Frank Sterling Law. Bernoulli's principle. Venturi principle. And anesthesia relevance.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have everything I need for a thorough, well-illustrated answer. Here it is:
Frank-Starling Law, Bernoulli's Principle, Venturi Principle, and Anesthesia Relevance
1. Frank-Starling Law
Physiology
The Frank-Starling law (also called Starling's law of the heart) states that the stroke volume ejected by the ventricle is directly proportional to its end-diastolic volume (EDV). In simpler terms: the more the heart fills during diastole, the more forcefully it contracts in systole.
Historical basis:
- Otto Frank (German physiologist): described the relationship between systolic pressure developed in a frog ventricle and its pre-systolic volume.
- Ernest Starling (British physiologist): demonstrated in an isolated dog heart that the volume ejected in systole is determined by the end-diastolic volume.
Cellular mechanism:
The underlying basis is the length-tension relationship of cardiac myofilaments. At a sarcomere length of ~2.0-2.2 µm, actin-myosin cross-bridge overlap is optimal and force generation is maximal. Stretching to this length also increases the sensitivity of troponin C to Ca²⁺ (myofilament length-dependent activation) - this is actually the dominant mechanism in cardiac muscle, rather than simple cross-bridge overlap as in skeletal muscle.
"An increase in end-diastolic volume is the equivalent of an increase in myocardial stretch; therefore, according to the Frank-Starling law, increased stroke volume is generated." - Miller's Anesthesia, 10e
The Frank-Starling Curve
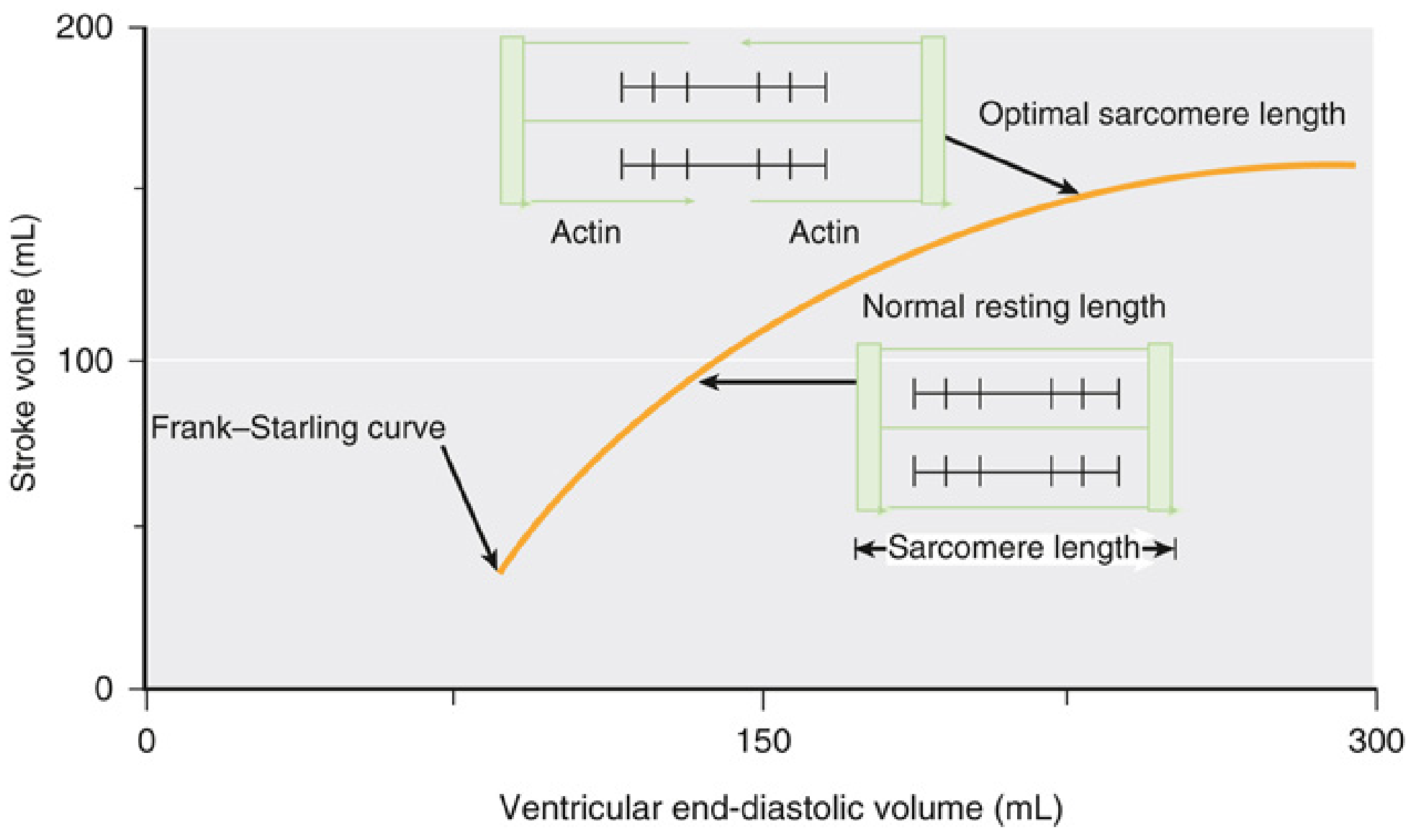
- As venous return (preload) increases → EDV increases → sarcomeres stretch → more cross-bridge overlap → greater stroke volume.
