO2 50 mmHg. Below this, cerebral vasodilation raises CBF and ICP.
- Target SpO2 >94% (SaO2 ≥95% per BTF guidelines - Barash Table 57-2)
- Avoid hyperoxia (PaO2 >200 mmHg) - associated with free radical injury and worse neurologic outcomes (Miller's Anesthesia, 10e)
- FiO2 >0.6 risks pulmonary oxygen toxicity - reduce with PEEP if possible
Practical rule: Start at FiO2 1.0 post-intubation. Once stable with continuous monitoring (SpO2, ETCO2), titrate down to keep SpO2 94-98%.
D. PEEP (Positive End-Expiratory Pressure)
What it is: Residual positive pressure maintained in the airways at end-expiration.
Pulmonary purpose: Prevents alveolar collapse (microatelectasis), improves FRC, allows FiO2 weaning.
The PEEP-ICP Problem:
High PEEP → ↑ intrathoracic pressure → ↓ venous return →
↑ jugular venous pressure → ↓ cerebral venous drainage →
↑ cerebral blood volume → ↑ ICP
This pathway is most dangerous when:
- The patient is hypovolemic
- ICP is already elevated
- Lung compliance is normal (PEEP effect transmitted directly to vessels)
Evidence from Bradley & Daroff's Neurology in Clinical Practice:
"Patients with decreased intracranial compliance may develop increases in ICP as intrathoracic pressure rises and imposes resistance to venous return. However, for the most part, relatively high levels of PEEP are well tolerated by euvolemic patients with intracranial hypertension."
Practical PEEP targets in neuro patients:
| Scenario | PEEP Target | Notes |
|---|
| Normal lungs, ICP normal | 5 cmH2O (physiologic) | Standard |
| Normal lungs, ICP elevated | 5-8 cmH2O | Keep head 30° elevated, ensure euvolemia |
| ARDS + Neuro-ICU | 8-12 cmH2O (titrated) | Monitor ICP closely; PEEP >8 risks ICP elevation |
| Post-op posterior fossa | 5 cmH2O initially | Posterior fossa edema - avoid high intrathoracic pressure |
| Patient with aspiration + high ICP | 8 cmH2O max | Consider ICP monitor if using >8 cmH2O |
Roberts & Hedges' Emergency Medicine: "PEEP levels higher than 8 cm H2O in the setting of elevated ICP, unilateral lung processes, hypotension, hypovolemia, or pulmonary embolism" require caution.
E. INSPIRATORY FLOW RATE & I:E RATIO
What it is: How fast gas is delivered; determines the ratio of inspiratory to expiratory time.
- Normal I:E ratio = 1:2 (inspiration takes 1 part, expiration 2 parts)
- In neurosurgical patients: maintain normal or even longer expiratory time (1:2 to 1:3)
- Short expiratory time → air trapping → auto-PEEP → unpredictable elevation of mean airway pressure → elevated ICP
Auto-PEEP in neuro-ICU:
- Breath stacking raises effective PEEP unpredictably - the ICP impact is then also unpredictable
- Check for auto-PEEP: perform an expiratory hold maneuver at bedside; any pressure above 0 at end-expiration = auto-PEEP
PART 3 - VENTILATOR MODES (Relevant to Neuro-ICU)
3.1 Mode Classification
Controlled Modes (no patient trigger required)
├── Volume Control (VC-AC): Fixed Vt delivered
└── Pressure Control (PC): Fixed pressure delivered, Vt varies
Assisted/Support Modes (patient triggers each breath)
├── SIMV (Synchronized IMV): Set mandatory rate + patient-triggered extras
├── Pressure Support (PSV): Patient-triggered, pressure-assisted
└── MMV (Mandatory Minute Ventilation): Hybrid backup
Hybrid Modes
└── PRVC / Volume-assured PS: Pressure-limited but volume-targeted
3.2 Volume Control Assist-Control (VC-AC) - The Default Neuro-ICU Mode
How it works:
- You set: Vt, RR, FiO2, PEEP, flow rate
- Ventilator delivers exactly the set Vt on every breath (mandatory and patient-triggered)
- The airway pressure varies breath-to-breath depending on lung compliance
Advantages for neurological patients:
- Guaranteed minute ventilation - you are guaranteed your PaCO2 target
- If patient has agitation/coughing/dyssynchrony, Vt is still delivered
- Predictable CO2 control = predictable CBF/ICP
Disadvantage:
- If patient bites tube, coughs, or fights the ventilator, Peak Inspiratory Pressure (PIP) spikes - set pressure alarm to alert you
- Does NOT protect against high pressures by itself (use plateau pressure monitoring)
Waveform appearance (VC-AC):
- Pressure-Time curve: Rectangular rise to plateau, then fall - the "square-wave" plateau
- Flow-Time curve: Constant (square wave) during inspiration with abrupt cutoff
- Volume-Time curve: Linear ramp up, plateau at Vt, then drops to baseline
In the Neuro-ICU, always check:
- Plateau pressure (Pplat): Perform an inspiratory hold. Pplat should be <30 cmH2O (lung protective). Pplat reflects alveolar pressure and mean airway pressure impact on venous drainage.
