Take me through radiology introduction and others kmtc clinical medicine
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have a thorough set of content from Grainger & Allison's Diagnostic Radiology. Here is a comprehensive introduction to radiology for KMTC Clinical Medicine students:
Introduction to Radiology — KMTC Clinical Medicine
Source: Grainger & Allison's Diagnostic Radiology, a Textbook of Medical Imaging
What is Radiology?
Radiology (medical imaging) is the branch of medicine that uses various forms of energy — X-rays, sound waves, magnetic fields, and radioactive tracers — to produce images of the inside of the body for diagnosis and treatment guidance. The main modalities you need to know are:
- Plain Radiography (X-ray)
- Computed Tomography (CT)
- Ultrasound (US)
- Magnetic Resonance Imaging (MRI)
- Radionuclide Imaging / Nuclear Medicine (PET, V/Q scan)
1. Plain Radiography (X-ray / Chest X-ray)
Principle
X-ray photons are passed through the body and captured by a detector. Denser structures (bone, fluid) absorb more X-rays and appear white (radiopaque); less dense structures (air, fat) absorb fewer X-rays and appear dark (radiolucent).
Equipment — Digital vs Film
Traditional film-screen radiography has largely been replaced by two digital systems:
- Computed Radiography (CR): Uses a photostimulable phosphor plate. Still found in some departments.
- Direct Radiography (DR): Flat-panel detectors convert X-ray photons directly into electrical signals, giving superior image quality. Both are integrated into PACS (Picture Archiving and Communication Systems), enabling easy digital storage, retrieval, and sharing.
Projections
- PA (Posteroanterior): Standard erect view — patient faces the detector, X-ray beam enters from behind. Best quality.
- AP (Anteroposterior): Beam enters from front. Used for portable/bedside radiography in very ill patients — the heart appears magnified.
- Lateral: Side view — used to localize lesions.
- Decubitus: Patient lying on side; useful to detect free pleural fluid (it layers out).
Limitations of portable AP films (Box 1.1): Magnification of the heart, rotation artefacts, lower image quality, inability to perform a full inspiratory effort — all must be factored in when interpreting bedside films.
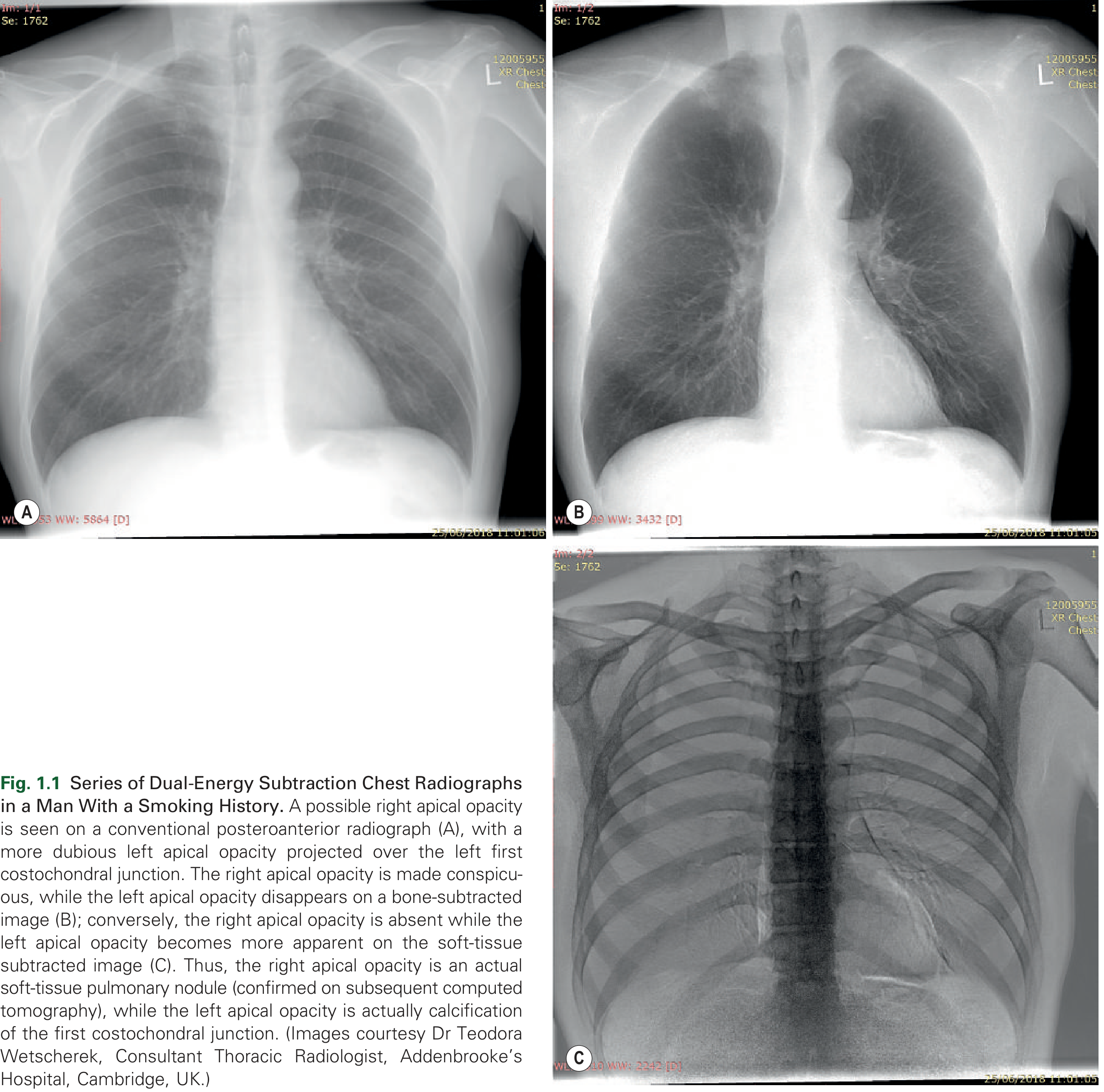
Novel Radiographic Techniques