- In the physiologic range, the relationship is nearly linear. At very high EDV, the curve flattens (the ventricle cannot keep up indefinitely).
- Note: Unlike skeletal muscle, cardiac muscle does NOT show a descending limb under physiologic conditions.
Family of Frank-Starling Curves (Contractility)
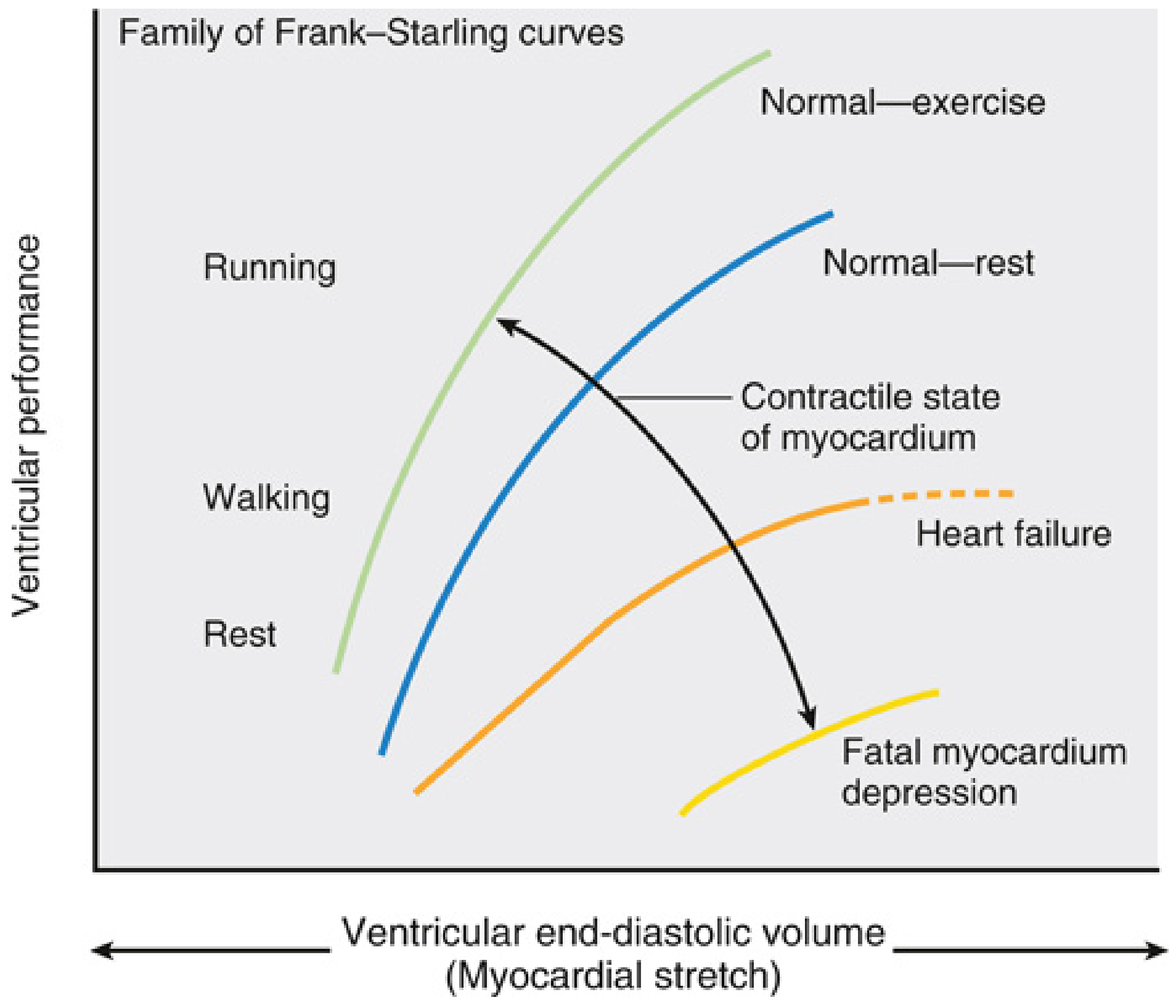
Each curve represents a different inotropic state (contractility):
- Leftward/upward shift = increased contractility (exercise, sympathetic stimulation, catecholamines, digoxin, milrinone) - higher stroke volume for same EDV
- Rightward/downward shift = decreased contractility (heart failure, acidosis, hypoxia, volatile anesthetics, beta-blockers)
Key formula link: Stroke Volume (SV) × Heart Rate (HR) = Cardiac Output (CO). Frank-Starling governs SV.
Anesthesia Relevance - Frank-Starling
| Clinical Scenario | Frank-Starling Implication |
|---|---|
| Volume loading / fluid resuscitation | Moves patient up the ascending curve; exploits preload-dependence |
| Hemorrhage / hypovolemia | Left shift on curve; reduced EDV → reduced SV → reduced CO |
| Volatile anesthetics (e.g., sevoflurane, isoflurane) | Negative inotropy = downward curve shift; also vasodilate → reduce preload and afterload |
| Head-down (Trendelenburg) position | Increases venous return → increases EDV → augments SV via Frank-Starling |
| Positive pressure ventilation (IPPV) | Reduces venous return → decreases RV preload; potential to reduce SV |
