Subsegmental pulmonary embolism , Subsegmental images
Reading File
Finding Sources
Searching PubMed
"subsegmental pulmonary embolism" AND management
Searching the Web
subsegmental pulmonary embolism CT imaging radiology images findings 2024
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading Article
PMID: 37871632
Reading Article
PMID: 41962426
Reading File
Loading Image
Searching the Web
subsegmental pulmonary embolism CTPA CT scan axial coronal image filling defect radiology
Loading Image
Loading Image
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC6039809
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive content and images. Let me compile the full answer.
Subsegmental Pulmonary Embolism (SSPE)
Definition and Anatomy
Subsegmental pulmonary embolism (SSPE) refers to thrombus lodged in the subsegmental (fourth-order) pulmonary arteries - the branches distal to the segmental arteries. These vessels are typically <3 mm in diameter on CT and are the smallest branches routinely visualized on CT Pulmonary Angiography (CTPA). SSPE represents clot burden limited to the periphery of the pulmonary vasculature, without involvement of the main, lobar, or segmental branches.
The pulmonary artery hierarchy is:
- Main pulmonary artery → Lobar arteries → Segmental arteries → Subsegmental arteries → sub-subsegmental arteries
CT Imaging: The Key Modality
CTPA is the primary diagnostic test. With modern 64+ detector-row scanners, SSPE can be detected at sub-millimeter resolution in the lower lobe subsegmental branches, where ~90% of emboli occur (preferentially due to greater blood volume and gravitational effect).
Imaging Appearances on CTPA
Direct Signs (Filling Defects)
1. "Polo Mint" / "Doughnut" Sign
When the subsegmental artery is imaged orthogonal to its long axis:
- Central low-attenuation filling defect (thrombus)
- Surrounded by a peripheral rim of enhancing contrast
- Gives a "polo mint" or ring appearance
2. "Railway Sign" / "Tram-Track Sign"
When imaged parallel to the vessel long axis:
- Central low-density filling defect flanked by two parallel lines of contrast
- Indicates non-occlusive thrombus
3. Occlusive Filling Defect
- Complete absence of contrast within an expanded subsegmental vessel
- The affected vessel may appear slightly dilated
- Arrowhead-shaped defect at the branch point
4. Mural/Eccentric Defect
- Low-density thrombus abutting one side of the vessel wall
