Parkisons disease definition etiology epidemology clinical features short pathology with reference
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Parkinson disease"[MeSH Terms] AND "epidemiology"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
I now have all the content needed to write a thorough response. Let me compile the comprehensive answer.
Parkinson's Disease
Definition
Parkinson's disease (PD) is a chronic, progressive neurodegenerative disorder characterized by a hypokinetic movement disorder resulting from loss of dopaminergic neurons in the substantia nigra pars compacta of the midbrain. It is the most common cause of the clinical syndrome of parkinsonism, which is defined by the four cardinal signs: tremor, rigidity, akinesia (bradykinesia), and postural instability. PD was first described by James Parkinson in 1817 in his "Essay on the Shaking Palsy."
"Parkinson disease (PD) is a neurodegenerative disease marked by a hypokinetic movement disorder due to loss of dopaminergic neurons from the substantia nigra."
- Robbins & Kumar Basic Pathology
Epidemiology
- PD is the second most common neurodegenerative disorder after Alzheimer's disease.
- Occurs in approximately 1 in 1,000 in the general population.
- Affects at least 1% of persons older than 65 years.
- Over 10 million people worldwide are affected.
- Men are affected more often than women (ratio approximately 3:2; men 1.5x more likely).
- Symptoms typically emerge between 55 and 65 years of age.
- The prevalence is increasing as the global population ages; age-adjusted mortality from PD increased by 2.4% per year between 1999 and 2019.
- Goldman-Cecil Medicine, 26th Edition
- Guyton and Hall Textbook of Medical Physiology
Etiology
The cause of PD is believed to be a variable combination of genetic and environmental factors. Known genetic causes account for only about 10% of cases, so environmental triggers are also likely.
Genetic Factors
| Gene / Locus | Inheritance | Notes |
|---|---|---|
| LRRK2 (leucine-rich repeat kinase 2) | Autosomal dominant | Most common cause of inherited PD |
| α-synuclein gene - point mutations, duplications, triplications | Autosomal dominant | α-synuclein is the chief constituent of Lewy bodies |
| Parkin, DJ1, PINK1 | Autosomal recessive | Typically early-onset parkinsonism |
| Glucocerebrosidase (GBA) mutations | Risk factor | Associated with higher dementia rates and faster progression |
| PARK10 haplotype (chromosome 1) | Risk factor | Strongly associated with PD |
Environmental Factors
- Pesticides and heavy metals (e.g., manganese) - increased risk with chronic exposure
- MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) - a neurotoxin that selectively destroys dopaminergic neurons in the substantia nigra; MPTP is oxidized to MPP+, a selective inhibitor of mitochondrial Complex I, implicating oxidative stress.
- Traumatic brain injury severe enough to require emergency care
- Possible environmental trigger entry via the enteric nervous system or olfactory pathway (Braak hypothesis)
Pathogenetic Mechanisms
- Oxidative stress
- Mitochondrial dysfunction
- Protein misfolding and aggregation (α-synuclein)
- Defective autophagy and lysosomal degradation (parkin, PINK1 pathway)
- Excitotoxicity and apoptotic cell death
- Neuroinflammation
- Goldman-Cecil Medicine; Adams and Victor's Principles of Neurology, 12th Edition
Pathology
Gross Findings
- Pallor of the substantia nigra (loss of the normal dark pigmentation from neuromelanin-containing dopaminergic neurons) - seen on gross midbrain sectioning.
- Pallor of the locus ceruleus also observed.
Microscopic Findings
- Loss of pigmented dopaminergic neurons in the substantia nigra pars compacta, with accompanying reactive gliosis.
- Approximately 60% of these neurons must be lost before classic motor symptoms develop.
- Lewy bodies - the pathological hallmark:
- Single or multiple cytoplasmic, eosinophilic, round to elongated inclusions in remaining neurons
- Ultrastructurally composed of fine filaments of α-synuclein, neurofilaments, and ubiquitin
- Also found in the sympathetic ganglia, locus ceruleus, and dorsal motor nucleus of the vagus
- Lewy neurites - dystrophic neurites that also contain aggregated α-synuclein.