- Driving pressure = Pplat - PEEP: Target <15 cmH2O. High driving pressure = over-distension = worsening brain physiology.
3.3 Pressure Control (PC-AC)
How it works:
- You set: Inspiratory pressure (above PEEP), RR, FiO2, PEEP, inspiratory time
- Delivers a fixed pressure - Vt is variable depending on lung compliance
- If lung compliance changes (pneumonia, tension pneumothorax, bronchospasm), Vt changes silently
Relevance to neuro-ICU:
- Used in paralyzed/deeply sedated patients (poor-grade SAH, acute herniation)
- Can provide more comfortable breath patterns in partially awake patients
- Risk: If you're not watching volumes closely, silent hypoventilation → PaCO2 rise → ICP crisis
- Bradley & Daroff's Neurology: "Pressure-control ventilation is used most frequently in patients who are sedated and paralyzed and is overall an uncommon ventilatory mode in the NICU."
Practical rule for neuro-ICU: If using PC mode, set a low-tidal-volume alarm (<5 mL/kg IBW) to catch compliance changes early.
3.4 Pressure Support Ventilation (PSV) - The Weaning Mode
How it works:
- Patient triggers every breath
- Ventilator augments each breath with a set pressure boost
- Breath ends when flow drops to 20% of peak
- No mandatory backup rate (except apnea alarm setting)
Neuro-ICU applications:
- Weaning phase in patients recovering from TBI or post-op posterior fossa
- Spontaneous breathing trials (SBT) before extubation
- Often combined with SIMV during transition
Danger in neuro-ICU: If GCS drops, apnea can go undetected. Always set apnea backup rate. - Bradley & Daroff's
3.5 SIMV (Synchronized Intermittent Mandatory Ventilation)
How it works:
- Delivers a set number of mandatory breaths (VC or PC) synchronized with patient effort
- Patient can breathe spontaneously between mandatory breaths (usually with pressure support added)
- Mandatory minute ventilation (MMV) is a variant that adjusts mandatory rate to patient effort
Weaning in neuro-ICU: "Weaning from mechanical ventilation is usually achieved in critically ill neurological patients by decreasing the rate of mandatory breaths on SIMV or, more commonly, by using PSV." - Bradley & Daroff's Neurology
PART 4 - WAVEFORM ANALYSIS FOR THE NEURO-ICU RESIDENT
Understanding waveforms tells you what is actually happening to the patient, not what you set.
4.1 Normal Waveform Patterns
PRESSURE-TIME (VC mode):
_______
| |
_____| |____
PEEP PEEP
PIP = peak, followed by Pplat if hold applied
FLOW-TIME (VC mode, square wave):
___________
| |
| |________ (inspiratory)
↓
__________| (expiratory - decelerating)
|_________
VOLUME-TIME:
/\
/ \
/ \
____/ \____
(ramp up, ramp down)
4.2 Dyssynchrony Detection - Critical for Neuro-ICU
Patient-ventilator dyssynchrony (PVD) is a neurological emergency trigger in the NICU. Agitation from dyssynchrony raises ICP through Valsalva-like intrathoracic pressure swings.
