Hello My name is Pritam Mistri, I am a 2nd year MBBS student from WBUHS University
Hello Pritam! Welcome. It's great to meet you.
I'm Orris, your AI study assistant. As a 2nd year MBBS student from WBUHS (West Bengal University of Health Sciences), you're likely deep into subjects like:
- Pathology
- Pharmacology
- Microbiology
- Forensic Medicine
- Clinical Postings (Medicine, Surgery, OBG, Pediatrics)
I have access to a rich medical textbook library and can help you with:
- Explaining concepts in any of your subjects
- Diagrams and visual aids
- Clinical correlations
- MCQ-style doubt clearing
- Case-based discussions
- Exam preparation tips
What would you like to study today, Pritam? Feel free to ask anything!
Will you help me to study for my upcoming profesional MBBS exam
Asking for Preferences
Type 3 hypersensitivity
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete, exam-focused breakdown of Type III Hypersensitivity for you, Pritam:
Type III Hypersensitivity - Immune Complex Mediated
Basic Definition
Type III hypersensitivity is caused by the deposition of antigen-antibody (immune) complexes in tissues and vessel walls, leading to complement activation and neutrophil-mediated tissue injury.
- Antibody class involved: IgG (primarily) and IgM
- Not cell-mediated - it is purely antibody + complement driven
Pathogenesis - 3 Sequential Phases
(This is the classic exam sequence from Robbins)
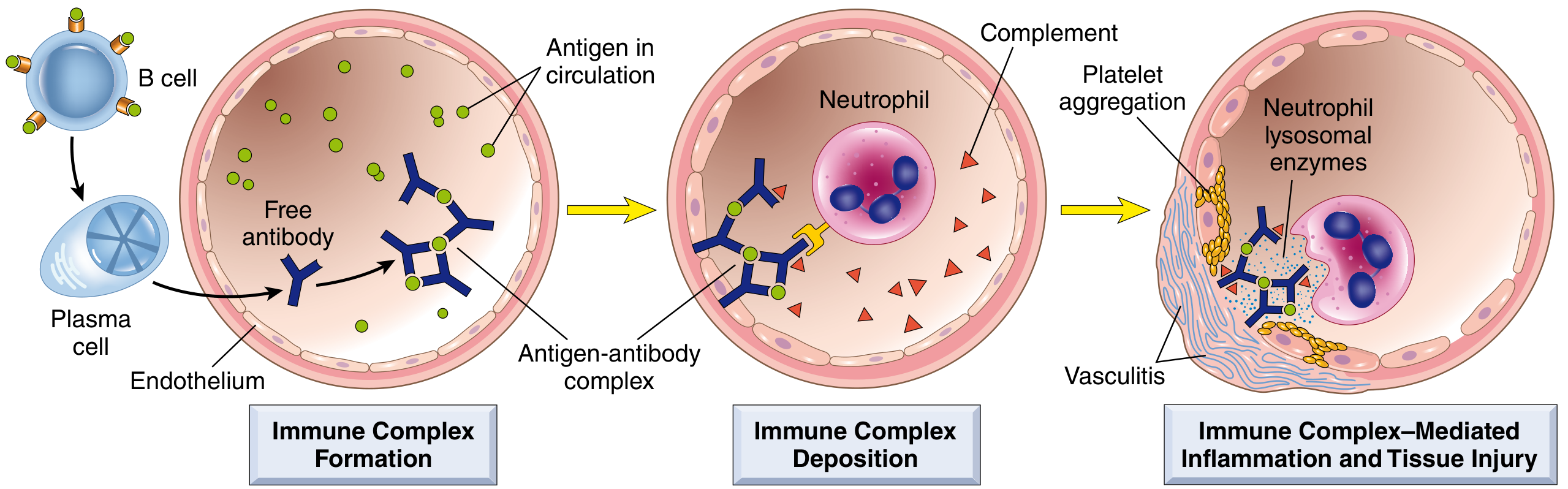
Phase 1 - Formation of Immune Complexes
- Antigen enters the body → stimulates B cells → plasma cells secrete IgG antibodies (~1 week later)
- Antibodies bind circulating antigen → form antigen-antibody (immune) complexes in the blood
Phase 2 - Deposition of Immune Complexes
- Complexes circulate and deposit in vessel walls (or are formed in situ at sites of "planted" antigen)
- Most pathogenic complexes: medium-sized, formed under slight antigen excess
- Preferred deposition sites: kidney (glomeruli), joints, skin, blood vessels - organs where blood is filtered at high pressure
Phase 3 - Inflammation and Tissue Injury
- Deposited complexes activate complement (C3a, C5a = anaphylatoxins)
- C5a is a potent chemoattractant - recruits neutrophils
- Neutrophils try to phagocytose the complexes but cannot (they are fixed in vessel walls) → "frustrated phagocytosis"
- Neutrophils release lysosomal enzymes and reactive oxygen species → tissue destruction
- Platelet aggregation → microthrombi → further ischemia
- Result: Fibrinoid necrosis of vessel walls (smudgy eosinophilic material = necrotic tissue + immune complexes + complement + plasma proteins)
Clinical Features (appear ~10 days after antigen exposure)
- Fever
