Explain all cns
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from authoritative textbooks. Let me compile a complete, well-structured student exam-level explanation.
The Central Nervous System (CNS) - Complete Overview
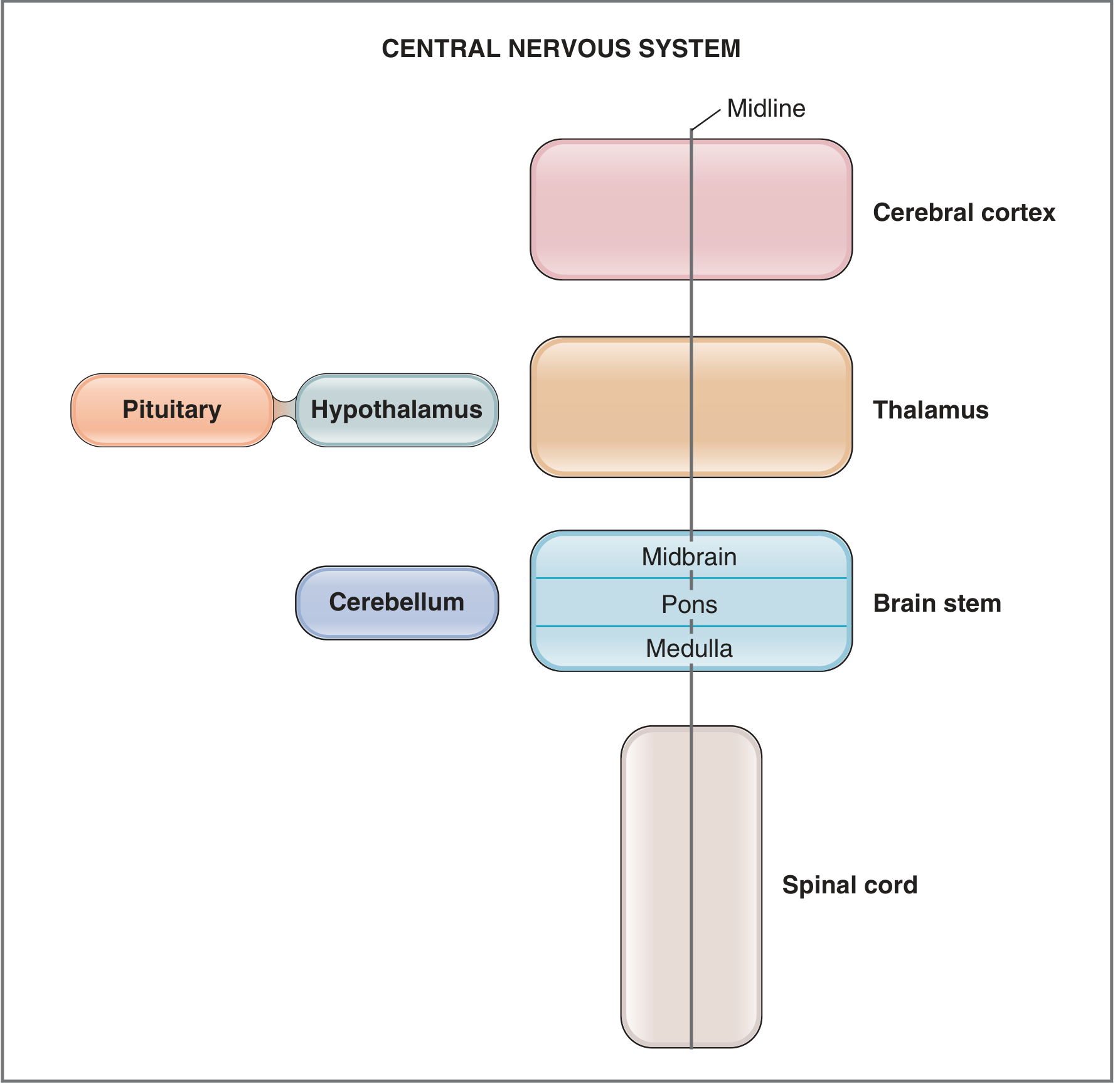
What is the CNS?
The Central Nervous System consists of the brain and the spinal cord. It is the primary control center of the body, receiving sensory input, processing information, and sending out motor commands. It is protected by:
- The skull (for the brain) and vertebral canal (for the spinal cord)
- Three layers of meninges (connective tissue coverings)
- Cerebrospinal fluid (CSF) in the subarachnoid space
Meninges (Protective Coverings)
The meninges are three layers that surround and protect both the brain and spinal cord:
| Layer | Description |
|---|---|
| Dura mater | Outermost, thickest layer |
| Arachnoid mater | Middle layer, against the inner surface of dura |
| Pia mater | Innermost, directly adherent to brain/spinal cord surface |
The subarachnoid space lies between the arachnoid and pia mater and is filled with CSF.
