Na 118, Plasma osmolality 253, Urine osmolality 366, Urine Na <20 whats the picture for hyponatremia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
This is a classic picture. Here's the full analysis:
Hyponatremia Classification from These Values
| Parameter | Value | Interpretation |
|---|---|---|
| Serum Na⁺ | 118 mEq/L | Severe hyponatremia |
| Plasma osmolality | 253 mOsm/kg | Hypotonic (true hyponatremia) |
| Urine osmolality | 366 mOsm/kg | Concentrated urine (>100 mOsm/kg — kidney retaining water) |
| Urine Na⁺ | <20 mEq/L | Avid Na⁺ reabsorption by kidney |
Step-by-Step Reasoning
Step 1 — Is this true hyponatremia?
Plasma osmolality 253 mOsm/kg confirms this is hypotonic (true) hyponatremia, not pseudohyponatremia (hyperlipidemia/hyperproteinemia) or hypertonic hyponatremia (hyperglycemia, mannitol).
Step 2 — Is the kidney appropriately diluting urine?
No. Urine osmolality of 366 mOsm/kg means the urine is more concentrated than plasma — ADH is active and the kidney is retaining free water. This rules out primary polydipsia (which would give very dilute urine <100 mOsm/kg).
Step 3 — What does urine Na⁺ <20 tell us?
This is the critical discriminator. Low urine Na⁺ (<20 mEq/L) means the kidney is aggressively holding onto sodium — indicating:
- The kidney senses the body as sodium/volume-depleted, OR
- There is a hypervolemic state driving avid sodium reabsorption via RAAS/SNS activation
The Picture: Hypervolemic Hyponatremia (most likely) OR Hypovolemic Hyponatremia with extrarenal losses
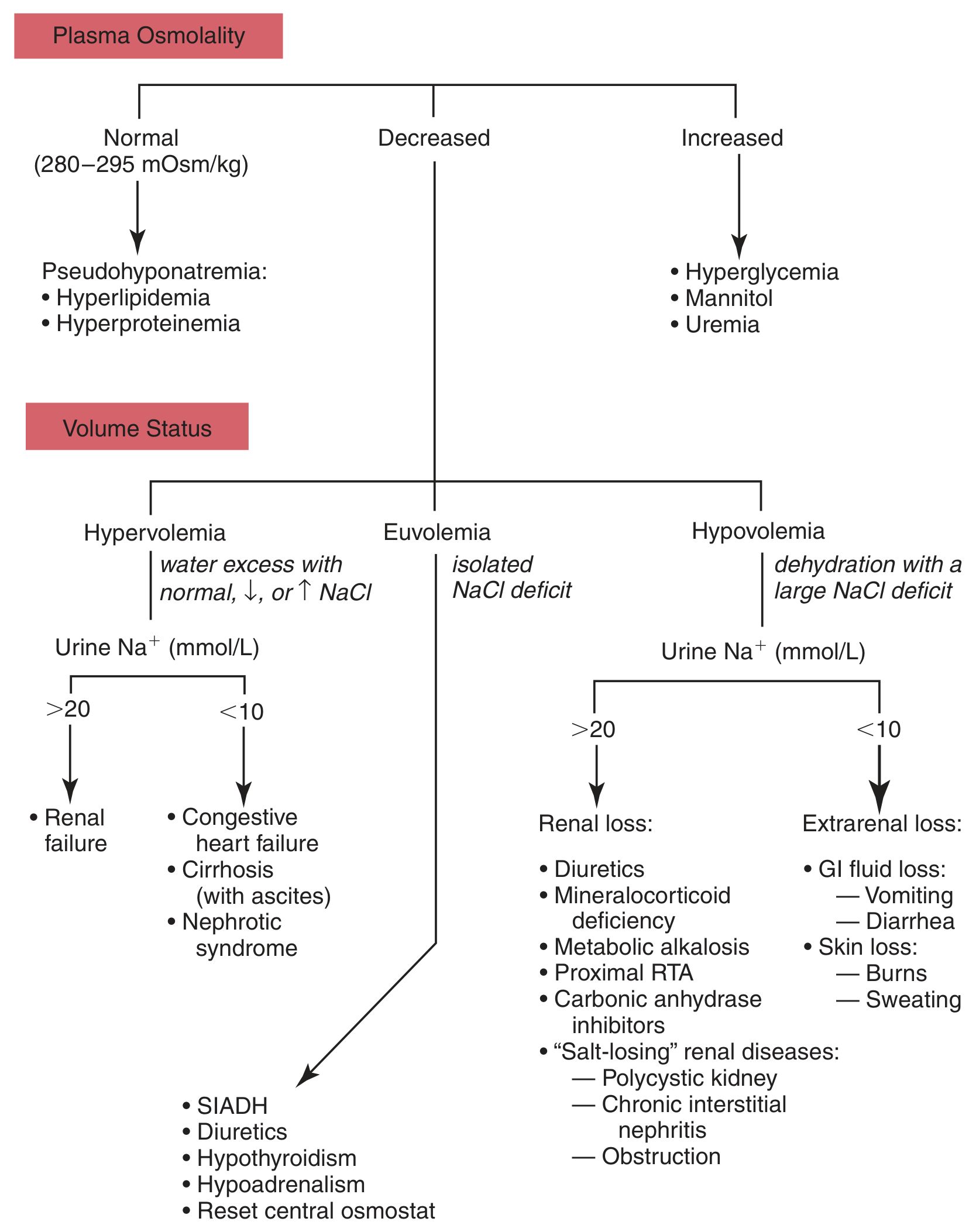
Algorithm for differential diagnosis of hyponatremia — Tietz Textbook of Laboratory Medicine, 7th Edition
Following the algorithm with decreased plasma osmolality + urine Na⁺ <20 mEq/L:
Most likely diagnoses:
Hypervolemic (clinically edematous):
