Adductor canal block
Reading File
Finding Sources
Finding Sources
Searching PubMed
"adductor canal block"[MeSH Terms] AND knee
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have rich, comprehensive content from three authoritative anesthesia textbooks plus key ultrasound and positioning images. Here is the full structured answer:
Adductor Canal Block (ACB)
Overview
The adductor canal block (also called the subsartorial block or saphenous nerve block) is an ultrasound-guided peripheral nerve block that targets sensory nerves within the adductor (Hunter's) canal of the mid-thigh. Its primary appeal is providing effective knee analgesia with minimal quadriceps motor weakness - making it the preferred motor-sparing alternative to the femoral nerve block (FNB) for knee surgery.
Anatomy of the Adductor Canal
The adductor canal is a triangular-shaped aponeurotic tunnel in the medial thigh, bounded by:
- Anterior/roof: sartorius muscle
- Antero-lateral: vastus medialis muscle
- Posterior: adductor longus and adductor magnus muscles
Contents relevant to the block:
| Structure | Role |
|---|---|
| Saphenous nerve | Primary target - purely sensory terminal branch of femoral nerve; supplies knee joint (infrapatellar branches), medial leg, medial ankle |
| Nerve to vastus medialis | Mixed nerve (sensory + motor to VM); important contributor to knee joint pain after TKA |
| Superficial femoral artery (SFA) | Key landmark on ultrasound |
| Superficial femoral vein (SFV) | Lies deep and medial to SFA |
The saphenous nerve runs anterior to the femoral artery within the canal. The nerve to the vastus medialis often lies in a distinct fascial sheath outside the true adductor canal, so a very distal injection may miss it.
The "true" adductor canal location on ultrasound is identified by the medial border of sartorius converging with the medial border of adductor longus, with the vastoadductor membrane forming a double-contour roof of the canal.
Indications
- Total knee arthroplasty (TKA) - preferred block (*ACB or saphenous nerve block)
- Anterior cruciate ligament (ACL) reconstruction
- Knee arthroscopy
- Partial knee arthroplasty
- Bunionectomy / hallux valgus surgery
- Medial ankle and foot procedures (combined with sciatic block)
ACB vs. Femoral Nerve Block
| Feature | Femoral Nerve Block | Adductor Canal Block |
|---|---|---|
| Motor block | Significant quadriceps weakness (up to 80%) | Minimal - motor sparing |
| Analgesia (TKA) | Effective | Comparable to FNB |