- Forms an acute angle with the vessel wall (distinguishes acute from chronic PE, which forms obtuse angles)
Textbook Images
Image 1: Solitary Subsegmental PE on CTPA with V/Q Correlation
(Murray & Nadel's Textbook of Respiratory Medicine, eFigure 20.54)
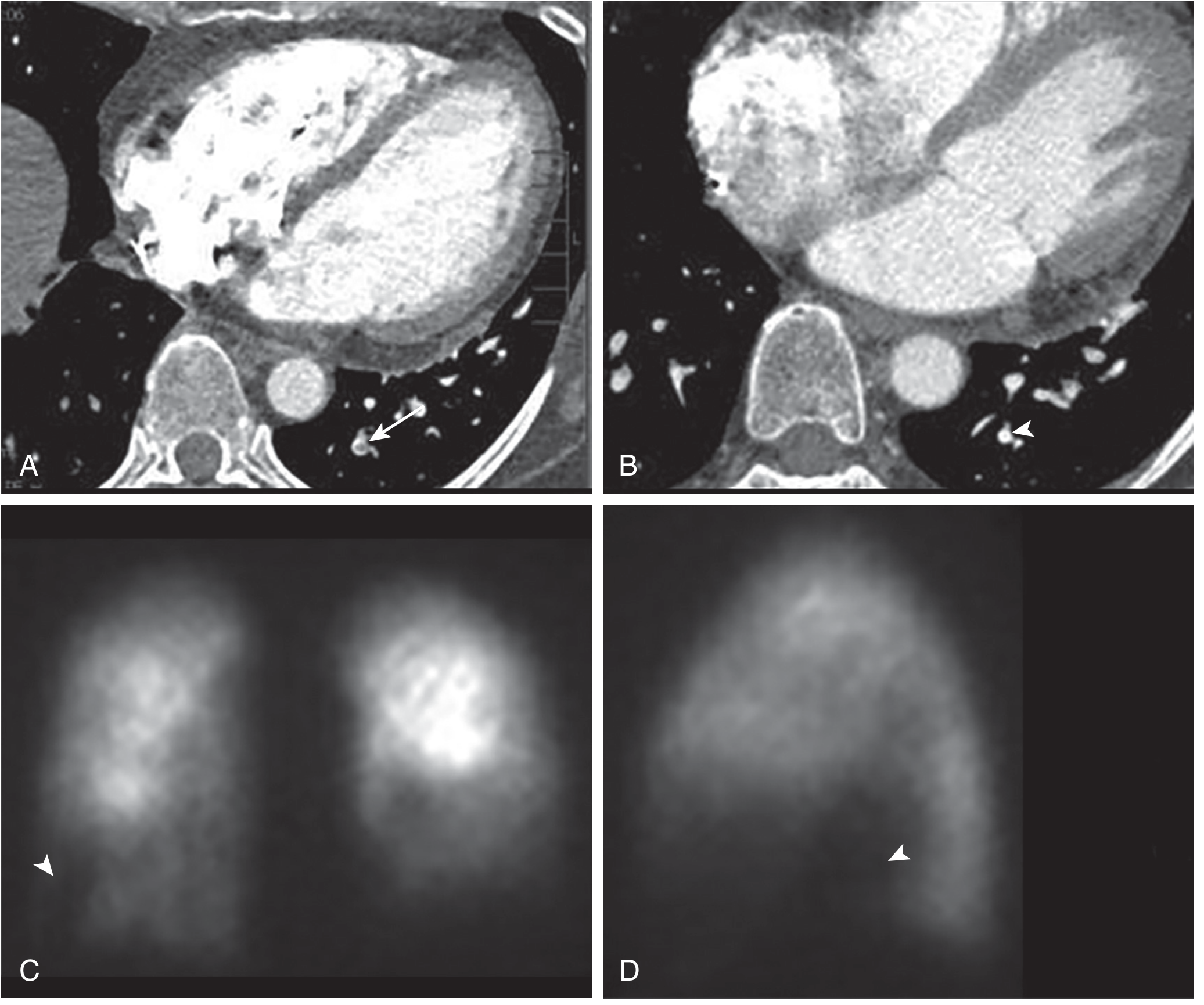
Panel A - Axial CTPA: Small intraluminal filling defect (arrow) in a posterior subsegmental left lower lobe pulmonary artery - the only PE detected in this study.
Panel B - Prior CTPA (>1 year earlier): The same vessel (arrowhead) is widely patent, confirming this is a new finding.
Panels C & D - V/Q Scintigraphy (posterior and left lateral projections): Perfusion defect (arrowheads) in the left base, confirming the CTPA finding - performed because only a solitary third-order SSPE was found and lower extremity ultrasound was negative for DVT.
Image 2: Radiopaedia - PE at the Subsegmental Level (Axial CTPA)

Axial CTPA: filling defect visible in a peripheral artery with good pulmonary arterial opacification, illustrating why thin-slice acquisition and appropriate window/level settings are essential for SSPE detection.
Technical Requirements for SSPE Detection
| Parameter | Recommendation |
|---|---|
| Slice thickness | ≤1 mm (ideally 0.625 mm) |
| Contrast timing | Bolus tracking - pulmonary trunk >200 HU |
| Reconstruction | Thin-slab MIP (3-5 mm) in axial, coronal, sagittal |
| Window setting | Mediastinal window (W:400, L:40) + lung window |
Pitfalls and Artifacts (Important for SSPE Specifically)
SSPE is uniquely prone to false positives and false negatives:
| Pitfall | Mimicker | How to Distinguish |
|---|---|---|
| Partial volume averaging | Hilar lymph nodes adjacent to small arteries | Review in all 3 planes; true PE persists on all views |
| Mucus-filled bronchi | Wall enhancement mimics filling defect | Identify adjacent normally-enhancing artery; trace bronchus on contiguous images |
| Flow artifact from downstream atelectasis | Low-attenuation "filling defect" | ROI attenuation >120 HU suggests artifact; repeat CT or delay scan |
| Cardiac/respiratory motion | Blurring of small vessels | ECG-gating; breath-hold technique |
| Pulmonary venous pseudo-filling defect | Mistaken for arterial PE | Early arterial phase acquisition; trace vessel back to left atrium |
Reported inter-observer variability for SSPE is substantially higher than for central or lobar PE - some studies report agreement rates as low as 25% among experienced radiologists for isolated subsegmental findings.