- Urticaria (hives)
- Joint pain (arthralgia/arthritis)
- Lymph node enlargement
- Proteinuria (glomerular damage)
Important Lab Finding
- Serum C3 levels fall during active disease (complement is consumed)
- Immunofluorescence of kidney biopsy: granular deposits of immunoglobulin + complement = "lumpy-bumpy" pattern
- Electron microscopy: electron-dense deposits along glomerular basement membrane (subendothelial/subepithelial)
Two Forms - HIGH YIELD
| Feature | Systemic Immune Complex Disease | Local (Arthus Reaction) |
|---|---|---|
| Prototype | Serum sickness | Arthus reaction |
| Antigen source | Circulating foreign proteins | Injected intracutaneously into sensitized individual |
| Mechanism | Complexes form in blood, deposit in vessels | Complexes form locally in vessel walls |
| Lesion | Systemic vasculitis, nephritis, arthritis | Localized skin necrosis |
| Time course | ~10 days after first exposure | Hours after re-exposure |
Classic Examples - Must Know for Exams
| Disease | Antigen Involved | Main Manifestation |
|---|---|---|
| SLE | Nuclear antigens (dsDNA, histones) | Nephritis, skin, arthritis |
| Post-streptococcal GN | Streptococcal cell wall antigens | Nephritis |
| Serum sickness | Foreign serum protein (e.g., horse antithymocyte globulin) | Vasculitis, arthritis, nephritis |
| Polyarteritis nodosa | Hepatitis B surface antigen | Systemic vasculitis |
| Reactive arthritis | Bacterial antigens (e.g., Yersinia) | Acute arthritis |
| Arthus reaction | Foreign proteins (experimental) | Cutaneous vasculitis/necrosis |
Comparison of All 4 Hypersensitivity Types - Quick Recap
| Type | Name | Antibody/Cell | Key Molecule | Example |
|---|---|---|---|---|
| I | Anaphylactic | IgE | Mast cells, histamine | Asthma, anaphylaxis |
| II | Cytotoxic | IgG, IgM | Complement/phagocytes | Hemolytic disease, Myasthenia gravis |
| III | Immune Complex | IgG, IgM | Complement + neutrophils | SLE, serum sickness, post-strep GN |
| IV | Delayed (DTH) | None (T cells) | CD4+/CD8+ T cells | TB, contact dermatitis, transplant rejection |
Exam Memory Tips
- "Lumpy-bumpy" = Type III (granular IF pattern in kidney)
- "Linear" = Type II (anti-GBM antibodies in Goodpasture)
- Complement consumption (↓C3) = active Type III disease
- Serum sickness = prototype systemic; Arthus = prototype local
- Medium-sized complexes in slight antigen excess = most pathogenic
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.); Robbins & Kumar Basic Pathology
Do you want me to go deeper into any specific aspect - like SLE as a Type III disease, the complement pathway in detail, or the comparison with Type II hypersensitivity? I can also give you MCQs to test yourself!