- Congestive heart failure — reduced effective arterial blood volume → RAAS activation → Na⁺ retention + ADH release → dilutional hyponatremia with low urine Na⁺
- Cirrhosis with ascites — portal hypertension → splanchnic vasodilation → perceived underfilling → same mechanism
- Nephrotic syndrome — low oncotic pressure → reduced EABV → same mechanism
Hypovolemic (extrarenal losses):
- GI losses (vomiting, diarrhea) — Na⁺ and water lost, replaced with free water → hyponatremia; kidney conserves Na⁺ (urine Na⁺ <20) while ADH is stimulated by volume depletion → concentrated urine
- Skin losses (burns, sweating)
Key Distinguishing Point
The combination of concentrated urine (Uosm 366) + low urine Na⁺ (<20) is the hallmark of non-renal sodium retention — the kidney is doing its job correctly by conserving Na⁺, but systemic volume/pressure sensing is driving ADH release inappropriately (in hypervolemic states) or appropriately (in hypovolemia).
This rules out SIADH (which would show urine Na⁺ >20–40 mEq/L and euvolemia).
Summary
| This patient | SIADH | Primary polydipsia | |
|---|---|---|---|
| Plasma osm | ↓ 253 | ↓ | ↓ |
| Urine osm | ↑ 366 | ↑ (>100) | ↓ (<100) |
| Urine Na⁺ | <20 | >20 | Low/variable |
| Volume status | Hypervolemic or hypovolemic | Euvolemic | Euvolemic |
Bottom line: This is hypotonic hyponatremia with concentrated urine and low urine Na⁺ — pointing to hypervolemic hyponatremia (CHF, cirrhosis, nephrotic syndrome) or hypovolemic hyponatremia from extrarenal (GI/skin) losses. Clinical volume assessment (JVP, edema, orthostatic BP) is essential to distinguish between them.
— Goldman-Cecil Medicine, p. 1201; Tietz Textbook of Laboratory Medicine 7th Ed., p. 1938–1939
This is a shared conversation. Sign in to Orris to start your own chat.