| Heart failure patients | Curve is flattened and rightward; patients are preload-dependent; aggressive fluid removal risks falling off the plateau |
| Inotropes (dobutamine, milrinone) | Shift curve up and left; increase SV at the same preload |
| Echocardiographic preload assessment (TEE) | LVEDA (left ventricular end-diastolic area) or LVEDD used intraoperatively to estimate preload; determines where patient sits on the Starling curve |
"The Frank-Starling mechanism may remain intact even in a failing heart. However, ventricular remodeling after injury or in heart failure may modify the Frank-Starling relationship." - Miller's Anesthesia, 10e
The Frank-Starling principle also underpins dynamic indices of fluid responsiveness (SVV, PPV): a cyclically preloaded ventricle with positive pressure ventilation demonstrates variation in SV if it is operating on the steep (preload-dependent) portion of the curve.
2. Bernoulli's Principle
Physics
Bernoulli's principle is a statement of conservation of energy in flowing fluids (derived from the Bernoulli equation):
Total mechanical energy per unit volume = Pressure energy + Kinetic energy + Potential energy = constant
For a horizontal tube (ignoring gravity):
P + ½ρv² = constant
Where:
- P = lateral (static) pressure
- ρ = fluid density
- v = flow velocity
Consequence: Where a tube narrows and velocity increases, lateral pressure decreases. When the tube widens again, velocity falls and pressure is restored (the energy conversion is reversible).