Incidence and Epidemiology
SSPE now accounts for approximately 15-20% of all CT-diagnosed PE - a figure that has risen sharply with the adoption of multidetector CTPA replacing single-detector scanners. Many of these represent incidental findings or clinically insignificant clots that would not have been detected on prior-generation imaging.
Clinical Significance and Prognosis
SSPE has a more benign natural history than proximal PE:
- Lower rates of hemodynamic compromise
- Lower short-term mortality
- Lower rate of right ventricular dysfunction
- Many patients have underlying cardiopulmonary reserve sufficient to compensate
However, SSPE is not always benign - particularly when:
- Multiple subsegmental vessels involved bilaterally
- Coexisting DVT is present
- Patient has poor cardiopulmonary reserve (cancer, COPD, heart failure)
- Patient is pregnant or anticoagulation was recently stopped
Management: Anticoagulation vs. Surveillance
This remains one of the most debated questions in thromboembolism management. Current evidence:
2026 Meta-Analysis (Nicoletto et al., Thrombosis Research, PMID: 41962426)
- 8 observational studies, 674 patients
- VTE recurrence: No statistically significant difference between anticoagulated and non-anticoagulated groups (RR 0.61, 95% CI 0.28-1.35)
- Bleeding: Significantly higher in anticoagulated patients (RR 3.10, 95% CI 1.39-6.88)
- All-cause mortality: No significant difference
- Conclusion: Available evidence does not support routine anticoagulation for isolated SSPE
2024 Systematic Review (Chin et al., Am Surg, PMID: 38058129)
- Supports clinical surveillance as a valid strategy in selected low-risk patients
Guideline Recommendations (ESC/ACCP)
- Anticoagulate if: concurrent proximal DVT, poor cardiopulmonary reserve, high recurrence risk, cancer
- Surveillance (no anticoagulation) may be considered if: isolated SSPE, no proximal DVT on lower extremity ultrasound, low recurrence risk, high bleeding risk
- Must perform bilateral leg ultrasound before withholding anticoagulation
Diagnostic Algorithm for Isolated SSPE
CTPA shows isolated SSPE
↓
Bilateral lower extremity venous ultrasound
↓
DVT present? → YES → Anticoagulate
↓ NO
Assess risk factors for VTE recurrence
↓
High risk (cancer, thrombophilia, recent surgery)?