A. Double Triggering
- What it looks like: Two volume spikes appearing immediately one after the other before expiration is complete
- Pressure-time curve: Two pressure peaks very close together
- Volume-time: Volume appears to stack
- Cause: Patient's neural inspiratory time is longer than machine's set inspiratory time
- Neuro consequence: Stacked breaths = large Vt delivered = high Pmean = ICP spike
- Fix: Increase inspiratory time on ventilator, or deepen sedation
B. Flow Starvation / Inadequate Flow
- What it looks like: On the pressure-time curve, instead of the normal rise to a plateau, you see a scalloped, scooped-out concavity on the upstroke
- Cause: Patient's inspiratory demand exceeds delivered flow rate
- Neuro consequence: Patient fighting the ventilator = increased work of breathing = agitation = ICP elevation
- Fix: Increase peak flow rate (e.g., from 40 to 60 L/min), or switch to PSV/PC which matches patient demand better
C. Auto-PEEP / Air Trapping
- What it looks like: On the flow-time curve, expiratory flow does not return to zero before the next breath starts
- The baseline of the flow-time tracing is shifted above the zero line on the expiratory side
- Volume-time: Volume does not return to baseline between breaths (stair-stepping pattern)
- Confirm: Expiratory hold maneuver - any pressure reading at end expiration
- Neuro consequence: Auto-PEEP acts like applied PEEP but is hidden - unpredictable ICP elevation
- Fix: Reduce RR, increase expiratory time (lower I:E), treat bronchospasm
D. Ineffective Effort (Missed Triggers)
- What it looks like: A small deflection in the pressure-time curve (patient effort) that is NOT followed by a ventilator breath
- Cause: Trigger threshold too high, or patient effort too weak (deep sedation, neuromuscular weakness)
- Neuro relevance: Can cause respiratory acidosis if patient is relying on spontaneous breaths; also indicates over-sedation
PART 5 - CLINICAL NEUROSURGICAL SCENARIOS
SCENARIO 1: Severe TBI, GCS 6, ICP 32 mmHg, CPP 54 mmHg
Patient: 28M, RTA. Left frontal contusion + right EDH evacuated 6h ago. ICP monitor in-situ. On propofol infusion.
Ventilator Strategy:
| Parameter | Setting | Rationale |
|---|
| Mode | VC-AC | Guaranteed Vt and MV for PaCO2 control |
| Vt | 6 mL/kg IBW | Lung-protective, minimize Pmean |
| RR | 16-18/min | Target PaCO2 35-40 mmHg initially |
| FiO2 | Titrate to SpO2 >94% | Avoid hypoxia (vasodilatation → ICP) |
| PEEP | 5 cmH2O | Physiologic PEEP only while ICP elevated |
| Flow rate | 60 L/min | Avoid flow starvation, minimize dyssynchrony |
| I:E ratio | 1:2 to 1:3 | Prevent auto-PEEP |
ICP spike management (PaCO2 as acute tool):
- Acute ICP crisis (pupil dilation, Cushing response): increase RR to 20-22, target PaCO2 30-35 mmHg as BRIDGE
- This is a temporizing measure only - simultaneously call for CT, consider surgical review
- Do NOT maintain PaCO2 <35 chronically (ischemia risk, only ~6 hours efficacy)
- Per Barash Table 57-2: Target SaO2 ≥95%, PaCO2 35-40 Torr as standard ICU goal
Head positioning: 30-45° head of bed elevation always - this dramatically improves venous drainage independent of ventilator
SCENARIO 2: Poor-Grade SAH (Hunt-Hess 4, Fisher 3), Day 3, Vasospasm Risk
Patient: 55F, sudden-onset headache, GCS 9. CT: diffuse thick SAH. Aneurysm coiled. Now on triple-H prophylaxis.