- Gray's Anatomy for Students, p. 48
Major Divisions of the CNS
1. BRAIN
The brain has three main parts: the cerebral hemispheres, the diencephalon, and the brainstem (plus the cerebellum).
A. Cerebral Hemispheres (Cerebrum)
The largest part of the brain, consisting of:
- Cerebral cortex - the convoluted (folded) outer surface, divided into four lobes
- Underlying white matter
- Three deep nuclei: basal ganglia, hippocampus, amygdala
The Four Lobes of the Cerebral Cortex:
| Lobe | Location | Key Functions |
|---|---|---|
| Frontal | Anterior | Voluntary movement (primary motor cortex), planning, personality, speech (Broca's area) |
| Parietal | Superior-posterior | Sensory processing (primary somatosensory cortex), spatial awareness |
| Temporal | Lateral | Hearing (primary auditory cortex), memory, language comprehension (Wernicke's area) |
| Occipital | Posterior | Vision (primary visual cortex) |
Lobes are separated by sulci (grooves). Elevated ridges are called gyri.
Cortical areas are classified as:
- Primary - directly receive/send signals (fewest synapses)
- Secondary/Tertiary - more complex processing
- Association areas - integrate diverse information (e.g., limbic association area for motivation, memory, and emotion)
Deep Nuclei:
-
Basal ganglia (caudate nucleus + putamen + globus pallidus): receive input from all cortical lobes, project via thalamus to frontal cortex to help regulate movement
-
Hippocampus: part of the limbic system; involved in memory formation
-
Amygdala: part of the limbic system; involved in emotion; communicates with the autonomic nervous system via the hypothalamus
-
Costanzo Physiology 7th Ed., p. 77
B. Diencephalon ("Between Brain")
Located between the cerebral hemispheres and brainstem. Consists of:
Thalamus
- Processes almost all sensory information going to the cerebral cortex
- Also processes almost all motor information coming from the cerebral cortex to the brainstem and spinal cord
- Acts as a major relay station for the brain
Hypothalamus
-
Lies ventral to the thalamus
-
Regulates: body temperature, food intake, water balance
-
Controls pituitary hormone secretion (releasing and inhibiting hormones via the hypophysial portal blood)
-
Contains cell bodies of neurons that produce ADH (antidiuretic hormone) and oxytocin (secreted by the posterior pituitary)
-
Costanzo Physiology 7th Ed., pp. 77-78
C. Brainstem
The brainstem = Midbrain + Pons + Medulla oblongata. It is continuous with the spinal cord inferiorly. 10 of the 12 cranial nerves (CN III-XII) arise from the brainstem.
| Part | Position | Key Functions |
|---|---|---|
| Midbrain | Rostral (uppermost) | Eye movement control; relay nuclei for auditory and visual systems |
| Pons | Middle | Balance, posture maintenance; regulation of breathing; relays signals from cerebral hemispheres to cerebellum |
| Medulla oblongata | Caudal (lowermost), closest to spinal cord | Autonomic centers for breathing and blood pressure; coordinates swallowing, coughing, and vomiting reflexes |
- Costanzo Physiology 7th Ed., p. 77
D. Cerebellum
- Attached to the brainstem; lies dorsal to the pons and medulla
- Foliated ("leafy") structure
- Functions:
- Coordination of movement
- Planning and execution of movement
- Maintenance of posture
- Coordination of head and eye movements
- Positioned strategically between the cerebral cortex and spinal cord - integrates:
- Sensory position information from the spinal cord
- Motor information from the cerebral cortex
- Balance information from the vestibular organs of the inner ear
2. SPINAL CORD
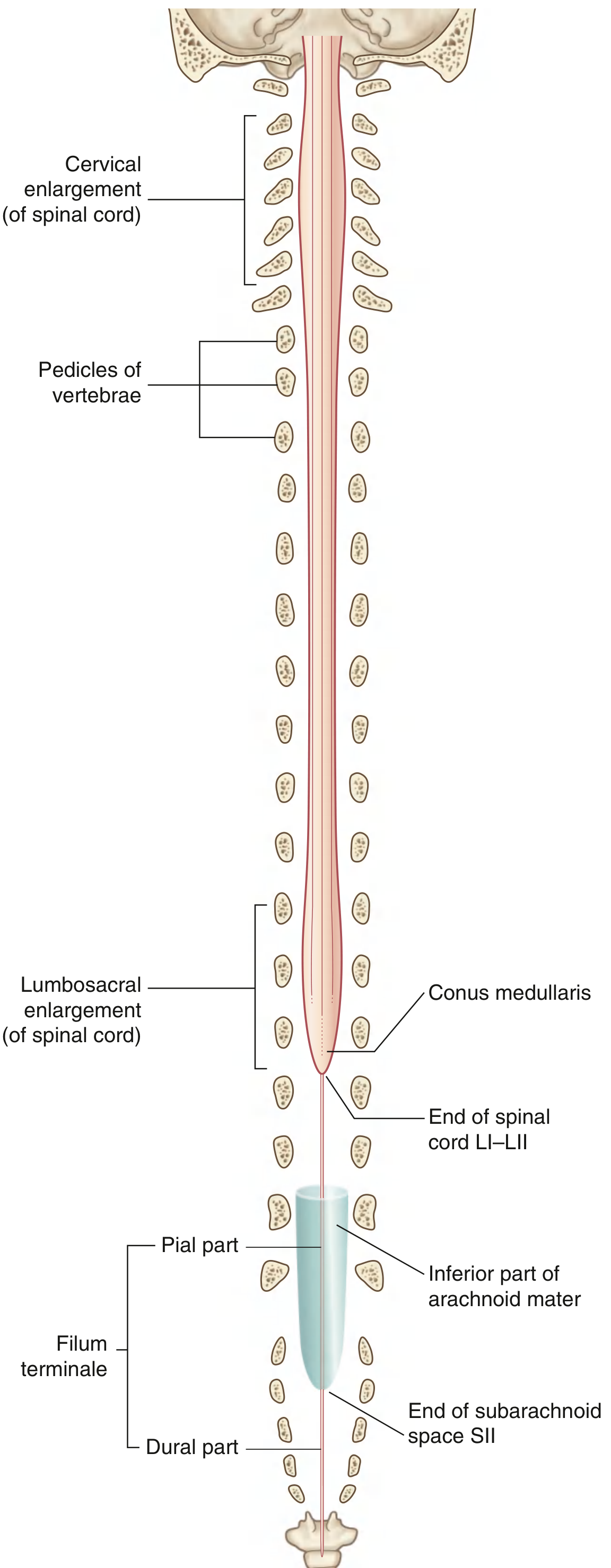
- Extends from the foramen magnum to approximately the level of disc L1-L2 in adults
- The distal end is the conus medullaris (cone-shaped); below it, a fine filament called the filum terminale continues inferiorly