→ YES → Anticoagulate
→ NO → Consider clinical surveillance
↓
Consider V/Q scintigraphy to confirm/refute CTPA finding
(especially if isolated single-vessel SSPE, uncertain quality)
Key Teaching Points
- SSPE = thrombus in 4th-order (subsegmental) pulmonary arteries, smallest branches visible on CTPA
- Filling defect is the hallmark - "polo mint" sign on axial view, "railway sign" on longitudinal view
- False positives are common - always review in all planes; inter-observer agreement is lower for SSPE than proximal PE
- Isolated SSPE without DVT may not require anticoagulation in low-risk patients - a critical management distinction from proximal PE
- V/Q scintigraphy can confirm questionable CTPA findings and guide management decisions
- The incidence of CT-detected SSPE has risen with improved scanner resolution, raising questions about overdiagnosis
Sources: Murray & Nadel's Textbook of Respiratory Medicine (eFigure 20.54); Fuster & Hurst's The Heart, 15th ed.; Nicoletto et al., Thrombosis Research 2026 [PMID: 41962426]; Baumgartner et al., Hämostaseologie 2024 [PMID: 37871632]; Radiopaedia PE article
Segmental
Finding Sources
Searching the Web
segmental pulmonary embolism CTPA CT imaging filling defect radiology images
Reading File
Loading Image
Loading Image
Finding Sources
Loading Image
Finding Sources
Searching the Web
segmental pulmonary artery PE polo mint railway sign CTPA axial coronal images 2023 2024
Finding Sources
Loading Image
Reading Web Page
https://radiologykey.com/imaging-of-acute-pulmonary-embolism
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Loading Image
Finding Sources
Loading Image
Reading File
I now have everything needed. Here is the full answer on segmental pulmonary embolism:
Segmental Pulmonary Embolism
Definition and Anatomy
Segmental PE refers to thrombus in the segmental (third-order) pulmonary arteries - branches arising from lobar arteries that supply individual bronchopulmonary segments. These vessels are:
- Diameter: approximately 3-6 mm on CTPA
- Clearly visible on standard-quality CTPA without special technical requirements
- The target level for "adequately opacified vessels" on diagnostic quality assessment
The pulmonary artery hierarchy:
- Main PA → Right/Left PA → Lobar arteries → Segmental arteries (3rd order) → Subsegmental arteries (4th order)
There are 18 segmental arteries total (10 right, 8 left), each named for the bronchopulmonary segment it supplies (e.g., right lower lobe posterior basal segmental artery, right upper lobe anterior segmental artery).
CT Imaging (CTPA)
Segmental PE is reliably detected by modern CTPA and has high inter-observer agreement compared to subsegmental disease. Segmental-level emboli are seen in the lobar/segmental branches and are the "working level" of confident PE diagnosis.
Image 1: Axial CTPA - Segmental + Lobar PE (Tintinalli's Emergency Medicine, Figure 56-3)

Caption (Tintinalli's Emergency Medicine): Axial CTPA image demonstrating filling defects consistent with acute pulmonary embolism. Two white arrowheads outline a circular filling defect in the right middle lobar pulmonary artery (central, ring of contrast = "polo mint" sign). The long white arrow (left lung) points to a filling defect in a segmental artery - the posterior medial segmental artery of the left lower lobe.
Image 2: Coronal CTPA - Normal vs. PE with Filling Defects (Labelled)

Left panel: Normal CTPA - no filling defects, homogeneous contrast enhancement of all pulmonary artery branches including segmental level.
Right panel: PE - multiple filling defects (red arrows) in the right pulmonary artery and its lobar/segmental branches, demonstrating how thrombus appears as low-attenuation material disrupting the bright contrast column.
Direct CT Signs of Segmental PE
1. "Polo Mint" Sign (= "Doughnut Sign")
- Seen when imaging orthogonal (perpendicular) to the vessel long axis
- Central low-attenuation filling defect (thrombus) surrounded by a peripheral ring of bright contrast
- The affected vessel is typically expanded/dilated
- The filling defect edge forms an acute angle with the vessel wall (differentiates acute from chronic PE)
- Classic at the segmental level where vessel diameter is ideal for this appearance
2. "Railway Sign" (= "Tram-Track Sign")
- Seen when imaging parallel to the vessel long axis
- Central linear filling defect flanked by two parallel stripes of contrast
- Indicates non-occlusive thrombus
- Best demonstrated on coronal or sagittal reformats along the segmental artery axis
- Example: right lower lobe superior segmental artery running in the plane of imaging
3. Occlusive / "Cut-Off" Sign
- Complete absence of contrast within the segmental vessel
- The vessel itself may appear dilated (expanded) compared to the contralateral equivalent
- Abrupt termination of the contrast column
4. Eccentric Mural Defect
- Thrombus adherent to one wall
- Low-density material forming acute angle with vessel wall
- Partial opacification of remaining lumen
5. "Vessel Expansion" Sign
- Affected segmental artery is visibly wider than the paired/contralateral vessel
- Caused by distension from thrombus
Anatomy: Which Segmental Arteries Are Involved?