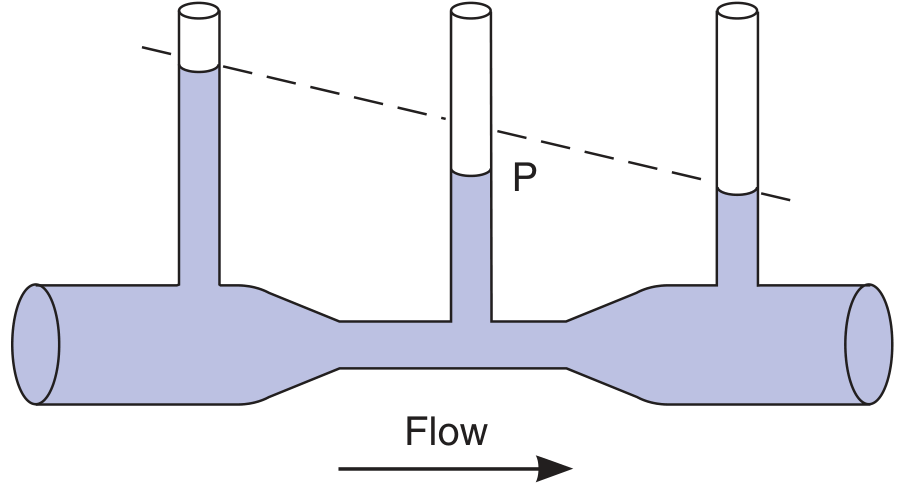
The dashed line shows what pressure drop due to friction alone would look like in a uniform tube. The extra pressure drop at the constriction is due to kinetic energy conversion - and it is recovered as the tube widens.
Pathophysiologic relevance
- Atherosclerotic stenosis: As blood accelerates through a narrowed lumen, lateral distending pressure falls. This can cause the weakened wall to be "sucked inward," maintaining or worsening the stenosis.
- Nasal valve: The nasal valve is the narrowest segment of the nasal airway; rapid airflow here creates the lowest lateral pressure, predisposing to dynamic collapse (relevant in nasal surgery and OSA).
- Korotkoff sounds in blood pressure measurement reflect turbulent flow at the brachial artery as cuff pressure is released.
Simplified Bernoulli Equation in Echocardiography
The modified (simplified) Bernoulli equation is one of the most important clinical applications:
ΔP = 4V²
where V = peak velocity (in m/s) measured by continuous-wave Doppler, and ΔP = pressure gradient (in mmHg).
Assumptions for simplification:
- Flow acceleration and viscous friction terms are negligible
- Density of blood ≈ constant (ρ/2 ≈ 4)
- Proximal velocity (V₁, e.g., LVOT velocity) is <1 m/s and contributes minimally
Example: A jet velocity of 4 m/s across the aortic valve = ΔP of 4 × 4² = 64 mmHg - indicating severe aortic stenosis.
"The Bernoulli equation (pressure change = 4V²) allows echocardiographers to determine the pressure gradient between areas of different velocities." - Morgan & Mikhail's Clinical Anesthesiology, 7e
Anesthesia Relevance - Bernoulli
| Application | Detail |
|---|---|
| Intraoperative TEE | Modified Bernoulli equation used to calculate pressure gradients across stenotic valves (aortic stenosis, mitral stenosis, RVOT), regurgitant jets, and intracavitary pressures (e.g., RV systolic pressure from TR jet) |
| TR jet → RVSP | If TR peak velocity = 3 m/s, RVSP = 4(3²) + RAP = 36 + RAP; used to estimate pulmonary artery pressures non-invasively |
| Aortic stenosis grading pre-op | Peak gradient from Bernoulli guides risk stratification and surgical planning |
| HOCM (dynamic LVOT obstruction) | Bernoulli applied to LVOT gradient; deepening anesthesia, avoiding tachycardia, maintaining preload avoids worsening obstruction |
| Airway resistance | Turbulent flow at airway constrictions increases pressure drop; supports use of heliox (low-density gas) in upper airway obstruction |
Limitation: The simplified equation is NOT valid for tandem (serial) stenoses, because the proximal velocity approaching the second stenosis is no longer negligible.
3. Venturi Principle (Venturi Effect)
Physics
The Venturi effect is a practical consequence of Bernoulli's principle. When a fluid flows through a constriction (a Venturi tube), velocity increases and lateral pressure drops below atmospheric. This negative pressure (sub-atmospheric) at the constriction can entrain a second fluid (gas or liquid) through a side port.
Structure of a Venturi device:
- Converging section → fluid accelerates
- Throat (minimum diameter) → maximum velocity, minimum pressure
- Diverging section → fluid decelerates, pressure partially recovers
The key insight is: kinetic energy at the throat creates a partial vacuum that sucks in entrained fluid.
