
Interpret
Patient & Specimen Info
- Patient: Male, 24 years old (DOB 20.07.2001)
- Sample collected: 02.05.2026 at 12:40
- Laboratory: INVITRO-Kazakhstan, Semey
Result-by-Result Interpretation
| Parameter | Result | Reference | Interpretation |
|---|---|---|---|
| Color | Light yellow | — | Normal |
| Clarity | Full (clear) | — | Normal |
| Relative density | 1033 | 1003–1035 | Upper end of normal — urine is well-concentrated; could indicate dehydration or reduced fluid intake |
| pH | 5.0 | 4.5–8.0 | Within range, but on the acidic side — common with high-protein diet, dehydration, or early morning sample |
| Protein | Negative | Negative | Normal — no proteinuria |
| Glucose | Negative | Negative | Normal — no glucosuria |
| Ketone bodies | Negative | Negative | Normal |
| Urobilinogen | Negative | Negative | Normal |
| Leukocyte esterase | Negative | Negative | No signs of infection/inflammation |
| Bilirubin | Negative | Negative | Normal |
| Hemoglobin | Negative | Negative | No hematuria or hemoglobinuria |
| Nitrites | Negative | Negative | No bacterial infection suggested |
| Squamous epithelium | Not detected | < 3/hpf | Normal |
| Transitional epithelium | Not detected | < 1/hpf | Normal |
| Renal epithelium | Not detected | Absent | Normal — no renal tubular damage |
| WBCs (micro) | 3 | < 2/hpf | Mildly elevated — borderline; could be normal variant, slight irritation, or contamination |
| RBCs (micro) | Not detected | Absent | Normal |
| Casts | Not detected | Absent | Normal |
| Salts | Not detected (comment) | — | Uric acid crystals in moderate amount — see below |
| Mucus | See comment | Trace | Small amount — generally insignificant |
| Bacteria | Not detected | Absent | Normal |
| Yeast | Not detected | Absent | Normal |
Key Findings & Clinical Significance
1. Uric Acid Crystals (moderate amount) ⚠️
- Hyperuricosuria — excess uric acid in the urine
- Dehydration — concentrated, acidic urine favors uric acid precipitation (note: SG 1033, pH 5.0)
- High-purine diet (red meat, organ meats, shellfish, alcohol)
- Risk factor for uric acid kidney stones if persistent
- May warrant checking serum uric acid level and assessing for gout if symptomatic
2. High Specific Gravity (1033)
3. Acidic pH (5.0)
4. Borderline Leukocytes (3/hpf; reference < 2)
- Sample contamination
- Mild urethral irritation
- Normal biological variation
Summary
Overall, this is a near-normal urinalysis in a healthy 24-year-old male. The primary finding is moderate uric acid crystalluria in concentrated, acidic urine, which is most consistent with dehydration and possibly a high-purine diet. There is no evidence of infection, proteinuria, hematuria, or kidney disease.
Recommendations
- Increase fluid intake significantly (2.5–3 L of water/day)
- Reduce purine-rich foods (organ meats, red meat, shellfish, alcohol, fructose-sweetened drinks)
- Repeat urinalysis in 2–4 weeks after dietary/hydration changes
- Consider checking serum uric acid if crystals persist or if there are joint symptoms
- The mildly elevated WBCs alone do not require antibiotic treatment
Im a doing gym so i take 5g creatinine and eat chicken every 3rd day two times
creatine supplementation urine specific gravity crystalluria
How Your Gym Lifestyle Explains the Results
Creatine (5g/day) — Direct Connection
- Creatine pulls water into muscle cells — this means less free water available for urine, making your urine more concentrated
- This directly explains your high specific gravity (1033) and acidic pH (5.0)
- Concentrated + acidic urine = ideal conditions for uric acid crystals to form — this is almost certainly why you have the uric acid crystals
Chicken (high-protein diet)
- High in purines → broken down into uric acid → excreted in urine → more uric acid crystals
- High protein → shifts urine pH more acidic, further promoting crystal formation
- Combined with creatine's dehydrating effect, this is a double driver of your uric acid crystals
The Real Issue: You're Likely Underdrinking
| Factor | Effect on Urine |
|---|---|
| Creatine (5g/day) | Draws water into muscles → concentrated urine |
| High-protein diet (chicken) | Increases uric acid + acidifies urine |
| Gym training (sweating) | Further water loss |
| Result | SG 1033, pH 5.0, uric acid crystals |
What You Should Do
Water Intake — this is the fix
- At 5g creatine/day + gym training, you need at least 3–4 liters of water per day
- General gym rule: 500ml extra per hour of training, on top of baseline 2.5L
- If your urine is dark yellow, you're not drinking enough
Diet Tweaks (minor)
- Chicken is fine — keep eating it. Just make sure you're drinking enough water alongside it
- No need to stop creatine — it's safe, just increase water with it
What You Don't Need to Worry About
- Your kidneys look completely healthy — no protein, no blood, no casts, no bacteria
- The WBCs (3/hpf) are not a UTI — no nitrites, no leukocyte esterase
- Uric acid crystals in an otherwise healthy young male who trains and takes creatine is very common and benign when hydration is optimized
Bottom Line
Your urinalysis is normal for a 24-year-old gym-goer on creatine. The uric acid crystals are almost certainly caused by insufficient water intake relative to your activity level + creatine use + protein intake. Drink more water — 3–4L/day — and repeat the test in a month. Everything should normalize.