Lower lobe segmental arteries account for the majority (~80-90%) of segmental PE due to:
- Greater blood flow volume
- Gravitational preferential flow
- Larger caliber
| Lobe | Segmental arteries |
|---|---|
| RUL | Apical, Anterior, Posterior |
| RML | Medial, Lateral |
| RLL | Superior, Medial basal, Anterior basal, Lateral basal, Posterior basal (most common) |
| LUL | Apico-posterior, Anterior, Superior lingular, Inferior lingular |
| LLL | Superior, Antero-medial basal, Lateral basal, Posterior basal |
The right lower lobe posterior basal segmental artery is among the most commonly involved.
Secondary (Indirect) Signs on CTPA at Segmental Level
When segmental PE causes downstream infarction or perfusion change:
| Secondary Sign | Appearance | Significance |
|---|---|---|
| Hampton's Hump | Wedge-shaped peripheral consolidation, pleural-based, apex toward hilum | Pulmonary infarct (~30% of PE cases) |
| Reverse Halo / Atoll Sign | Round GGO center surrounded by rim of consolidation | Organising infarct |
| Westermark Sign | Oligaemia / decreased vascular markings distal to occlusion | Reduced perfusion |
| Pleural effusion | Ipsilateral small effusion (usually exudate) | Common, ~40% of PE |
| Raised hemidiaphragm | Loss of lung volume from infarction/atelectasis | Non-specific |
Segmental vs. Subsegmental PE: Key Differences
| Feature | Segmental PE | Subsegmental PE |
|---|---|---|
| Vessel order | 3rd order | 4th order |
| Vessel diameter | 3-6 mm | <3 mm |
| Inter-observer agreement | High | Low (25-60%) |
| Confidence of diagnosis | High | Moderate |
| Always anticoagulate? | Yes | Debated |
| Clinical significance | Definite treatment threshold | May not need anticoagulation |
| Artifact risk | Low | High |
Management: Segmental PE Always Requires Anticoagulation
Per Tintinalli's Emergency Medicine: "Anticoagulation should be started for all patients with a segmental or larger filling defect consistent with PE seen on CT scan."
This is unambiguous - unlike subsegmental PE where surveillance may be considered, segmental PE:
- Carries significant clot burden
- Has well-established VTE recurrence risk
- Falls clearly above the threshold for anticoagulation in all major guidelines (ESC, ACCP/CHEST, AHA)
Standard anticoagulation options:
- DOAC (rivaroxaban, apixaban - preferred first-line in most patients)
- LMWH bridge to warfarin
- LMWH alone (cancer-associated)
Duration: typically 3 months minimum; extended if unprovoked.
Pitfalls Specific to Segmental Arteries
| Pitfall | Cause | How to Avoid |
|---|---|---|
| Hilar lymph nodes | External compression mimicking filling defect | Review in all planes; node is extramural |
| Cardiac motion artifact | Blurring of medial segmental vessels near the heart | Lung window confirms vessel integrity; repeat with ECG-gating |
| Mucus-filled bronchi | Adjacent bronchus shows wall enhancement | Trace the airway vs. artery on contiguous slices |
| Incomplete contrast mixing | Streaming artifact in segmental branches | Check ROI attenuation; value >120 HU suggests artifact |
| Partial volume (oblique vessels) | Vessel running obliquely through slice gives apparent defect | Review orthogonal MPR views - true PE persists |
Key Teaching Summary
- Segmental PE = 3rd-order pulmonary arteries, diameter 3-6 mm - reliably seen on CTPA
- Direct signs: polo mint sign (axial), railway sign (longitudinal), cut-off, eccentric mural defect, vessel expansion
- Lower lobes dominate (80-90%), especially posterior basal segments bilaterally
- Always anticoagulate segmental PE - no debate, unlike subsegmental
- Secondary signs (Hampton's hump, pleural effusion, oligaemia) support the diagnosis and indicate infarction
- Inter-observer agreement is high at segmental level - confident, actionable diagnosis
Sources: Tintinalli's Emergency Medicine (Figure 56-3, p. 436, 438); Murray & Nadel's Textbook of Respiratory Medicine; Imaging of Acute PE - Radiology Key; PMC: Imaging of Acute PE Update
This is a shared conversation. Sign in to Orris to start your own chat.