- Has 31 pairs of spinal nerves (each with sensory/afferent and motor/efferent components)
Two Enlargements:
| Enlargement | Vertebral Level | Supplies |
|---|---|---|
| Cervical enlargement | C5-T1 | Upper limbs |
| Lumbosacral enlargement | L1-S3 | Lower limbs |
Internal Organization:
- Gray matter (central, H-shaped in cross section): rich in nerve cell bodies
- White matter (surrounding the gray matter): rich in nerve fibers/tracts that ascend and descend
Key Pathways:
- Ascending pathways: carry sensory information from periphery to higher CNS levels
- Descending pathways: carry motor information from higher CNS to the motor nerves of the periphery
Sensory nerves carry information from the skin, joints, muscles, and visceral organs via dorsal root ganglia. Motor nerves include:
-
Somatic motor - innervate skeletal muscle
-
Autonomic motor - innervate cardiac muscle, smooth muscle, glands
-
Costanzo Physiology 7th Ed., p. 76; Gray's Anatomy for Students, pp. 119-120
Cells of the CNS
Neurons
The functional unit of the nervous system. Structure:
| Component | Function |
|---|---|
| Cell body (soma) | Contains nucleus, ER, Golgi; synthesizes proteins |
| Dendrites | Receive incoming signals; contain receptors for neurotransmitters |
| Axon | Arises from the axon hillock; carries action potentials (up to 1 m long); may be myelinated |
| Presynaptic terminals | Release neurotransmitters into the synapse when action potential arrives |
Myelinated axons conduct faster; breaks in myelin occur at the nodes of Ranvier (saltatory conduction).
Glial Cells (Support Cells)
Glial cells outnumber neurons and occupy over half of the brain's volume.
| Cell Type | Function |
|---|---|
| Astrocytes | Supply metabolic fuel (lactic acid) to neurons; synthesize neurotransmitters; modulate cerebral blood flow; maintain extracellular K⁺ concentration |
| Oligodendrocytes | Produce myelin in the CNS |
| Schwann cells | Produce myelin in the PNS (peripheral nervous system) |
| Microglial cells | Proliferate after neuronal injury; act as scavengers to remove cellular debris |
- Costanzo Physiology 7th Ed., pp. 78-79
Functional Divisions of the CNS
The nervous system is divided functionally into:
| Division | What it innervates | Primary role |
|---|---|---|
| Somatic | Skin and skeletal muscle | Receive and respond to the external environment |
| Visceral (Autonomic) | Smooth muscle, cardiac muscle, glands, organs | Detect and respond to the internal environment |
- Gray's Anatomy for Students, p. 48
Quick Summary Table
| Structure | Location | Key Function |
|---|---|---|
| Cerebral cortex | Outermost brain | Perception, cognition, voluntary movement, memory |
| Basal ganglia | Deep cerebral nuclei | Regulate movement |
| Hippocampus | Medial temporal lobe | Memory |
| Amygdala | Medial temporal lobe | Emotion |
| Thalamus | Diencephalon | Sensory/motor relay station |
| Hypothalamus | Diencephalon | Temperature, hunger, water balance, endocrine control |
| Midbrain | Brainstem | Eye movements, auditory/visual relay |
| Pons | Brainstem | Balance, posture, breathing relay |
| Medulla | Brainstem | Breathing, BP, reflexes (swallowing, cough, vomit) |
| Cerebellum | Posterior fossa | Movement coordination, posture |
| Spinal cord | Vertebral canal | Sensory/motor relay; 31 spinal nerves |
Sources: Costanzo Physiology 7th Edition, pp. 76-79 | Gray's Anatomy for Students, pp. 48, 119-120
Everything related to Babinski sign in detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching the Web
Babinski sign variants Chaddock Oppenheim Gordon Bing surrogate signs UMN
I now have comprehensive, authoritative content from multiple sources. Let me compile the complete, detailed explanation.
