Imaging of bone tumors detailed explanation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive material from Grainger & Allison's Diagnostic Radiology, Miller's Review of Orthopaedics, Harrison's Principles, Rockwood & Green, and Campbell's Operative Orthopaedics. I have enough to write a detailed, well-structured answer. Let me compile it now.
Imaging of Bone Tumors - Detailed Explanation
Based on Grainger & Allison's Diagnostic Radiology, Miller's Review of Orthopaedics 9th Ed., Harrison's Principles of Internal Medicine 22E, Rockwood & Green's Fractures 10th Ed., and Campbell's Operative Orthopaedics 15th Ed.
1. The Systematic Radiological Approach (Enneking's Four Questions)
When evaluating any bone lesion, plain radiographs in two planes are obtained first to establish answers to four fundamental questions:
- Location - Where is the lesion (epiphysis, metaphysis, diaphysis; intramedullary, intracortical, surface)?
- Tumor-bone interaction - How is the tumor destroying bone (Lodwick classification)?
- Bone-tumor interaction - How is the host bone responding?
- Matrix - What are the tumor cells producing (bone, cartilage, fibrous tissue)?
2. Age of the Patient
Age is one of the most important factors in differential diagnosis:
| Age Group | Common Malignant Lesions | Common Benign Lesions |
|---|---|---|
| < 5 years | Neuroblastoma mets, Wilms tumor mets, LCH | Simple bone cyst |
| < 30 years | Ewing sarcoma, Osteosarcoma | Osteochondroma, NOF, UBC, ABC, GCT |
| > 30 years | Chondrosarcoma, Lymphoma, MFH | Enchondroma |
| > 40-50 years | Metastases (most common!), Myeloma | Paget's disease |
Primary bone tumors are rare below age 5 and above age 40. Myeloma: 97% present after age 40. A single destructive lesion in a patient over 50 years always warrants ruling out metastatic disease first.
- Miller's Review of Orthopaedics 9th Edition
3. Plain Radiograph - Rate of Growth & Lodwick Classification (Tumor-Bone Interaction)
The most important radiographic feature is the lesion margin, which reflects rate of growth:
Type I - Geographic (Slow Growth / Benign or Low-Grade)
- Type IA: Well-defined lytic lesion with a sclerotic rim (e.g., nonossifying fibroma, osteoid osteoma)
- Type IB: Well-defined lytic lesion with no marginal sclerosis (e.g., unicameral bone cyst)
- Type IC: Slightly less sharp, non-sclerotic margin (e.g., giant cell tumor)
Type II - Moth-Eaten (Moderately Aggressive)
- Multiple lucent areas 2-5 mm in diameter separated by intact trabeculae
- Examples: Osteomyelitis, metastases, lymphoma
Type III - Permeative/Destructive (Most Aggressive)
-
Multiple coalescing tiny ill-defined lesions ≤1 mm in diameter
-
Wide zone of transition spanning several centimeters
-
Example: Ewing sarcoma
-
Radiographs underestimate medullary involvement; MRI is essential
-
Grainger & Allison's Diagnostic Radiology, Miller's Review of Orthopaedics 9th Edition
4. Periosteal Reaction
Periosteal reaction reflects the aggressiveness of the lesion, though no single pattern is pathognomonic:
| Pattern | Aggressiveness | Typical Lesion |
|---|---|---|
| Thick, solid | Slow growth | Grade 2 chondrosarcoma; can also be benign |
| Laminated ("onion-skin") | Subperiosteal tumor extension | Ewing sarcoma, osteomyelitis |
| Codman's triangle | Aggressive - periosteum lifted away at tumor margin | Osteosarcoma, Ewing sarcoma |
| Sunburst / hair-on-end (vertical spiculation) | Very aggressive | Classic for osteosarcoma |
Codman's triangle: The periosteum is lifted from the cortex at the limits of subperiosteal tumor spread. It indicates the distal margin of tumor extent, not a separate lesion. Seen in osteosarcoma and Ewing sarcoma.
Sunburst pattern: Radiating spicules of new bone perpendicular to the cortex - classic for osteosarcoma. Represents reactive bone laid down along vessels running perpendicular to the cortex.
- Grainger & Allison's Diagnostic Radiology, Campbell's Operative Orthopaedics 15th Ed.