Case #1. Community-Acquired Pneumonia Patient M., 34 years old, presents with complaints of fever up to 39.2 °C, cough with rust-colored sputum, dyspnea on exertion, and right-sided chest pain that worsens with breathing. Symptoms have been present for 3 days. The patient self-administered paracetamol with no improvement. Medical history: no chronic conditions; penicillin allergy denied; no hospitalization in the past 2 weeks. Physical examination: RR 22/min, SpO₂ 95%, HR 98/min, BP 120/80 mmHg. Auscultation reveals crepitation in the lower right lung field with increased tactile fremitus. Chest X-ray: infiltration of the right lower lobe. PSI severity index — Class II. Complete blood count: WBC 14.2 × 10⁹/L, band neutrophils 18%, ESR 42 mm/h. Sputum culture: results expected in 48–72 hours.
Case #1 — Community-Acquired Pneumonia (CAP)
1. Diagnosis
Diagnostic reasoning:
| Finding | Significance |
|---|---|
| Fever 39.2°C, 3-day history | Acute infectious process |
| Rust-colored sputum | Classic for Streptococcus pneumoniae (pneumococcal pneumonia) |
| Right-sided pleuritic chest pain | Pleural involvement/irritation |
| RR 22/min, SpO₂ 95% | Mild respiratory compromise |
| Crepitations + ↑ tactile fremitus, right lower lobe | Consolidation |
| CXR: right lower lobe infiltrate | Confirms lobar consolidation |
| WBC 14.2 × 10⁹/L, bands 18%, ESR 42 mm/h | Significant bacterial inflammatory response |