Short note on Methotrexate
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I have all the information needed. Here is your complete short note on Methotrexate, exam-ready:
Short Note: Methotrexate (MTX)
Drug Class
Antimetabolite / Folate Antagonist - belongs to the DMARD (Disease-Modifying Anti-Rheumatic Drug) category and is also used as a cytotoxic/anticancer agent.
Mechanism of Action
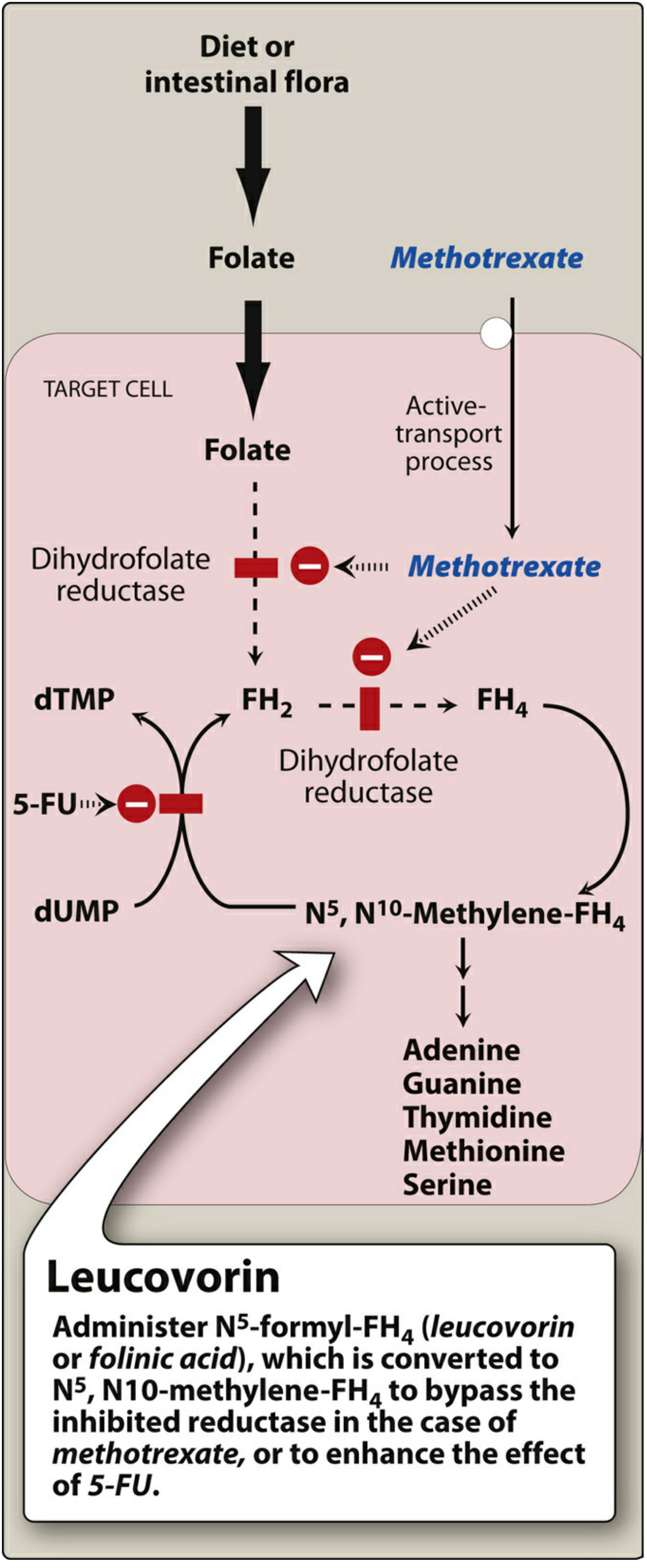
MTX is structurally similar to folic acid. It enters cells via active transport and inhibits dihydrofolate reductase (DHFR) - the enzyme that converts:
Folic acid (FH2) → Tetrahydrofolate (FH4)
- Without FH4, there is no N5,N10-methylene-FH4 available
- This blocks synthesis of: dTMP (thymidine), purines (adenine, guanine), and amino acids (methionine, serine)
- Net result: DNA and RNA synthesis is halted - affecting rapidly dividing cells most
- Cell cycle specific: S phase
- At low (rheumatic) doses, MTX also inhibits AICAR transformylase → accumulation of extracellular adenosine → potent anti-inflammatory effect (suppresses neutrophils, macrophages, lymphocytes)
- MTX is polyglutamated inside cells - retained for prolonged periods = prolonged effect
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Routes | Oral, IV, IM, intrathecal (IT) |
| Oral bioavailability | ~70% (variable at higher doses) |
| Distribution | Intestinal epithelium, liver, kidney; also ascites/pleural effusions |
| BBB penetration | Poor - given intrathecally for CNS malignancy |
| Metabolism | 7-hydroxylation (less water-soluble metabolite - can cause crystalluria) |
| Excretion | Primarily renal (urine) - up to 30% via bile |
| Half-life | 6-9 hours |
Important: Urine must be kept alkaline + patient well-hydrated to prevent crystalluria and renal toxicity.