5. Anatomical Location Within the Bone
Location within the bone strongly guides diagnosis:
| Location | Typical Tumors |
|---|---|
| Epiphysis | Giant cell tumor (GCT), chondroblastoma, clear cell chondrosarcoma |
| Metaphysis | Osteosarcoma, NOF, unicameral bone cyst, chondrosarcoma, osteochondroma |
| Diaphysis | Ewing sarcoma, fibrous dysplasia, lymphoma, adamantinoma |
| Vertebral body | Hemangioma, metastases, myeloma, chordoma (ends of vertebral column) |
| Epiphysis + metaphysis | Giant cell tumor (crosses physis in skeletally mature patients) |
Skeletal distribution notes:
-
Lesions distal to the elbow and knee are usually from lung or renal primaries when metastatic
-
Myeloma: spine and ribs most common
-
Chordoma: exclusively at ends of the vertebral column (sacrum/clivus)
-
Miller's Review of Orthopaedics 9th Edition
6. Matrix Characterization on Radiograph
The matrix (what the tumor cells produce) is visible on plain films:
| Matrix Type | Radiographic Appearance | Tumor |
|---|---|---|
| Osteoid (bone) | Dense "cloud-like" or "ivory" mineralization | Osteosarcoma, osteoma |
| Chondroid | Stippled, "rings and arcs," "popcorn" calcification | Enchondroma, chondrosarcoma, chondroblastoma |
| Fibrous | Lytic, "ground-glass," no matrix mineralization | NOF, fibrous dysplasia |
| No matrix | Pure lytic | Ewing sarcoma, giant cell tumor, myeloma, metastases |
7. Number of Lesions
| Age | Multiple Lesions Pattern | Diagnosis |
|---|---|---|
| > 50 years | Multiple destructive lesions | Metastatic disease, myeloma, lymphoma, Paget's |
| < 30 years | Multiple lytic oval lesions, same extremity | Vascular tumors (hemangioendothelioma) or fibrous dysplasia (Jaffe-Campanacci) |
8. Modality-by-Modality Role
Plain Radiograph (X-ray)
- First-line always - defines lesion type, location, periosteal reaction, matrix
- Two planes mandatory
- Underestimates medullary extent
Computed Tomography (CT)
- Better than X-ray for infection detection; MRI is still more sensitive
- Confirms benign appearance of enchondroma, osteochondroma, bone island (enostosis)
- Best modality for osteoid osteoma - the nidus is better visualized on CT and can be misleading on MRI
- Precisely delineates calcifications, mineralization, cortical integrity, periosteal reaction (MDCT)
- Does not show soft tissue characteristics or medullary canal extent as well as MRI
- Used when MRI is contraindicated (pacemaker, metallic foreign bodies) or unavailable
- 3D CT for preoperative planning
MRI
- Most sensitive for evaluating bone lesions
- Should encompass the entire bone when evaluating primary bone tumors (to exclude skip metastases)
- Best for soft tissue extension, neurovascular involvement, medullary canal extent
- Guides surgical planning and limb-salvage decisions
- Guides biopsy site selection
Key MRI signal patterns by tumor:
| Tumor | T1 Signal | T2 Signal | Notes |
|---|---|---|---|
| Osteosarcoma | Low-intermediate | Heterogeneous high | Mineralized areas show low signal both sequences |
| Ewing sarcoma | Low | High | Large soft tissue mass out of proportion to bone destruction |