| No hospitalization in past 2 weeks | Rules out hospital-acquired pneumonia |
2. Severity Assessment
PSI/PORT Class II
CURB-65 cross-check:
| Criterion | Patient | Score |
|---|---|---|
| Confusion | No | 0 |
| Urea >7 mmol/L | Not reported | 0 (assume normal) |
| RR ≥30/min | RR 22 — No | 0 |
| BP <90/60 | BP 120/80 — No | 0 |
| Age ≥65 | 34 years — No | 0 |
3. Treatment Plan
Setting: Outpatient (ambulatory)
This patient's profile:
- Previously healthy, 34 years old
- No chronic cardiopulmonary disease
- No antibiotics in the past 3 months
- No MRSA/Pseudomonas risk factors
- No penicillin allergy
First-line antibiotic options (per Fishman's Pulmonary & Rosen's Emergency Medicine):
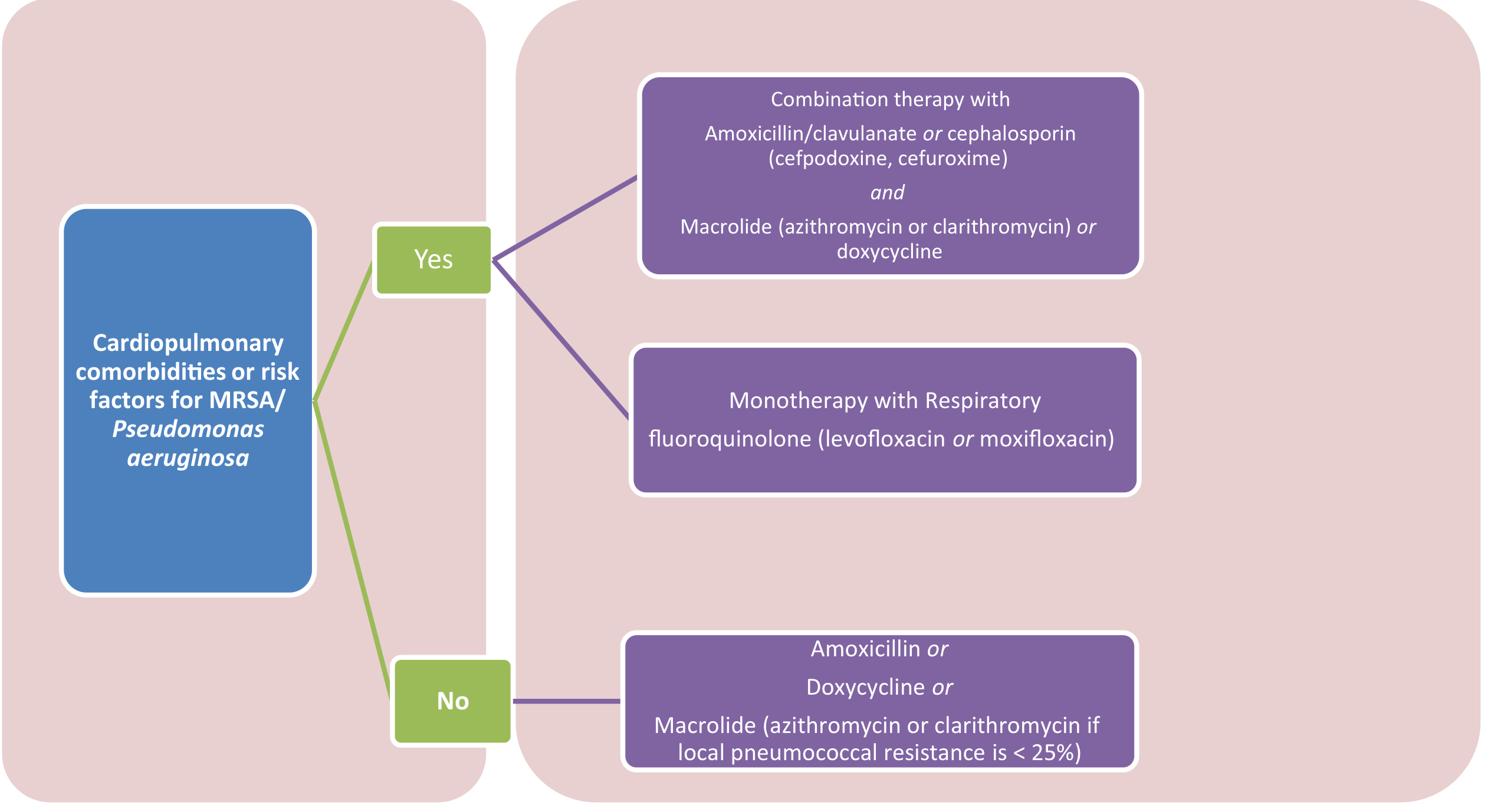
| Option | Regimen | Duration |
|---|---|---|
| Preferred | Amoxicillin 1 g PO three times daily | 5–7 days |
| Alternative | Doxycycline 100 mg PO twice daily | 5–7 days |
| Alternative (if macrolide resistance <25%) | Azithromycin 500 mg day 1, then 250 mg days 2–5 | 5 days |
⚠️ Macrolide monotherapy is no longer recommended unless local pneumococcal resistance is <25% — Rosen's Emergency Medicine.
Note on rust-colored sputum: This strongly suggests pneumococcal etiology. Amoxicillin (β-lactam) is the best targeted choice for S. pneumoniae and is the guideline-preferred first-line agent for low-risk outpatient CAP.