Figure: Lewy body in a nigral neuron (H&E stain)
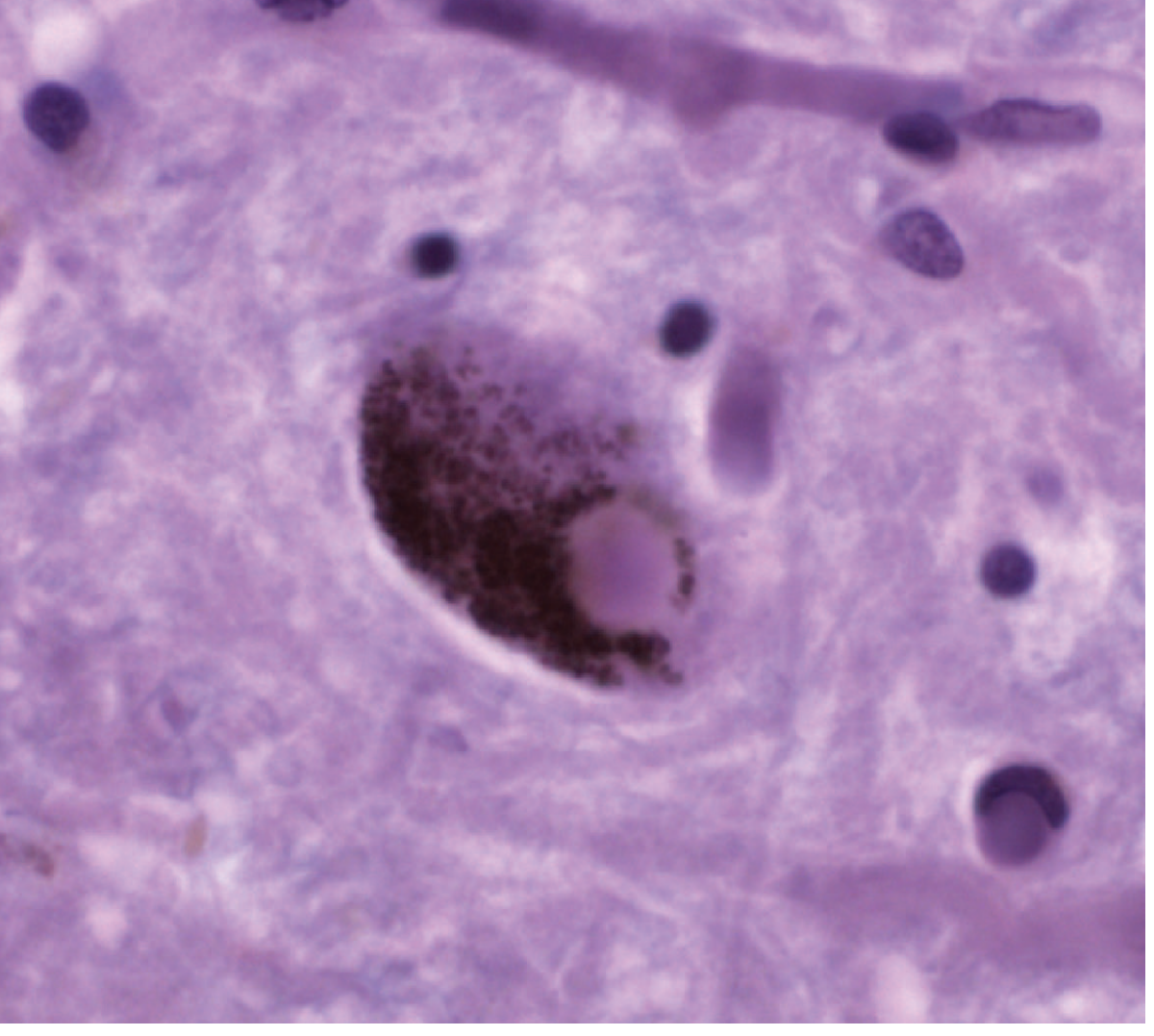
Photomicrograph of a round Lewy body inclusion in the cytoplasm of a nigral neuron (H&E staining). - Adams and Victor's Principles of Neurology, 12th Ed.
Neurochemical Pathology
- Decreased dopamine in the neostriatum (especially putamen) due to loss of the nigro-striatal pathway.
- Dopamine is normally an inhibitory transmitter in the caudate and putamen; its loss leads to overactivity of the striatum, producing continuous excitatory output to the corticospinal motor system.
- Abnormal β-oscillatory activity in the motor cortex and basal ganglia underlies bradykinesia.