The Babinski Sign - Complete Guide
1. History & Eponym
The Babinski sign was first described by Joseph Babinski (1857-1932), a French neurologist of Polish origin, in 1896 (the "great toe sign") and again in 1903 (the "toe abduction" or "fan sign"). It remains one of the most important and reliable clinical signs in neurology.
- Adams and Victor's Principles of Neurology, 12th Ed., p. 73
2. How to Elicit the Sign
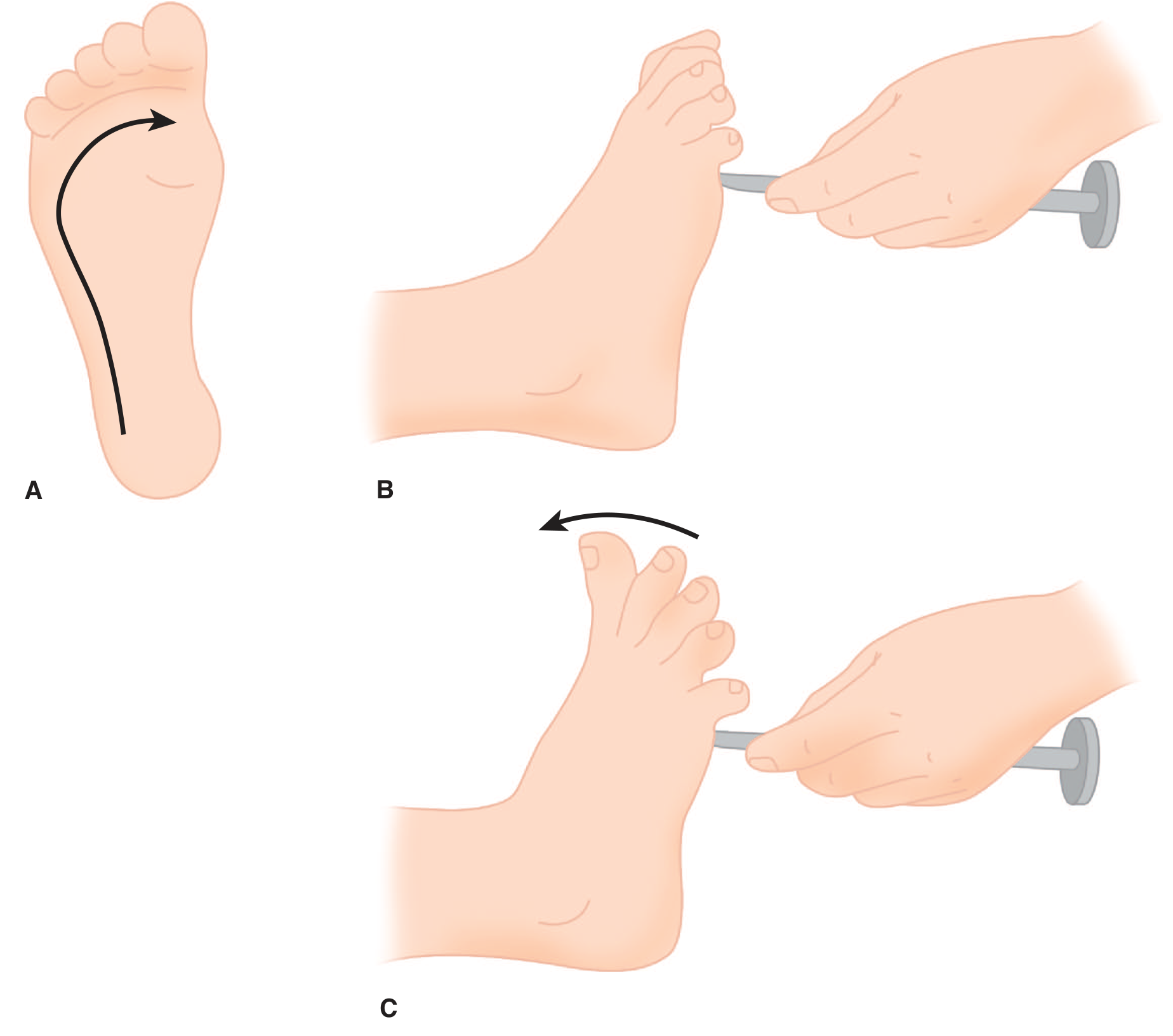
Technique:
- Use a blunt instrument (e.g., tongue depressor, key, or the handle of a reflex hammer)
- Apply a firm but not painful stimulus to the lateral plantar surface of the foot
- Start from the lateral heel, sweep forward toward the small toe, then arc medially toward the big toe