- Dual-energy subtraction radiography: Two exposures at different kV are taken almost simultaneously. One image shows only soft tissue (bone subtracted), the other shows only bone (soft tissue subtracted). This helps distinguish pulmonary nodules from rib/costal cartilage calcifications.
2. Computed Tomography (CT)
Principle
CT uses a rotating X-ray tube and a curved row of detectors to take multiple cross-sectional images (slices) of the body. A computer reconstructs these into detailed 2D axial images and 3D reconstructions.
Evolution: Single-Slice → Multidetector CT (MDCT)
- Spiral/helical CT (introduced early 1990s): Replaced sequential single-slice CT with volumetric data acquisition — a continuous helix of data is acquired as the table moves through the gantry.
- Multidetector CT (MDCT) (from 1998): Multiple rows of detectors (up to 320 rows today) acquire data simultaneously. Benefits:
- Single breath-hold imaging of the entire thorax/abdomen
- Reduction in motion artefacts (important in children — less sedation needed)
- Improved spatial resolution — thin slices of 0.6–1.25 mm can be reconstructed
Reconstruction Algorithms (Kernels/Filters)
- Soft-tissue/low-resolution algorithm: Reduces image noise → used for mediastinum, blood vessels, liver
- Lung/high-resolution algorithm: Enhances fine detail → used for lung parenchyma, airways, HRCT
CT Windows
The greyscale on the monitor must be adjusted — called windowing:
- Lung window: Wide window; shows air and lung parenchymal detail
- Mediastinal/soft-tissue window: Narrow window; shows soft tissues, lymph nodes, vessels
- Bone window: Very wide; optimises cortical and trabecular bone detail
CT Contrast Enhancement
- IV (intravenous) iodinated contrast is used to opacify blood vessels and enhance vascular lesions. Timing of the scan after injection is critical:
- Arterial phase (~20–25 sec) — aorta, pulmonary emboli
- Portal venous phase (~70 sec) — liver parenchyma
- Delayed phase (~3–5 min) — urinary tract, some tumour characterisation
High-Resolution CT (HRCT)
- Uses thin sections (1–1.5 mm) with a high-spatial-resolution algorithm
- Gold standard for diffuse interstitial lung disease (e.g. fibrosis, bronchiectasis)
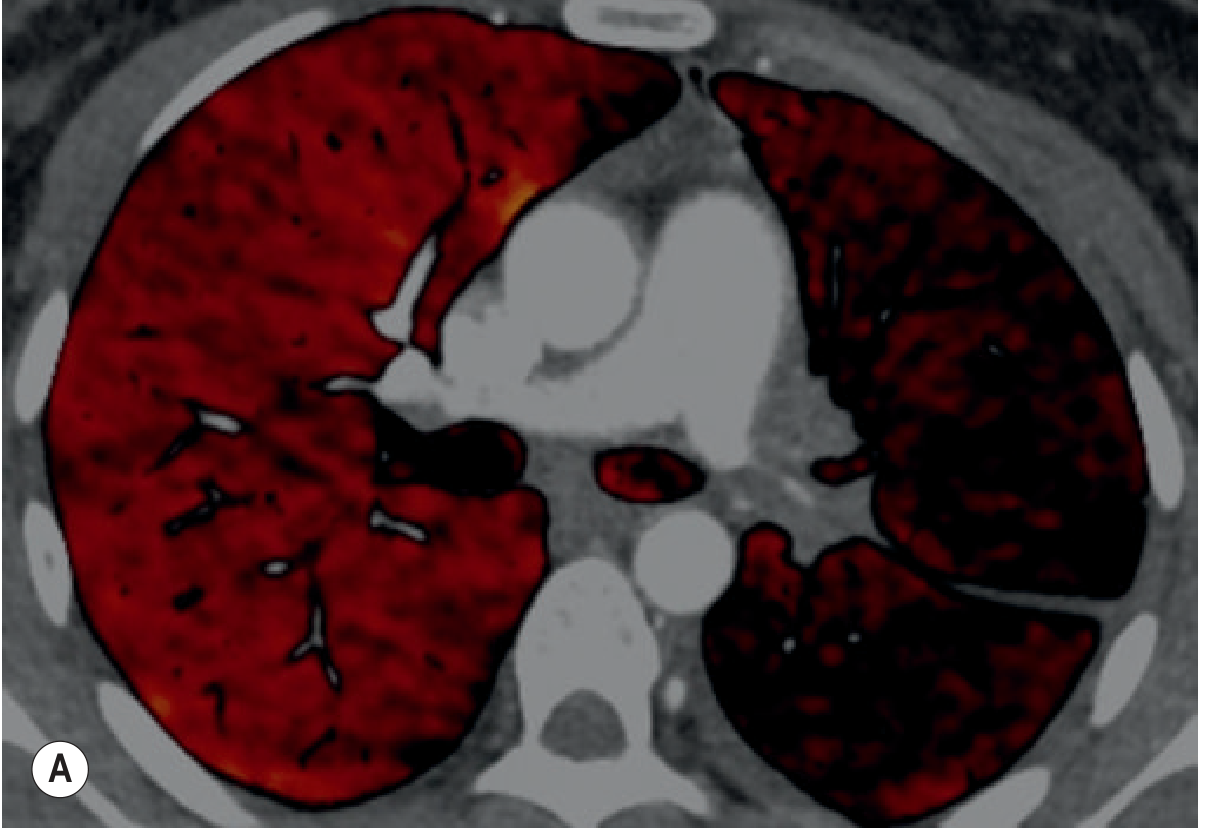
Dual-Energy CT (DECT)