Braak Staging (Hypothesis)
The earliest pathological changes may begin in:
- Dorsal vagal nucleus and anterior olfactory nuclei (explaining early premotor symptoms like anosmia and autonomic dysfunction)
- Lower brainstem nuclei (locus ceruleus, raphe)
- Substantia nigra (classical motor symptoms appear)
- Cortex (dementia in late stages)
- Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine; Adams and Victor's Principles of Neurology; Guyton and Hall Textbook of Medical Physiology
Clinical Features
Premotor / Prodromal Phase (Years Before Motor Onset)
These symptoms often precede motor diagnosis by years:
- Anosmia (loss of smell) - one of the earliest signs
- REM sleep behavioral disorder (RBD) - acting out dreams, a very specific early marker
- Constipation and other autonomic dysfunction
- Depression and anxiety
- Restless leg syndrome
Cardinal Motor Features ("TRAP")
| Feature | Description |
|---|---|
| Tremor | Resting "pill-rolling" tremor, 4-6 Hz; subsides with voluntary movement; accentuated by stress; present in upper limbs during walking |
| Rigidity | Increased muscle tone on passive joint movement; "cogwheel" (with tremor superimposed) or "lead pipe" (without tremor) |
| Akinesia/Bradykinesia | Slowness, reduced amplitude, fatigue, interruptions in movement |
| Postural instability | Flexed "stooped" posture; impaired righting reflexes; propulsion (forward), retropulsion (backward); falls |
Note: Classic resting tremor occurs in only about 1 in 5 patients at presentation.
Features of Bradykinesia (Clinical Manifestations)
- Hypomimia / masked facies (reduced facial expression, "reptilian stare")
- Hypophonia (soft, monotonous speech)
- Micrographia (small, cramped handwriting)
- Sialorrhea (drooling - from impaired swallowing)
- Reduced arm swing, shuffling gait, shortened stride
- Freezing of gait (sudden arrest in ongoing movement)
- Difficulty turning in bed, rising from a chair
Non-Motor Features (Progress with Disease)
- Pain and sensory disturbances
- Autonomic dysfunction: orthostatic hypotension, urinary urgency/frequency, constipation, erectile dysfunction
- Depression and anxiety
- Cognitive disturbances: mild cognitive impairment progressing to dementia (up to 80% of patients will eventually develop dementia)
- Psychosis: visual hallucinations (often drug-related)
- Sleep disturbances: REM sleep behavior disorder, insomnia
Disease Course
- Typically progresses over 10 to 15 years, leading to severe motor slowing and near-immobility.
- Asymmetric onset is characteristic and often persists into later stages.
- Death often results from aspiration pneumonia or trauma from falls.
- Goldman-Cecil Medicine, 26th Ed.; Robbins & Kumar Basic Pathology; Guyton and Hall Textbook of Medical Physiology; Bradley and Daroff's Neurology in Clinical Practice
Summary Table
| Feature | Details |
|---|---|
| Definition | Progressive neurodegenerative disorder; loss of dopaminergic neurons in substantia nigra pars compacta |
| Etiology | Genetic (~10%) + environmental; LRRK2, α-synuclein, parkin; pesticides, MPTP |
| Epidemiology | 2nd most common neurodegeneration; 1% >65 yrs; men > women (3:2); >10 million worldwide |
| Pathology | Pallor of SN; Lewy bodies (α-synuclein); nigral cell loss + gliosis; Braak staging |
| Cardinal signs | Tremor (resting), Rigidity (cogwheel/lead-pipe), Akinesia/Bradykinesia, Postural instability |
| Premotor | Anosmia, RBD, constipation, depression |
| Non-motor | Autonomic dysfunction, dementia, depression, psychosis |
References
- Goldman-Cecil Medicine, 26th Edition - Chapter 378: Parkinson Disease
- Robbins & Kumar Basic Pathology - Chapter 21: Parkinson Disease
- Adams and Victor's Principles of Neurology, 12th Edition - Chapter 38: Parkinson Disease (Pathology & Pathogenesis)
- Guyton and Hall Textbook of Medical Physiology - Chapter: Basal Ganglia / Parkinson Disease
- Bradley and Daroff's Neurology in Clinical Practice - Chapter 32: Parkinson Disease
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry - Dementia in Parkinson Disease
This is a shared conversation. Sign in to Orris to start your own chat.