| Lymphoma | Low | High | Massive soft tissue mass out of proportion to minimal bone destruction |
| Chordoma | Low | Very bright | Midline sacral bone destruction + soft tissue mass |
| ABC | Variable | Fluid-fluid levels | Characteristic fluid-fluid levels on T2 |
| Myeloma | Low-intermediate | Low with small edema halo | Punched-out lesions |
Bone Scan (Tc-99m)
- Whole-body - identifies occult polyostotic bone involvement
- Useful for staging and detecting skip lesions
- Cold scan in myeloma (false negative) - skeletal survey is more sensitive for myeloma
- Useful in protracted back pain / night pain (spinal tumors)
PET/CT
- Whole-body staging for metastatic disease
- Evaluates metabolic activity - useful for treatment response assessment
Whole-body MRI
-
Used in assessment of metastases from myxoid liposarcoma specifically
-
Increasingly used for myeloma staging
-
Rockwood & Green's Fractures 10th Ed., Miller's Review of Orthopaedics 9th Edition, Grainger & Allison's Diagnostic Radiology
9. Specific Tumor Imaging Signatures
Osteosarcoma
- Metaphysis of long bones (distal femur > proximal tibia > proximal humerus)
- Aggressive mixed lytic/sclerotic lesion with sunburst periosteal reaction and Codman's triangle
- Soft tissue mass with tumor bone formation
- MRI: entire bone should be imaged to identify skip metastases
- CT chest for pulmonary metastases (most common site)
Ewing Sarcoma
- Diaphysis of long bones; flat bones (pelvis, ribs, scapula)
- Onion-skin (laminated) periosteal reaction on X-ray; Codman's triangle
- Permeative bone destruction (Lodwick type III)
- MRI: massive soft tissue mass disproportionate to the degree of bone destruction - characteristic finding
- Bone scan for staging
Giant Cell Tumor (GCT)
- Epiphysis of long bones in skeletally mature patients (distal femur, proximal tibia, distal radius)
- Lodwick type IC: lytic, geographic, eccentric, subarticular, NO sclerotic margin
- No matrix mineralization
- "Soap bubble" appearance of expanded cortex
- MRI: T1 low, T2 intermediate-high signal; well-defined margins
Chordoma
- Exclusively at ends of vertebral column: sacrum (50%), clivus (35%), vertebral bodies (15%)
- Radiographs underestimate true extent
- MRI: midline bone destruction + soft tissue mass; T1 low, T2 very bright signal; sacrum often expanded with irregular mineralization
Aneurysmal Bone Cyst (ABC)
- Metaphysis of long bones; posterior elements of spine
- Eccentric lytic expansile lesion with "eggshell" cortex
- MRI hallmark: fluid-fluid levels on T2 (layering of blood products at different stages)
Enchondroma
- Small bones of hands/feet most common; also proximal humerus, femur
- Stippled or "rings and arcs" chondroid calcification
- Benign appearance confirmed on CT; no cortical destruction, no soft tissue mass
Osteochondroma
- Sessile or pedunculated bony outgrowth with cartilage cap
- Cortex and medullary canal continuous with host bone
- MRI cartilage cap thickness: > 2 cm in adults raises concern for malignant transformation to chondrosarcoma
Multiple Myeloma
- "Punched-out" lytic lesions - no host bone response (no sclerotic margin, no periosteal reaction)