- Observe the movement of the toes
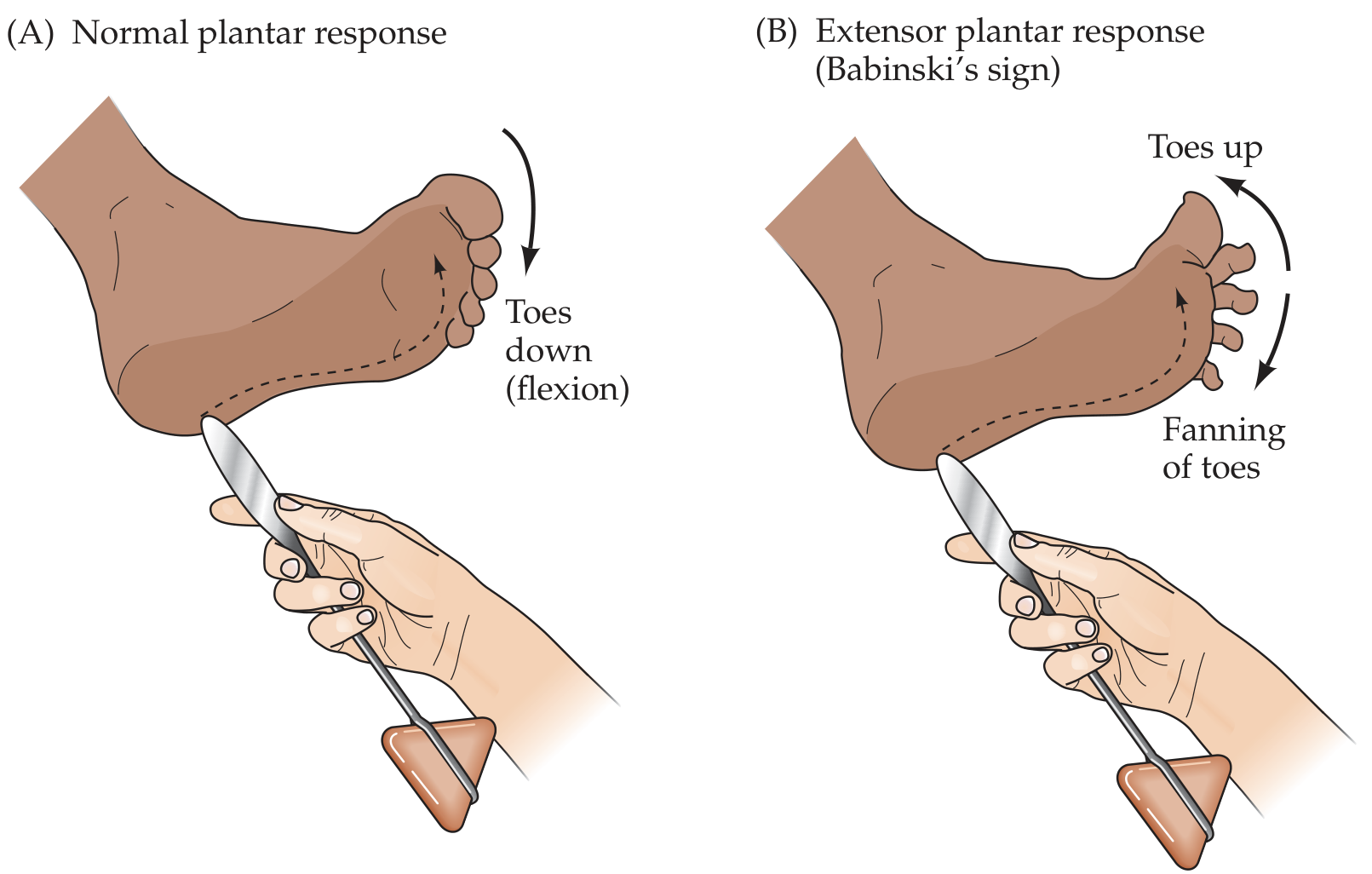
3. Responses - Normal vs Abnormal
| Response | Finding | Interpretation |
|---|---|---|
| Normal (adults) | Toes curl downward (plantar flexion) | Normal corticospinal tract |
| Positive Babinski | Big toe extends upward (dorsiflexion) + fanning of other toes | UMN lesion |
| "Silent" toes | Toes move neither up nor down | If one side goes down and other is silent, the silent side is abnormal |
| Normal (infants <~1-2 years) | Upgoing toe | Physiological - descending tracts not yet myelinated |
"The presence of Babinski's sign in an adult is always abnormal."