| Ambulation Day 1 | Impaired (weakness limits mobility) | Better - patients walk further |
| Fall risk | Higher | Lower |
| Technique | Easier (nerve stim or US) | Requires ultrasound |
| Volume needed | Standard | 10-20 mL (higher volumes risk quad paresis) |
Patients with continuous ACB catheters ambulate further on Day 1 post-TKA than those with either FNB (limited by weakness) or no block (limited by pain). - Morgan and Mikhail's Clinical Anesthesiology, 7e
Patient Position
The patient is supine, with the knee slightly flexed and the thigh in slight external rotation to expose the medial thigh. The leg is extended.
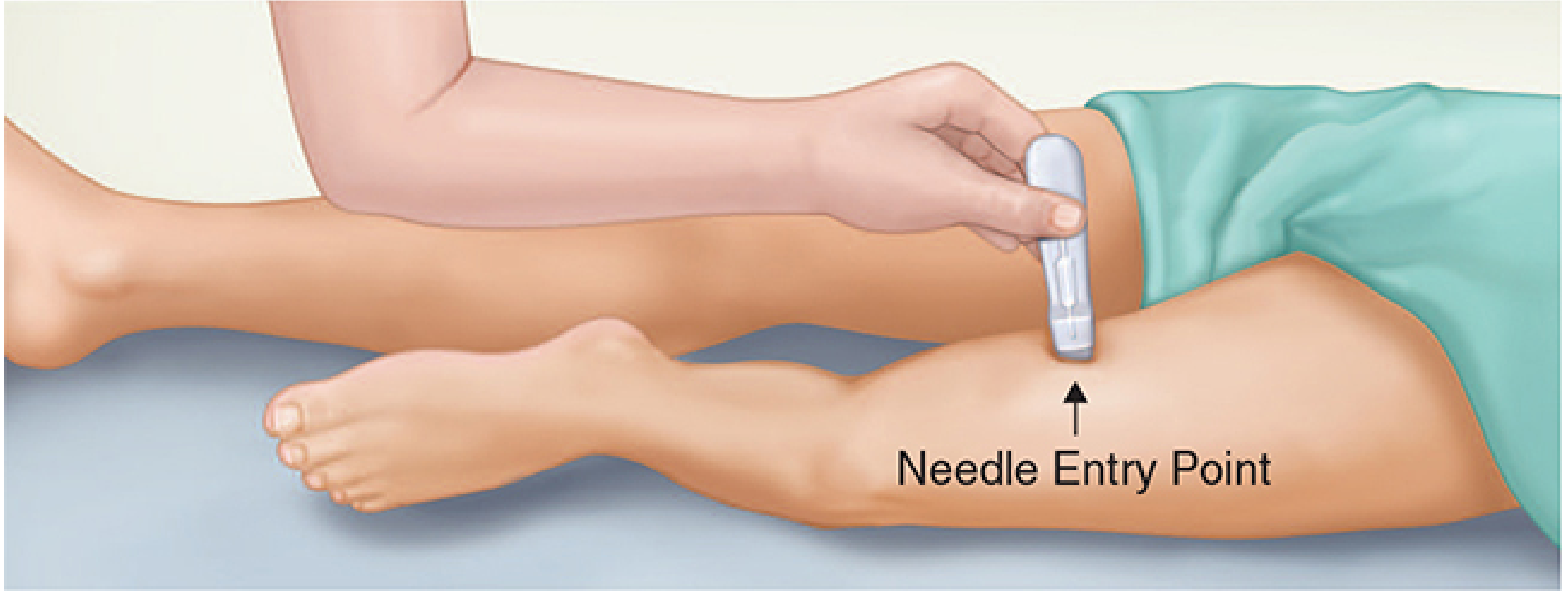
Figure: Patient positioning for ACB with transducer placement at mid-thigh (Morgan and Mikhail, 7e)
Ultrasound-Guided Technique
Probe and Scanning
- Transducer: High-frequency linear probe (short-axis / transverse orientation)
- Starting point: Mid-thigh, approximately halfway between the ASIS and the superior patellar pole (junction of middle and distal thirds of thigh)
- Scan in short axis; identify the sartorius muscle and the subsartorial space
Sonographic Landmarks
The following structures are identified deep to the sartorius:
- SFA (pulsatile, round, compressible artery)
- SFV (medial and deep to SFA)
- Saphenous nerve (small, hyperechoic, anterior/lateral to SFA)
- Vastoadductor membrane (bright fascial band defining the canal roof)
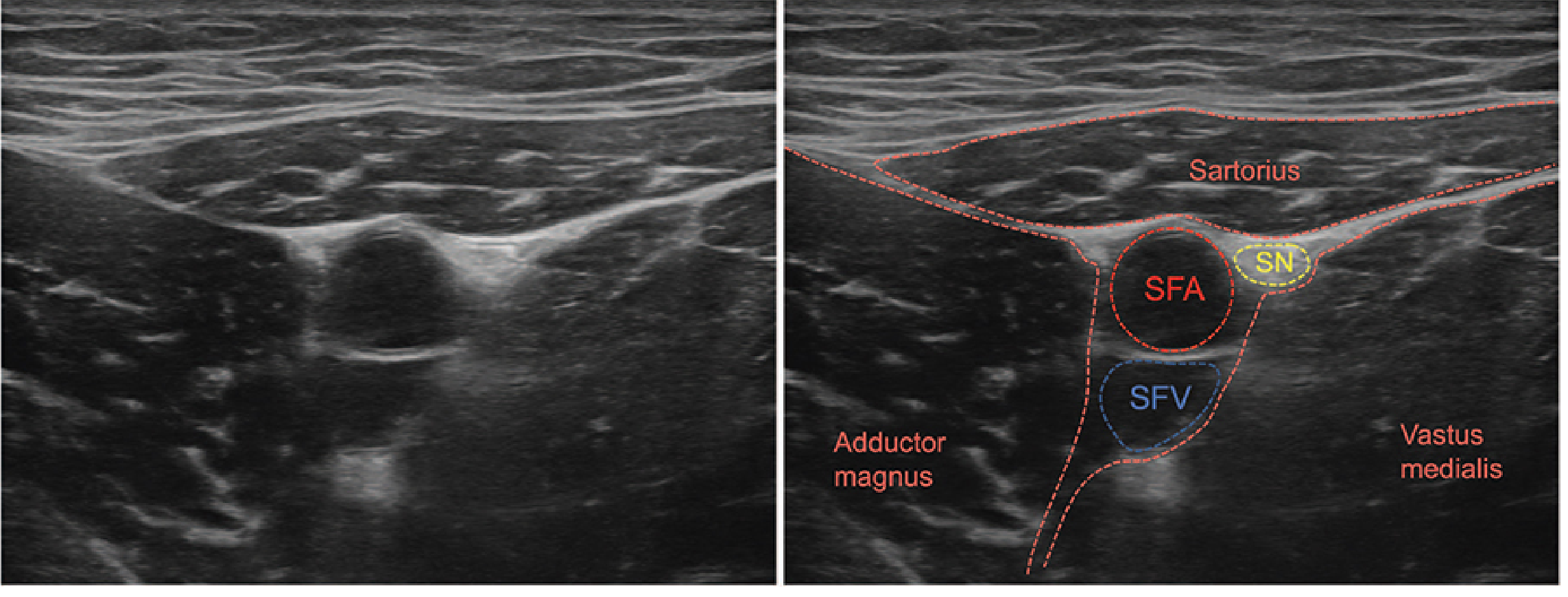
Figure: Short-axis sonoanatomy - SFA = superficial femoral artery, SFV = superficial femoral vein, SN = saphenous nerve (Morgan and Mikhail, 7e)
Needle Technique
- Needle entry: 2-3 cm lateral to the ultrasound transducer
- Advance in-plane from lateral to medial
- Target: the triangular space deep to the sartorius, lateral to the femoral artery, deep to the vastoadductor membrane
- Aspirate to confirm no intravascular placement
- Inject 10-20 mL of local anesthetic (volumes >20 mL risk quadriceps paresis)
- Jaeger et al. advocate a periarterial injection lateral to the femoral artery under the sartorius, midway between ASIS and patella, to cover both the saphenous nerve and nerve to vastus medialis
Note: Nerve stimulation alone or combined with ultrasound can be used. If using nerve stimulation, elicit twitches in the vastus medialis (0.1-0.2 mL/kg of local anesthetic).
Local Anesthetic
- Volume: 10-20 mL (single injection); higher volumes increase risk of motor spread
- Typical agents: 0.25-0.5% bupivacaine or ropivacaine for surgical analgesia; 1.5-2% lidocaine for shorter procedures