Key differences from TBI:
- Cerebral vasospasm (days 3-14) can be worsened by hypocarbia - avoid PaCO2 <35
- Sympathetic surge can cause neurogenic pulmonary edema - lungs may be worse than expected
- Need to maintain or augment CPP (hypertensive therapy) while ventilating
Ventilator Strategy:
| Parameter | Setting | Rationale |
|---|
| Mode | VC-AC | PaCO2 control paramount |
| Vt | 7-8 mL/kg IBW | Normocarbia target, slightly higher if lungs OK |
| RR | 12-14/min | Target PaCO2 38-42 mmHg - mild permissive normocarbia |
| PEEP | 5-8 cmH2O | Balance lung recruitment vs. venous drainage |
| FiO2 | Target PaO2 100-200 mmHg | Neurogenic pulmonary edema may require higher FiO2 |
Special concern: If developing vasospasm - do not hyperventilate. PaCO2 <35 further vasoconstricts already spastic cerebral vessels → ischemia in the territory of the aneurysm.
SCENARIO 3: Large MCA Infarct with Malignant Edema, Day 2
Patient: 67M, right MCA territory infarct, rapid swelling. GCS deteriorating. ICP 24 mmHg.
Key pathophysiology: Autoregulation is severely impaired in the infarcted hemisphere. The penumbra (ischemic but salvageable tissue) is exquisitely sensitive to CPP drops. On the other hand, hypercarbia will cause global vasodilation - potentially a "steal" phenomenon where blood goes to healthy brain, not penumbra.
Ventilator Strategy:
| Parameter | Setting | Rationale |
|---|
| Mode | VC-AC | Controlled MV |
| PaCO2 Target | 35-40 mmHg strictly | Avoid both hypercarbia (ICP) and hypocarbia (penumbral ischemia) |
| PEEP | 5 cmH2O | Minimize venous obstruction, monitor ICP |
| Vt | 6-7 mL/kg IBW | Lung protection |
Decompressive hemicraniectomy post-op: After DHC, the brain can herniate outward through the defect. ICP monitor still useful. PEEP management same as above.
SCENARIO 4: Post-Op Posterior Fossa Craniectomy for Cerebellar Hemorrhage - Early Post-Op
Patient: 58F, right cerebellar hemorrhage 4 cm. Underwent suboccipital craniectomy + evacuation. Day 1 post-op.
Special concerns:
- Posterior fossa edema peaks 24-72 hours post-op - highest risk of brainstem compression
- Brainstem is immediately behind the operative field - any venous congestion = catastrophic
- EVD often placed for 4th ventricle/hydrocephalus management
- Patient position: HOB 30°, avoid neck flexion (impairs venous drainage)
Ventilator Strategy:
| Parameter | Setting | Rationale |
|---|
| Mode | VC-AC Day 1-2, then PSV for weaning | Controlled phase first |
| Vt | 6-7 mL/kg IBW | Minimize Pmean |
| RR | 14-16/min | PaCO2 35-40 mmHg |
| PEEP | 5 cmH2O max initially | Posterior fossa: high intrathoracic pressure = brainstem venous congestion |
| FiO2 | Titrate to SpO2 >95% | Standard |
Weaning & Extubation:
- Wean SIMV rate or PS gradually as GCS improves
- Extubation requires both ventilatory criteria AND neurological criteria
- Neurological criteria for extubation: GCS ≥8, airway reflexes intact, able to follow commands, no impending ICP crisis
- Per Bradley & Daroff: "Keeping patients intubated once they have fulfilled the ventilatory criteria for extubation is a common but questionable practice. In patients with TBI, this practice may be associated with a higher risk of ventilator-associated complications."
SCENARIO 5: The "Tight Brain" Intraoperatively (MCh Neurosurgery Relevance)
Context: Your patient is in the operating room, the dura is opened, and the brain is bulging. The anesthesiologist asks for your input.