- Neuroanatomy through Clinical Cases, 3rd Ed., p. [reflex section]
4. Physiological Basis (Mechanism)
The Babinski sign is a component of the flexion withdrawal reflex (also called the "triple flexion response" or nocifensive reflex). In the intact adult:
- The corticospinal (pyramidal) tract exerts tonic inhibitory control over the flexion withdrawal reflex
- Plantar stimulation normally produces plantar flexion (a simple spinal reflex suppressed by descending inhibition)
When the corticospinal tract is damaged:
- This inhibitory control is lost ("release phenomenon")
- The primitive flexor/withdrawal reflex is disinhibited
- Plantar stimulation triggers the full withdrawal response: hip flexion + knee flexion + ankle dorsiflexion - and as part of this, the big toe extends (what appears as "upgoing") while other toes fan out
- In physiologic terms, toe extension IS part of the flexor withdrawal response - it's not a true extensor response
Key quote: "Clinical and electrophysiologic observations indicate that the extension movement of the great toe is a component of a larger synergistic flexion or shortening reflex of the leg - that is, toe extension when viewed from a physiologic perspective is a protective (nocifensive, or defensive) response."
- Adams and Victor's Principles of Neurology, 12th Ed., p. 74
In normal infants: The Babinski sign is present because the corticospinal tracts are not yet fully myelinated. It disappears as myelination completes (around 1-2 years of age).
5. What It Indicates - UMN Lesion
A positive Babinski sign is the most reliable indicator of an upper motor neuron (UMN) lesion affecting the corticospinal tract at any level.
Classic UMN Syndrome Features:
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Muscles affected | Groups of muscles | Individual muscles |
| Tone | Spasticity (increased) | Flaccidity (decreased) |
| Reflexes | Hyperreflexia | Hyporeflexia / areflexia |
| Plantar reflex | Babinski sign (extensor) | Normal flexor response |
| Atrophy | Slight (disuse only) | Pronounced (up to 70%) |
| Fasciculations | Absent | May be present |
| EMG | Normal nerve conduction; no denervation | Abnormal nerve conduction; fibrillations, fasciculations |
- Adams and Victor's Principles of Neurology, 12th Ed., Table 3-1, p. 75
Where Along the Corticospinal Tract?
A Babinski sign may result from a lesion anywhere along the corticospinal tract:
- Cerebral cortex (motor cortex, internal capsule)
- Brainstem (descending corticospinal fibers)
- Spinal cord (lateral corticospinal tract)
6. Common Clinical Conditions Where Babinski Is Positive
| Category | Examples |
|---|---|
| Stroke / CVA | Cortical stroke, capsular infarct, brainstem stroke |
| Spinal cord lesions | Cord compression, trauma, myelitis, MS |
| Brain/spinal tumors | Cortical or spinal mass lesions |
| Demyelinating disease | Multiple sclerosis |
| Motor neuron disease | ALS (Amyotrophic Lateral Sclerosis) - has BOTH UMN and LMN signs |
| Cervical spondylotic myelopathy | Cervical cord compression |
| Metabolic encephalopathy (transient) | Hypoglycemia, postictal state |
| Head injury/TBI | |
| Severe systemic illness | Deep coma, severe infections |
"Hyperreflexia, clonus, or a Babinski sign (positive plantar reflex) suggests upper motor neuron pathology, such as cord impingement."
- Rosen's Emergency Medicine
Important caveat (from Tintinalli's Emergency Medicine): In acute stroke or acute spinal cord injury, reflexes (including Babinski) may take hours to days to become hyperactive due to "spinal shock." The absence of Babinski does NOT exclude acute UMN pathology early on.
7. Associated UMN Signs (Context of Babinski)
When a Babinski sign is present, look for these co-existing UMN signs:
- Spasticity - velocity-dependent increased tone ("clasp-knife" phenomenon)
- Hyperreflexia - exaggerated deep tendon reflexes
- Clonus - rhythmic oscillation (5-7 Hz) at ankle or patella with sustained stretch
- Loss of abdominal reflexes - normally abolished by UMN lesions
- Hemiplegia pattern - arm flexed/pronated, leg extended/adducted
The degree of spasticity and weakness do not always correlate - severe weakness can have mild spasticity and vice versa.