Anesthesia Applications - Venturi
a) Venturi Oxygen Masks (Air-Entrainment Masks)
Fixed FiO₂ masks use a Venturi device at the O₂ inlet. A high-velocity O₂ jet passes through a narrow orifice → creates negative pressure → entrains a precise amount of room air through side ports. The size of the side port orifice determines the entrainment ratio and thus the delivered FiO₂.
| Colour (UK coding) | FiO₂ | O₂ flow (L/min) |
|---|---|---|
| Blue | 0.24 | 2 |
| White | 0.28 | 4 |
| Yellow | 0.35 | 8 |
| Red | 0.40 | 10 |
| Green | 0.60 | 15 |
"Venturi masks can deliver sub-100% FiO₂ mixtures by entraining room air, though its use should be avoided if drapes are present over the patient's face due to entrainment of gases." - Barash Clinical Anesthesia, 9e
b) Jet Ventilation (High-Frequency Jet Ventilation)
"During inspiration (1-2 s), a high-pressure (30-50 psi) jet of oxygen is directed through the glottic opening and entrains a mixture of oxygen and room air into the lungs (Venturi effect)." - Morgan & Mikhail's Clinical Anesthesiology, 7e
Used in:
- Microlaryngoscopy and panendoscopy (where an ETT obstructs the surgical field)
- Laser airway surgery
- Tracheal resection and reconstruction
- High-frequency jet ventilation (80-300 breaths/min) via tracheal cannula
Mechanism: A high-velocity O₂ jet entrains room air via Venturi effect, inflating the lungs. Expiration is passive. Adequate expiratory time must be allowed to prevent air-trapping.
Caveat: Capnography is unreliable during jet ventilation because alveolar gas is constantly diluted.
c) Anesthesia Machine Ventilators
"Some anesthesia machines reduce oxygen consumption by incorporating a Venturi device that draws in room air to provide air/oxygen pneumatic power." - Morgan & Mikhail's Clinical Anesthesiology, 7e
In double-circuit bellows ventilators, if pure oxygen is used as the driving gas, the ventilator consumes oxygen at a rate equal to or greater than minute ventilation (potentially 6+ L/min extra). Incorporating a Venturi device allows room air to be entrained, reducing O₂ consumption from the central supply.
d) Nebulizers
Small-volume nebulizers in the breathing circuit use the Venturi principle: a high-velocity gas jet entrains liquid medication from a reservoir, atomizing it into an aerosol for delivery.
e) Suction/Ejector Devices
Venturi-based suction devices (e.g., surgical aspirators, Yankauer suction) use a high-pressure gas flow to create entrainment and negative pressure for aspiration.
Summary Comparison Table
| Principle | Core Statement | Key Formula | Primary Anesthesia Applications |
|---|---|---|---|
| Frank-Starling Law | Stroke volume ∝ end-diastolic volume (preload) | SV increases with EDV; curve shifts with contractility | Fluid management, hemodynamic monitoring (TEE/LVEDA), inotrope titration, heart failure care, fluid responsiveness indices (SVV/PPV) |
| Bernoulli's Principle | In flowing fluid, ↑ velocity → ↓ lateral pressure; total energy is conserved | P + ½ρv² = const; simplified: ΔP = 4V² | Doppler/TEE pressure gradient calculations (valve stenosis, TR jet, RVSP, HOCM), airway physics |
| Venturi Principle | High-velocity jet through a constriction creates sub-atmospheric pressure that entrains a second fluid | Entrainment ratio determined by orifice geometry and jet velocity | Venturi O₂ masks (fixed FiO₂), jet ventilation (panendoscopy, laser airway), anesthesia machine pneumatics, nebulizers |
Sources:
- Costanzo Physiology, 7e - Frank-Starling Relationship, pp. 161-178
- Miller's Anesthesia, 10e - Contractility and Frank-Starling, pp. 1377-1379
- Ganong's Review of Medical Physiology, 26e - Bernoulli principle and blood pressure, p. 578
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Bernoulli/TEE, Venturi jet ventilation, Venturi in anesthesia machines, pp. 209-210, 1471
- Barash Clinical Anesthesia, 9e - Venturi masks in airway fire safety, p. 2686
This is a shared conversation. Sign in to Orris to start your own chat.