Your checklist (VENTILATION contributions to brain relaxation):
- PaCO2: Confirm ETCO2 showing ~32-35 mmHg. Ask anesthesiologist to target PaCO2 30-35 mmHg with hyperventilation. Effect peaks in 2-5 minutes.
- PEEP: Temporarily reduce PEEP to 3-5 cmH2O if safe from oxygen standpoint
- Vt check: Ensure 6-8 mL/kg IBW, not higher
- FiO2: Avoid high FiO2 unnecessarily, but SpO2 >95% is mandatory
- Position: Confirm HOB slightly elevated if possible, neck neutral
- Concurrent measures: Mannitol 0.5-1 g/kg IV, CSF drainage via EVD if present
PART 6 - QUICK-REFERENCE TARGET TABLE FOR NEURO-ICU
| Parameter | Standard Neuro-ICU | Acute ICP Crisis | Vasospasm (SAH) | Post-op Day 1 |
|---|
| Mode | VC-AC | VC-AC | VC-AC | VC-AC → PSV |
| Vt | 6-7 mL/kg IBW | 6 mL/kg IBW | 7-8 mL/kg IBW | 6-7 mL/kg IBW |
| RR | 12-16/min | 18-22/min | 12-14/min | 12-14/min |
| PaCO2 Target | 35-40 mmHg | 30-35 mmHg (bridge) | 38-42 mmHg | 35-40 mmHg |
| PEEP | 5 cmH2O | 5 cmH2O | 5-8 cmH2O | 5 cmH2O |
| FiO2 | Titrate SpO2 >94% | 1.0 initially | Titrate | Titrate |
| Head Position | 30-45° HOB | 30° HOB | 30° HOB | 30° HOB |
| Pplat Target | <30 cmH2O | <30 cmH2O | <30 cmH2O | <30 cmH2O |
PART 7 - KEY CLINICAL PEARLS FOR YOUR MCh ORAL EXAM
-
PaCO2 is your most powerful ventilator-brain dial. 1 mmHg PaCO2 change = 1-2 mL/100g/min CBF change. This is linear between 20-80 mmHg. Below 20 mmHg: reflex vasodilation (ischemia-driven).
-
Hyperventilation is a bridge, not a destination. Effect lasts ~6 hours due to CSF pH renormalization. Using it prophylactically in the first 24 hours post-TBI is harmful (BTF Guideline, Level II evidence).
-
PEEP raises ICP only in hypovolemic patients with poor lung compliance. Euvolemic patients tolerate moderate PEEP (5-10 cmH2O) well.
-
Auto-PEEP is invisible PEEP. Always check the flow-time curve for failure of expiratory flow to return to zero.
-
Dyssynchrony is an ICP crisis in disguise. A fighting patient generates intrathoracic pressure swings = impaired cerebral venous drainage = ICP spikes. Fix synchrony first (flow, sedation, mode adjustment) before just deepening sedation reflexively.
-
VC-AC mode gives you guaranteed PaCO2 control - the paramount concern in neuro patients. PC mode is acceptable but requires vigilant Vt alarms.
-
Extubation in neuro-ICU requires BOTH criteria: ventilatory readiness (RSBI <105, adequate effort, SpO2 on minimal support) AND neurological readiness (GCS ≥8, airway reflexes, no impending herniation risk).
-
The CPP target in TBI is 60-70 mmHg (BTF 4th edition). Above 70 mmHg increases ARDS risk through aggressive vasopressor use. Below 60 mmHg risks ischemia.
Sources:
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - Cerebral physiology, TBI management
- Bradley & Daroff's Neurology in Clinical Practice - Neuro-ICU ventilation modes, PEEP and ICP, extubation
- Bailey and Love's Surgery, 28th Ed. - ICP physiology, Monro-Kellie, CPP
- Miller's Anesthesia, 10e - Post-arrest ventilation, PaCO2 targets
- Roberts & Hedges' Clinical Procedures in Emergency Medicine - PEEP thresholds
- Brain Trauma Foundation (BTF) Guidelines, 4th Edition - CPP targets, hyperventilation recommendations