8. Variants of Babinski Sign (Surrogate Signs)
Over the years, more than 30 surrogate responses have been described using different stimulation sites. All have the same clinical significance as the classic Babinski sign (indicating UMN lesion). The most important ones:
| Sign | Stimulus | Response |
|---|---|---|
| Babinski (classic) | Stroke lateral sole heel to toe | Upgoing great toe + fanning |
| Chaddock's sign | Stroke skin around/below lateral malleolus in a circle | Upgoing great toe |
| Oppenheim's sign | Compress/stroke anterior tibia with thumb and index finger (downward) | Upgoing great toe |
| Gordon's sign | Deep pressure/squeeze the calf muscle | Upgoing great toe |
| Bing's sign | Prick the dorsum of the foot or 1st toe with a pin | Upgoing great toe |
| Schaeffer's sign | Deep pressure on the Achilles tendon | Upgoing great toe |
| Gonda's sign | Forceful stretching/snapping 2nd or 4th toe downward | Upgoing great toe |
| Stransky's sign | Vigorously abduct then snap the 5th (little) toe | Upgoing great toe |
| Strümpell's sign | Patient attempts to flex knee against resistance | Upgoing great toe |
| Moniz's sign | Ankle is forcibly and passively plantar flexed | Upgoing great toe |
| Rossolimo's sign | Tap ball of foot / flick distal phalanges of toes | Upgoing great toe |
"Several dozen surrogate responses (with numerous eponyms) have been described...all have the same significance as the Babinski response."
- Adams and Victor's Principles of Neurology, 12th Ed., p. 74
Why are variants useful? If the plantar surface is hypersensitive, painful, or callused, eliciting the classic Babinski may be difficult. Also, when toe extensors are severely weak, Babinski may not be elicitable at all - variants that use proximal stimulation may then be helpful.
9. Grading / Forms of Response
| Form | Description |
|---|---|
| Minimal | Tensor fascia lata and hamstrings contract only; toe movement subtle |
| Classic | Clear upgoing big toe + fanning of toes |
| Exaggerated | Full triple flexion (hip + knee flexion + ankle dorsiflexion) - seen in severe cord lesions |
| Flexor spasm dominant | Seen in posterior column disease (MS, subacute combined degeneration) |
| Extensor spasm dominant | Seen in isolated corticospinal lesions with intact posterior columns |
| Pseudo-Babinski | Seen in sensitive individuals with plantar hyperaesthesia or choreoathetosis; not a true sign |
10. Clinical Pearls for Exams
- Positive Babinski in an adult = always abnormal = UMN/corticospinal tract lesion until proven otherwise
- Positive Babinski in an infant < 1-2 years = normal (immature myelination)
- The response is really a disinhibited flexor withdrawal reflex - "toe extension" is physiologically a flexion movement
- The Babinski sign may be absent early in acute UMN lesions (spinal shock) - do not use its absence to exclude cord injury acutely
- It cannot be elicited if there is severe weakness of the toe extensors (LMN lesion to the foot)
- In ALS, you see both Babinski (UMN) and muscle wasting/fasciculations (LMN) - this combination is pathognomonic
- All Babinski equivalents (Chaddock, Oppenheim, Gordon, etc.) carry the same clinical meaning
- Babinski sign + spasticity + hyperreflexia + clonus = complete UMN syndrome
- The abdominal reflexes are lost in UMN lesions (opposite to Babinski, which is gained)
Sources:
- Adams and Victor's Principles of Neurology, 12th Ed., pp. 73-75 (dedicated section)
- Neuroanatomy through Clinical Cases, 3rd Ed. (plantar response testing)
- Neuroscience: Exploring the Brain, 5th Ed. (UMN vs LMN, Babinski mechanism)
- Tintinalli's Emergency Medicine (clinical context, spinal cord emergencies)
- Rosen's Emergency Medicine (UMN signs)
Whats important in babinski sign in first year physiology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have all the content I need from physiology textbooks. Let me compile a focused, exam-oriented answer specifically for first-year physiology students.
Babinski Sign - What's Important for First Year Physiology (MBBS)
Here's everything you need to know, structured exactly how it appears in exams - from Costanzo, Ganong's, and standard physiology curricula.
1. Definition (1 liner - must know)
Babinski sign = dorsiflexion (upward extension) of the great toe + fanning of the other toes when the lateral sole of the foot is stroked from heel to toe.
2. How to Elicit (Technique)
- Use a blunt object (key, tongue depressor, reflex hammer handle)
- Stroke the lateral plantar surface of the foot
- Direction: heel → small toe → arc medially toward big toe
- Force: firm but not painful
3. Responses - The Core Comparison (Most Exam-Asked)
| Response | Significance | |
|---|---|---|
| Normal adult | Toes curl DOWN (plantar flexion) | Normal corticospinal function |
| Positive Babinski | Big toe goes UP (dorsiflexion) + other toes fan out | UMN lesion |
| Normal infant (< ~1.5 yrs) | Big toe goes UP (same as Babinski) | Physiological - immature corticospinal tracts |
4. Why Is It Positive in UMN Lesions? (The Physiology - Most Important)
This is the core physiology concept that examiners love to ask.