- "Ballooned" appearance with expansion in advanced disease
- Spine and ribs most common
- Whole-body low-dose CT or PET/CT now preferred over skeletal survey
Lymphoma of Bone
- Minimal bone destruction on plain film despite large soft tissue mass
- MRI T2: massive soft tissue mass disproportionate to the minimal cortical destruction - characteristic
- Older patients (>30 years); CD45+, CD20+ markers
Vertebral Hemangioma
- Vertical striations ("corduroy cloth") or honeycomb coarsened trabecular pattern on X-ray
- Typical location: vertebral body
- Usually incidental; symptomatic lesions may be treated
10. Blue Cell Tumors - Imaging Comparison (Mnemonic: LERNM - "Learn 'em")
| Tumor | Age | Imaging Features |
|---|---|---|
| Lymphoma | >30 | Plain film: minimal bone destruction; MRI: massive soft tissue mass out of proportion |
| Ewing sarcoma | <30 | Plain film: onion-skinning + Codman triangle; MRI: massive soft tissue mass |
| Rhabdomyosarcoma | <30 | Plain film: normal; MRI: soft tissue mass |
| Neuroblastoma | <30 | Plain film: normal; MRI: soft tissue mass |
| Myeloma | >30 | Plain film: punched-out lesions, no host response; MRI: lesion with small edema halo |
- Miller's Review of Orthopaedics 9th Edition
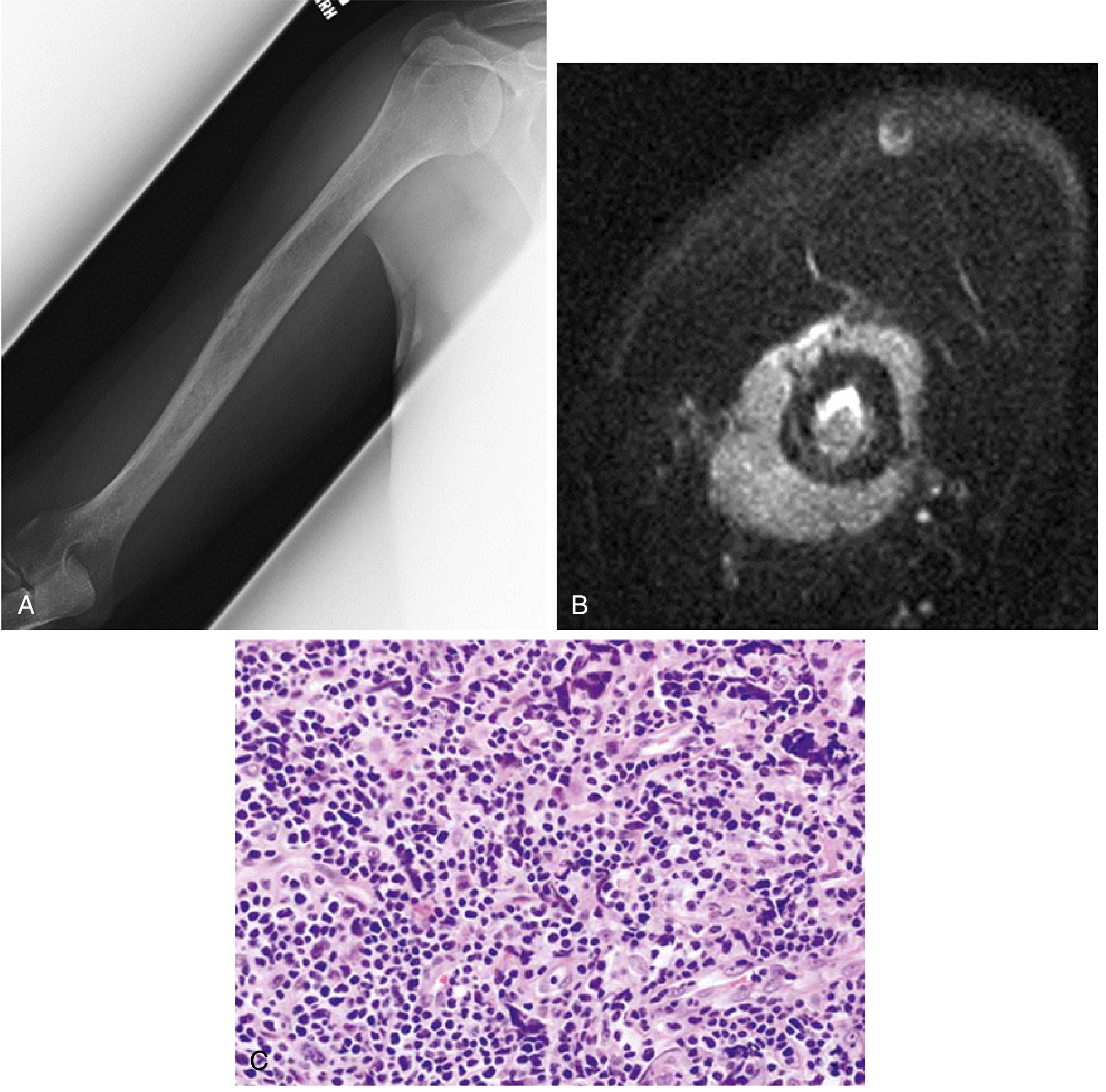
Lymphoma of bone - illustrating the classic imaging triad (X-ray showing lytic diaphyseal lesion, MRI T2 showing massive soft tissue extension, histology showing small blue cells):
11. Staging of Bone Sarcomas (Enneking / AJCC)
| Stage | Tumor | Grade | Metastasis |
|---|---|---|---|
| IA | T1 (≤8 cm) | Low grade (G1/G2) | None |
| IB | T2 (>8 cm) | Low grade | None |
| IIA | T1 | High grade (G3/G4) | None |
| IIB | T2 | High grade | None |
| III | T3 (discontinuous in same bone) | Any | None |
| IVA | Any | Any | Lung |
| IVB | Any | Any | Other distant sites / LN |
Note: Ewing sarcoma is always classified G4 (undifferentiated - high grade).
- Harrison's Principles of Internal Medicine 22E
12. Summary Algorithm
Bone lesion detected
↓
Plain X-ray (2 views) → Apply Lodwick, assess periosteum, matrix, location, age
↓
Is it likely benign? ──Yes──> CT to confirm (enchondroma, osteochondroma, bone island)
↓ No
MRI of entire bone → Extent of medullary involvement, soft tissue mass, skip lesions
↓
Tc-99m bone scan → Polyostotic disease? Skip lesions?
↓
CT chest/abdomen/pelvis or PET/CT → Metastatic staging
↓
Biopsy (guided by imaging, through single compartment, longitudinal incision)
Key rule for biopsy: Always include the soft tissue component of a bone tumor in the biopsy specimen (avoids creating a stress riser/fracture in an already compromised bone). Culture the specimen to exclude infection.
Sources:
- Grainger & Allison's Diagnostic Radiology, Chapter 40 (Bone Tumors)
- Miller's Review of Orthopaedics 9th Ed., Section 9 (Musculoskeletal Oncology)
- Harrison's Principles of Internal Medicine 22E, Chapter 96 (Bone Sarcomas)
- Rockwood & Green's Fractures in Adults 10th Ed., Chapter on Infection and Bone Tumor Workup
- Campbell's Operative Orthopaedics 15th Ed., Chapters 10, 11, 23, 83
This is a shared conversation. Sign in to Orris to start your own chat.