Therapeutic Uses
Oncology (High-dose MTX)
- Acute Lymphocytic Leukemia (ALL) - most important
- Burkitt lymphoma (children)
- Breast cancer
- Head and neck carcinomas
- Mycosis fungoides
- CNS prophylaxis (intrathecal route)
Non-oncology / Inflammatory Diseases (Low-dose MTX)
- Rheumatoid Arthritis (RA) - anchor drug, 7.5-25 mg/week
- Psoriasis (severe)
- Psoriatic arthritis
- Crohn disease
- SLE, vasculitis, polymyositis, giant cell arteritis
- Juvenile Idiopathic Arthritis (JIA)
- Ectopic pregnancy (IM injection)
Adverse Effects - HIGH YIELD
| System | Effect |
|---|---|
| Bone marrow | Myelosuppression - leukopenia, thrombocytopenia, anemia |
| GI | Nausea, stomatitis (mucositis), GI ulceration - most common |
| Liver | Hepatotoxicity - elevated LFTs; chronic use → hepatic fibrosis/cirrhosis |
| Lung | Pneumonitis / pulmonary fibrosis - hypersensitivity type |
| Kidney | Crystalluria, renal tubular damage (7-OH metabolite) |
| Skin | Alopecia, photosensitivity |
| Teratogenicity | Absolutely contraindicated in pregnancy (Category X) - causes neural tube defects, abortion |
| CNS | Leukoencephalopathy (with high-dose/IT use) |
Leucovorin Rescue - EXAM FAVOURITE
Why needed? In high-dose MTX therapy, toxicity to normal cells is severe.
Leucovorin (Folinic acid = N5-formyl-FH4):
- Bypasses the DHFR block
- Directly replenishes the folate pool
- Rescues normal rapidly dividing cells (GI mucosa, bone marrow) without reversing MTX effect on tumor (given after a timed delay)
- Also given to reduce stomatitis and GI side effects even at low doses
Resistance Mechanisms
- Gene amplification of DHFR gene (cancer cells make more DHFR to overcome inhibition)
- Reduced drug uptake (transporter mutations)
- Impaired polyglutamation
Drug Interactions
- NSAIDs - reduce renal clearance of MTX → increased toxicity
- Probenecid, penicillins - reduce tubular secretion → MTX accumulation
- Folic acid supplements - reduce toxicity but may slightly reduce efficacy by 10-18%
- Hydroxychloroquine - reduces MTX clearance
Contraindications
- Pregnancy (absolute)
- Renal failure (drug accumulates)
- Significant hepatic disease
- Pre-existing myelosuppression
- Active infection
One-Line Summary for Exam
MTX = Folate antagonist → inhibits DHFR → blocks dTMP/purine synthesis → stops DNA replication (S-phase specific). Uses: ALL, RA, psoriasis, ectopic pregnancy. Toxicity: myelosuppression, mucositis, hepatotoxicity, pneumonitis. Antidote: Leucovorin.
Sources: Lippincott Illustrated Reviews - Pharmacology; Katzung's Basic & Clinical Pharmacology (16th ed.)
Want MCQs on Methotrexate, or should we move to another drug or topic, Pritam?
This is a shared conversation. Sign in to Orris to start your own chat.