- Continuous catheter technique is feasible and provides superior Day 1 analgesia
Nerves Blocked
- Saphenous nerve (always blocked) - sensory to medial knee, medial leg, medial ankle
- Nerve to vastus medialis (variably blocked depending on injection level) - sensory to anterior knee joint; mixed nerve
- Posterior division of the obturator nerve (may be affected)
The block does not cover posterior knee pain. For complete TKA analgesia, ACB is often combined with an IPACK block (infiltration between popliteal artery and posterior capsule of knee) or a tibial nerve block for posterior coverage.
Combination Strategies (for TKA/ACL)
- ACB + IPACK block - covers anterior and posterior knee; motor-sparing combination
- ACB + sciatic nerve block - complete below-knee anesthesia for foot/ankle surgery
- ACB + obturator nerve block - medial knee coverage
- ACB + periarticular infiltration - multimodal analgesia approach
Complications and Side Effects
| Complication | Notes |
|---|---|
| Vascular injury / arterial pseudoaneurysm | Rare; proximity to SFA |
| Intramuscular LA spread / myonecrosis | Severe myonecrosis reported with continuous catheters; unexpected thigh weakness warrants evaluation |
| Residual quadriceps weakness | Possible with high volumes; less than FNB |
| Fall risk | Lower than FNB but not zero; fall-prevention strategies mandatory |
| Block failure | Historical failure rate with landmark-only technique >30%; ultrasound has dramatically reduced this |
Fall prevention is mandatory: Despite being motor-sparing, patients should NOT ambulate unsupported. Patient education is essential. - Miller's Anesthesia, 10e
Key Clinical Pearls
- The correct ACB level is debated - the "true" adductor canal is defined by the convergence of sartorius and adductor longus medial borders on ultrasound
- A block too distal may miss the nerve to vastus medialis (often outside the true canal in a separate fascial sheath), which is a major knee pain contributor after TKA
- Continuous ACB provides the best mobility outcomes after TKA vs. FNB or no block
- ACB is purely analgesic (not anesthetic) for the knee; complete surgical anesthesia requires neuraxial or general anesthesia
- The block can also be called "high saphenous block" or "subsartorial block" in the literature
Sources: Morgan and Mikhail's Clinical Anesthesiology, 7e | Miller's Anesthesia, 10e | Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
This is a shared conversation. Sign in to Orris to start your own chat.