Two X-ray beams at different kilovoltages allow material-specific differentiation (e.g. iodine vs calcium). This can generate:
- Virtual unenhanced images (reduces need for pre-contrast scan → lower dose)
- Pulmonary blood volume/iodine maps — shows perfusion defects in pulmonary embolism
Radiation Dose & Dose Reduction
CT carries significant radiation dose compared with plain X-ray. Key dose-reduction strategies:
- Low-dose CT protocols — lower mA settings; suitable for lung cancer screening (LDCT)
- Iterative reconstruction algorithms — mathematically reduce image noise, allowing lower doses while maintaining image quality
- Automatic tube current modulation — reduces dose in less attenuating areas (e.g. thin thorax vs shoulders)
- Dual-source CT allows low-kV scanning with dose compensation
3. Ultrasound (US)
Principle
Ultrasound uses high-frequency sound waves (2–18 MHz) emitted by a transducer (probe). Sound reflects back differently from tissues of varying density. No ionising radiation — safe for pregnant women, children, and repeated examinations.
Key Properties
- Real-time imaging — dynamic; can assess movement (e.g. diaphragm, cardiac valves)
- B-mode (brightness mode): Standard grey-scale 2D image
- Doppler ultrasound: Detects blood flow direction and velocity — used in vascular studies, echocardiography
Advantages
- No radiation
- Portable — can be performed bedside, in ICU, in theatre
- Inexpensive relative to CT/MRI
- Excellent for fluid (pleural effusion, ascites, pericardial effusion, abscess)
- Guides real-time procedures — paracentesis, thoracocentesis, biopsy, central line insertion
Limitations
- Operator-dependent
- Poor penetration through bone and air (lungs, bowel gas)
- Limited field of view in obese patients
Endoscopic Ultrasound (EUS) and Endobronchial Ultrasound (EBUS)
These combine endoscopy with ultrasound probes to image and sample mediastinal lymph nodes and masses from within the oesophagus (EUS) or airways (EBUS). A combined EUS + EBUS approach has a sensitivity of 96% for mediastinal staging in lung cancer — superior to either technique alone.
4. Magnetic Resonance Imaging (MRI)
Principle
MRI uses a strong magnetic field and radiofrequency (RF) pulses to excite hydrogen protons in body water and fat. As protons return to their resting state, they emit signals that are detected and reconstructed into images. No ionising radiation.