Supportive care:
- Antipyretic/analgesic: Continue paracetamol; add ibuprofen for pleuritic pain if no contraindications
- Hydration: Encourage oral fluids
- Activity: Rest; avoid strenuous activity until afebrile
- Supplemental O₂: Not required outpatient (SpO₂ 95% at rest); advise to return if dyspnea worsens
4. Monitoring & Follow-Up
| Timepoint | Action |
|---|---|
| 24–48 hours | Phone follow-up — check for fever resolution, worsening dyspnea |
| 48–72 hours | Review sputum culture results; de-escalate or adjust antibiotics if needed |
| Day 3–5 | Clinical reassessment — if no improvement, consider hospitalization and broadened coverage |
| 4–6 weeks | Repeat CXR to confirm radiologic resolution (especially important in adults >40 to exclude underlying malignancy) |
Criteria for hospitalization (escalate if any develop):
- RR ≥30/min or SpO₂ drops below 92%
- New confusion
- BP <90/60 mmHg
- No clinical improvement at 72 hours on antibiotics
5. When Sputum Culture Returns (48–72 h)
- If S. pneumoniae confirmed: continue amoxicillin (optimal)
- If atypical pathogen (Mycoplasma, Chlamydophila): switch to doxycycline or azithromycin
- If resistant organism: adjust per sensitivity report
Summary
This is a 34-year-old healthy male with PSI Class II lobar CAP, most likely pneumococcal given rust-colored sputum and lobar consolidation. Outpatient treatment with amoxicillin 1 g TID × 5–7 days is appropriate, with close follow-up at 48–72 hours and repeat CXR at 4–6 weeks. No hospitalization is required at this stage.
Treatment plan
Treatment Plan — CAP, PSI Class II, Outpatient
Patient Profile Recap
- 34-year-old male, previously healthy
- No comorbidities, no penicillin allergy, no recent antibiotics
- No hospitalization in past 2 weeks
- No MRSA / Pseudomonas risk factors
I. Antibiotic Therapy
First-Line (Recommended)
- Targets the most likely pathogen (S. pneumoniae — strongly suggested by rust-colored sputum + lobar consolidation)
- β-lactam monotherapy is now guideline-preferred for low-risk outpatient CAP without comorbidities
- Oral bioavailability is sufficient; IV not needed
Alternatives (if amoxicillin unavailable or not tolerated)
| Alternative | Dose | Duration | Notes |
|---|---|---|---|
| Doxycycline | 100 mg PO BID | 5–7 days | Good if atypical co-infection suspected |
| Azithromycin | 500 mg day 1, then 250 mg days 2–5 | 5 days | Only if local pneumococcal macrolide resistance <25% |
| Levofloxacin | 750 mg PO once daily | 5 days | Reserve — use if β-lactam fails or comorbidities present |
⚠️ Macrolide monotherapy is no longer recommended as routine first-line due to rising pneumococcal resistance.
II. Symptomatic / Supportive Treatment
| Symptom | Treatment |
|---|---|
| Fever | Paracetamol 500–1000 mg PO every 6 hours as needed (patient already using — continue) |
| Pleuritic chest pain | Ibuprofen 400 mg PO TID with food (if no contraindications) |
| Dyspnea | Rest; no supplemental O₂ needed at home at SpO₂ 95%, but escalate if it drops |
| Hydration | Oral fluids ≥2 L/day — supports mucociliary clearance and recovery |
| Activity | Rest until afebrile for 24–48 hours; avoid exertion |
| Cough | Productive cough should not be suppressed — aids expectoration |
III. Monitoring Schedule
| When | What to Check |
|---|---|
| 24–48 h | Fever trend, dyspnea, tolerability of antibiotics (phone/telehealth) |
| 48–72 h | Review sputum culture — adjust antibiotics if needed |
| Day 3 | If no clinical improvement → admit and broaden coverage |
| 4–6 weeks | Repeat CXR — confirm radiologic resolution; exclude underlying lesion |
IV. Red Flags — Indications to Hospitalize Immediately
- SpO₂ < 92% at rest
- RR ≥ 30/min
- New confusion or altered mental status
- BP < 90/60 mmHg
- Inability to take oral medications
- No improvement after 72 hours of outpatient antibiotics
V. Antibiotic De-escalation at 48–72 h (Sputum Culture)
| Culture Result | Action |
|---|---|
| S. pneumoniae (sensitive) | Continue amoxicillin — optimal |
| Mycoplasma / Chlamydophila | Switch to doxycycline or azithromycin |
| H. influenzae | Continue amoxicillin or switch to amoxicillin-clavulanate |
| Resistant organism | Adjust per susceptibility report |
| No growth / viral | Reassess — consider stopping antibiotics if clinical picture allows |
Summary Prescription
Amoxicillin 1000 mg PO three times daily × 5–7 days Paracetamol 1000 mg PO every 6 h PRN fever/pain Ibuprofen 400 mg PO TID with food PRN pleuritic pain Oral fluids ≥2 L/day, rest Follow-up in 48–72 hours; repeat CXR at 4–6 weeks