The Normal Situation:
- The corticospinal (pyramidal) tract descends from the motor cortex → through brainstem → to anterior horn cells of the spinal cord
- It exerts tonic inhibitory control over spinal reflex circuits
- Plantar stimulation normally produces a simple plantar flexion reflex suppressed by this descending inhibition
When the Corticospinal Tract Is Damaged:
- The inhibitory control is removed (disinhibition / "release phenomenon")
- The primitive flexor withdrawal reflex is released
- Plantar stimulation triggers the full withdrawal (flexor) reflex:
- Hip flexes → Knee flexes → Ankle dorsiflexes → Big toe extends upward + toes fan
- What looks like "toe extension" is actually part of the protective flexion withdrawal response
"Damage to upper motor neurons initially causes muscles to become weak and flaccid but eventually leads to spasticity, hypertonia, hyperactive stretch reflexes, and abnormal plantar extensor reflex (positive Babinski sign)."
- Ganong's Review of Medical Physiology, 26th Ed.
Key Physiology Concept to Write in Exams:
The Babinski sign = release of the flexor withdrawal reflex from corticospinal inhibition.
5. Why Is It Normal in Infants? (Another Favourite Exam Point)
- At birth, the corticospinal tracts are not fully myelinated
- Descending inhibitory control over spinal reflexes has not developed
- So the flexor withdrawal reflex is uninhibited → toe goes up (same as Babinski)
- As myelination completes (around 12-18 months), the response converts to normal plantar flexion
- Persistence after 2 years = abnormal (indicates UMN lesion)
6. UMN vs LMN - The Classic Table (Always in First Year Physiology Exams)
This comparison is a guaranteed question - Babinski sign sits firmly in the UMN column:
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Weakness | Yes | Yes |
| Tone | Increased (Spasticity) | Decreased (Flaccidity) |
| Reflexes (DTR) | Increased (Hyperreflexia) | Decreased (Hyporeflexia/Areflexia) |
| Babinski sign | Positive (extensor plantar) | Absent - normal plantar flexion |
| Atrophy | No (only disuse) | Yes (pronounced, up to 70%) |
| Fasciculations | Absent | Present |
| Clonus | Present | Absent |
| Example | Stroke, cord compression, MS | Polio, Guillain-Barré, peripheral nerve injury |
- Neuroanatomy through Clinical Cases, 3rd Ed., Table 6.4 | Ganong's, 26th Ed.
7. The Reflex Arc Background (Physiology Context)
The flexor withdrawal reflex is the basis of Babinski sign. From Costanzo Physiology:
| Reflex | Synapses | Stimulus | Afferent Fibers |
|---|---|---|---|
| Stretch reflex (knee jerk) | 1 (monosynaptic) | Muscle stretch | Ia |
| Golgi tendon reflex | 2 | Muscle contraction | Ib |
| Flexor withdrawal reflex | Many (polysynaptic) | Pain / noxious stimulus | II, III, IV |
The Babinski sign is a modified / released flexor withdrawal reflex - the noxious plantar stimulus triggers it when descending inhibition is absent.
- Costanzo Physiology, 7th Ed., Table 3.5
8. Conditions Causing Positive Babinski (Know for Viva)
| Level of Lesion | Examples |
|---|---|
| Cortex | Stroke (upper cortex/internal capsule) |
| Brainstem | Brainstem stroke |
| Spinal cord | Cord compression, MS, trauma, myelitis |
| Both UMN + LMN | ALS (amyotrophic lateral sclerosis) |
| Physiological | Normal infants < 1.5 years |
9. High-Yield Exam Points - Quick Summary
| # | Point |
|---|---|
| 1 | Positive Babinski = UMN lesion (always abnormal in adults) |
| 2 | Response = big toe UP + fanning of other toes |
| 3 | Normal adult response = toes DOWN (plantar flexion) |
| 4 | Normal in infants < 1.5-2 years (unmyelinated corticospinal tracts) |
| 5 | Mechanism = release of flexor withdrawal reflex from corticospinal inhibition |
| 6 | The "extensor" toe movement is physiologically a flexor withdrawal response |
| 7 | Associated UMN signs: spasticity + hyperreflexia + clonus + loss of abdominal reflexes |
| 8 | Associated LMN signs (contrast): flaccidity + hyporeflexia + atrophy + fasciculations |
| 9 | Cannot be elicited if toe extensors are severely weak (LMN lesion to foot) |
| 10 | In ALS: both Babinski (UMN) AND fasciculations/wasting (LMN) are present |
10. Likely Exam Questions on Babinski Sign
Short answer / SAQ:
- "What is Babinski sign? How is it elicited? What is its significance?"
- "Differentiate UMN and LMN lesions."
- "Why is Babinski sign positive in infants?"
- "Explain the mechanism of Babinski sign."
Viva questions:
- "What is the normal plantar response?"
- "Why does the toe go up in UMN lesion?"
- "At what age does Babinski disappear?"
- "Name two conditions causing positive Babinski."
- "What is the reflex arc involved in Babinski sign?"
Sources: Costanzo Physiology 7th Ed. (spinal reflexes, Table 3.5) | Ganong's Review of Medical Physiology 26th Ed. (UMN vs LMN, p. ~corticospinal section) | Neuroanatomy through Clinical Cases 3rd Ed. (clinical correlation)
This is a shared conversation. Sign in to Orris to start your own chat.