Note on temporalis muscle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a structured note on the temporalis muscle, drawn from Gray's Anatomy for Students and K.J. Lee's Essential Otolaryngology.
Temporalis Muscle
Location
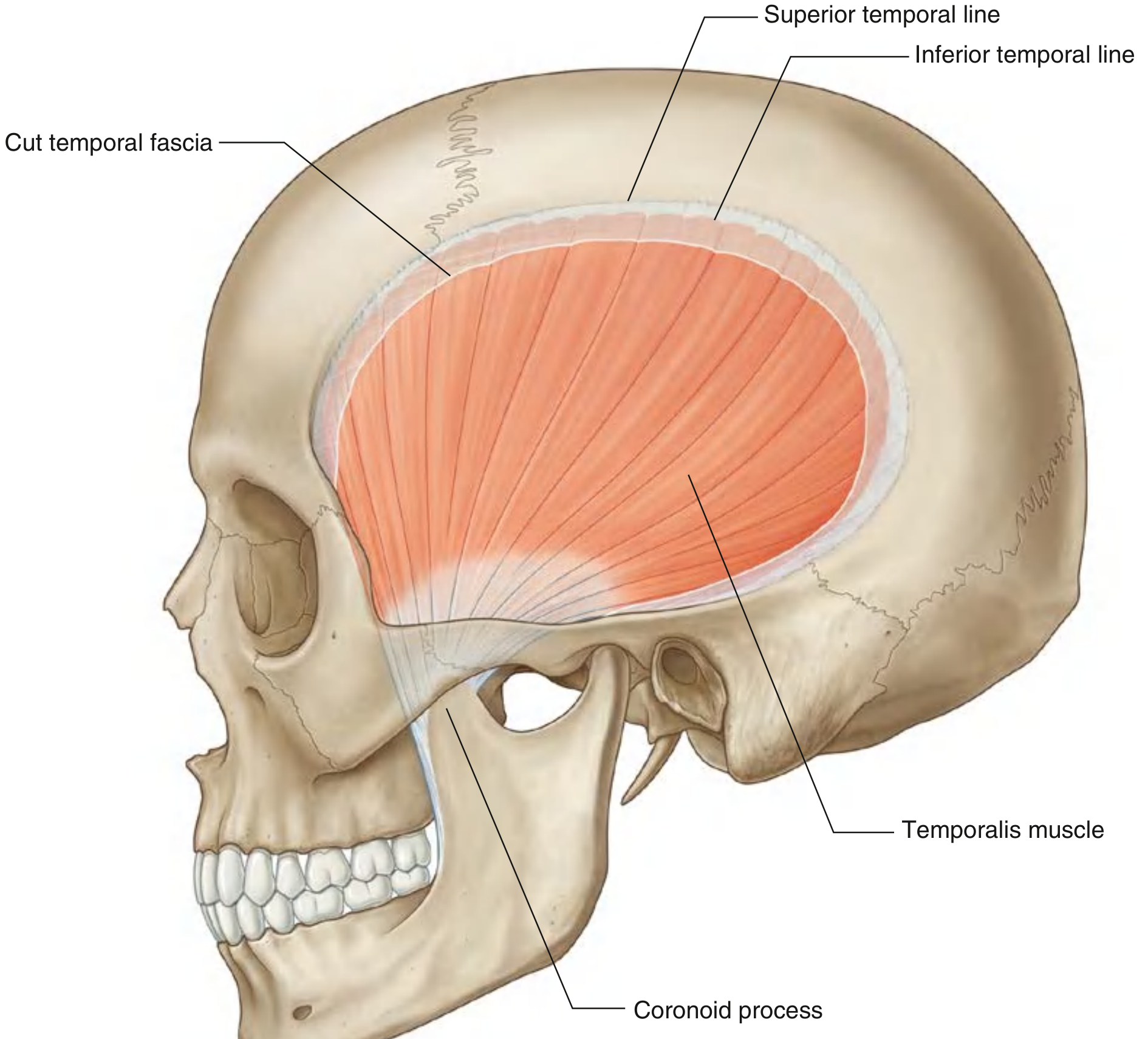
The temporalis is a large, fan-shaped muscle that fills much of the temporal fossa on the lateral aspect of the skull. It is the major structure occupying that fossa.
Attachments
| Detail | |
|---|---|
| Origin | Bony floor of the temporal fossa, from the inferior temporal line superiorly, and from the deep surface of the temporal fascia laterally. Origin spans the parietal bone, frontal bone, and superior temporal surface of the sphenoid bone. |
| Insertion | Coronoid process of the mandible and the anterior margin of the ramus of the mandible, extending down almost to the level of the last molar tooth. |
The fibers converge inferiorly to form a tendon that passes deep to the zygomatic arch (between the zygomatic arch and the infratemporal crest of the greater wing of the sphenoid) before inserting on the coronoid process.
Fiber orientation:
- Anterior fibers - run vertically
- Posterior fibers - run horizontally
Actions
- Elevation of the mandible (jaw closure) - the primary and most powerful action
- Retraction of the mandible - pulls the mandible posteriorly (the posterior horizontal fibers are responsible for this)
- Side-to-side (grinding) movements of the mandible - participates in mastication
Nerve Supply
- Deep temporal nerves - usually two in number, from the anterior trunk of the mandibular nerve (CN V3) in the infratemporal fossa
- They pass superiorly, around the infratemporal crest of the greater wing of the sphenoid, and enter the temporal fossa deep to the temporalis muscle
Blood Supply
- Deep temporal arteries (usually two) - branches of the maxillary artery; travel with the deep temporal nerves; anastomose with the middle temporal artery
- Middle temporal artery - branch of the superficial temporal artery, arising just above the root of the zygomatic arch; penetrates the temporal fascia, passes under the margin of the temporalis, and runs superiorly on the deep surface of the muscle
Coverings
The temporalis is enclosed by the temporal fascia, a strong fibrous layer attached superiorly to the superior temporal line and splitting inferiorly to attach to the medial and lateral surfaces of the zygomatic arch.
Relations
- Medially: skull, including the pterion (the thinnest part - clinically important in head trauma)
- Laterally: temporal fascia
- Inferiorly: zygomatic arch
- Opens medially to the infratemporal fossa (through which the tendon passes to insert on the coronoid process)
- The zygomaticotemporal nerve (branch of V2) passes between the bone and the muscle and pierces the temporal fascia to supply skin of the temple
Clinical Relevance
- Temporalis flap (regional muscle transfer): The temporalis is commonly used in reconstructive surgery - strips of muscle (and deep temporal fascia) can be rotated over the zygomatic arch and inset at the oral commissure to restore dynamic facial reanimation in facial palsy (Gillies procedure/orthodromic temporalis transfer). A drawback is temporal hollowing and increased midfacial bulk.
- Trismus: Spasm or fibrosis of the temporalis (along with masseter and pterygoids) restricts mouth opening - seen after radiation, infection, or trauma.
- Temporal arteritis (Giant Cell Arteritis): Involves the superficial temporal and middle temporal arteries in close proximity to this muscle - may cause jaw claudication from ischemia of the temporalis.
- Temporal lobe herniation: Because the pterion overlies the middle meningeal artery, trauma here can cause an extradural hematoma - the temporalis muscle is retracted during pterional craniotomy.
Sources: Gray's Anatomy for Students, p. 1118-1120; K.J. Lee's Essential Otolaryngology, p. 664
This is a shared conversation. Sign in to Orris to start your own chat.