Key Sequences
| Sequence | Bright signal | Dark signal | Main use |
|---|---|---|---|
| T1-weighted | Fat, blood (subacute), gadolinium-enhanced tissue | Water/fluid | Anatomy, post-contrast enhancement |
| T2-weighted | Water/fluid, oedema | Fat, fibrous tissue | Pathology detection; cysts appear bright |
| STIR (fat-suppressed) | Fluid/oedema (fat suppressed) | Fat | Nodal staging, bone marrow oedema |
| DWI (diffusion-weighted) | Highly cellular tissue (restricts diffusion) | Normal tissue | Tumour characterisation |
Advantages
- Excellent soft-tissue contrast — best for brain, spinal cord, musculoskeletal, pelvic organs
- No ionising radiation
- Multi-planar imaging (axial, sagittal, coronal, oblique) without moving the patient
Limitations for the Chest
- Low signal-to-noise ratio in the lungs (proton-poor air-filled parenchyma)
- Motion artefact from breathing and cardiac pulsation
- Long scan times
- Contraindicated with ferromagnetic implants (certain pacemakers, cochlear implants, metallic foreign bodies)
- Expensive, less widely available
Thoracic MRI Indications
- Mediastinal and chest wall lesion characterisation (best modality)
- Confirm cystic nature of lesions (non-serous cysts can be dense on CT but bright on T2)
- Assess diaphragmatic invasion by pleural mesothelioma
- Differentiate rebound thymic hyperplasia from malignancy (chemical shift imaging detects fat)
- STIR sequences may outperform FDG-PET in nodal staging of lung cancer
5. Radionuclide Imaging (Nuclear Medicine)
Principle
A radiotracer (a molecule labelled with a radioactive isotope) is administered to the patient. The tracer concentrates in specific organs or tissues based on its metabolic/physiological behaviour. A gamma camera detects the emitted gamma rays and produces a functional (not purely anatomical) image.
Ventilation–Perfusion (V/Q) Scintigraphy
- Perfusion scan: Technetium-99m (⁹⁹ᵐTc) macroaggregated albumin (MAA) is injected IV → lodges in pulmonary capillaries proportional to blood flow. Perfusion defects appear as areas of reduced uptake.
- Ventilation scan: Inhaled radioactive gas (⁸¹ᵐKr or ⁹⁹ᵐTc-DTPA aerosol) → images regional ventilation.
- Clinical use: Diagnosing pulmonary embolism (PE) — PE causes perfusion defects with preserved ventilation (V/Q mismatch).
Summary: A normal perfusion scan essentially excludes PE. A V/Q mismatch pattern in the right clinical setting is highly suggestive of PE.
PET-CT (Positron Emission Tomography fused with CT)
- Tracer: FDG (¹⁸F-fluorodeoxyglucose) — a glucose analogue taken up by metabolically active cells (tumours, inflammation)
- Principle: FDG undergoes positron emission → annihilation → two 511 keV gamma rays detected simultaneously at 180° → image reconstructed
- Fusion with CT: Provides simultaneous:
- Metabolic/functional information (PET)
- Anatomical localisation (CT)
- Detection of unsuspected extrathoracic metastatic disease
- Main clinical uses:
- Lung cancer staging (detecting nodal metastases, distant metastases)
- Lymphoma staging and response assessment
- Assessing unknown primary tumours
Comparing the Modalities — Quick Summary Table
| Feature | X-ray | CT | Ultrasound | MRI | Nuclear Medicine |
|---|---|---|---|---|---|
| Radiation | Low | Moderate–High | None | None | Low–Moderate |
| Speed | Very fast | Fast | Real-time | Slow | Variable |
| Bone | Good | Excellent | Poor | Good | Good (bone scan) |
| Soft tissue | Poor | Good | Moderate | Excellent | Variable |
| Fluid detection | Moderate | Excellent | Excellent | Excellent | — |
| Functional info | No | Limited (DECT) | Doppler | Yes (DWI, MR spectroscopy) | Yes |
| Cost | Lowest | Moderate | Low | Highest | Moderate |
| Portability | Yes (portable) | No | Yes | No | No |
Key Principles for Clinical Practice
- Justify every investigation — the benefit must outweigh radiation risk (ALARA principle: As Low As Reasonably Achievable)
- Plain X-ray is usually first-line for chest, bones, and abdomen
- Ultrasound is first-line for soft tissues, fluid, and pregnancy
- CT is the workhorse for emergency/trauma, chest pathology, and staging
- MRI is preferred for brain, spinal cord, musculoskeletal, and pelvic disease
- Nuclear medicine is used when functional/metabolic information is needed
Grainger & Allison's Diagnostic Radiology — a Textbook of Medical Imaging (Grainger & Allison's)
This is a shared conversation. Sign in to Orris to start your own chat.